- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
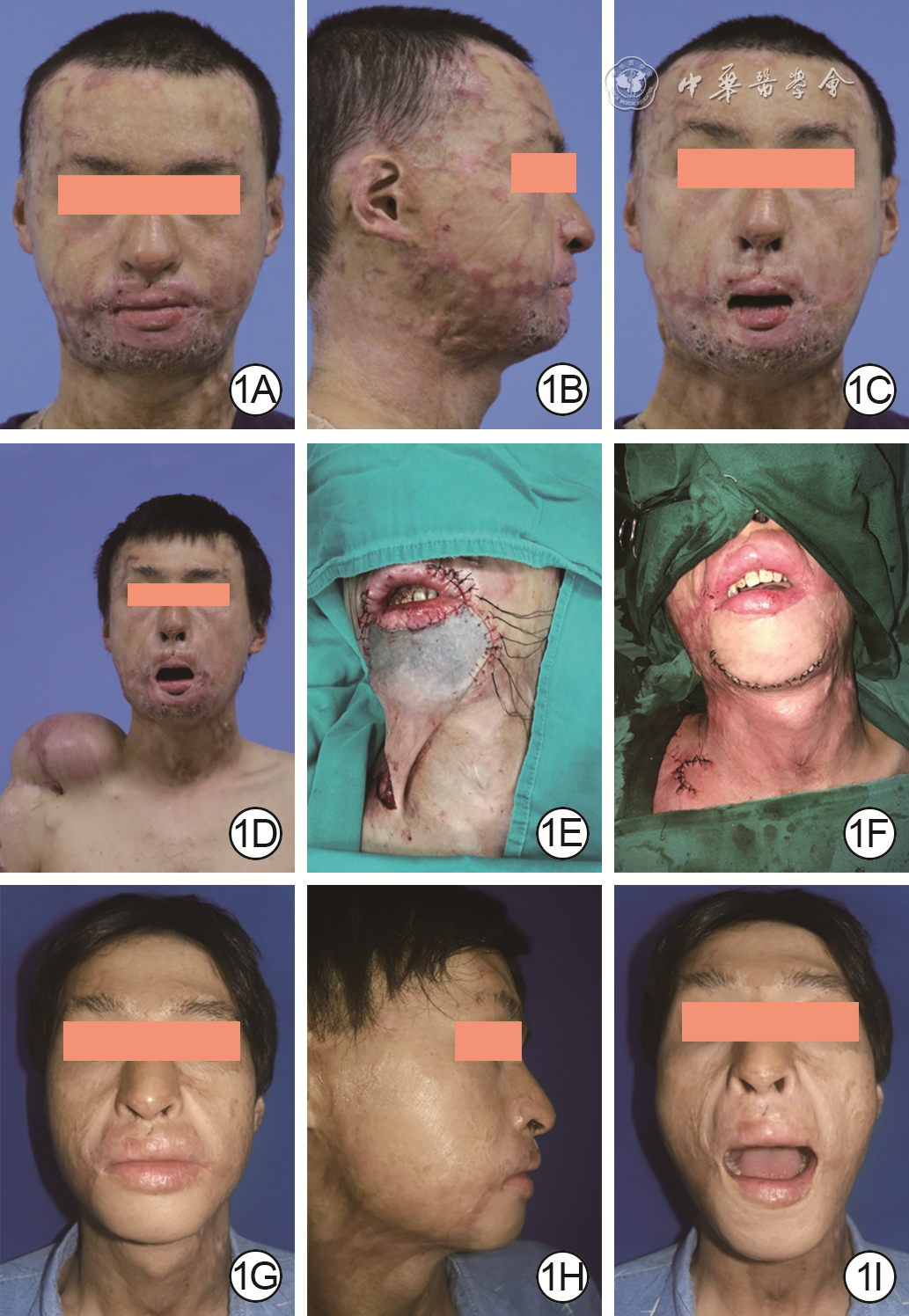
| Citation: | Zhang JP,Yuan X,Jiang XP,et al.Aesthetic reconstruction of the scar contracture deformity in chin and neck with expanded flaps based on the "MRIS" principle[J].Chin J Burns Wounds,2022,38(4):306-312.DOI: 10.3760/cma.j.cn501120-20211130-00401.

|

| [1] |
AkitaS,HayashidaK,TakakiS,et al.The neck burn scar contracture: a concept of effective treatment[J/OL].Burns Trauma,2017,5:22[2022-02-10]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5508764/.DOI: 10.1186/s41038-017-0086-8.
|
| [2] |
Gonzalez-UlloaM.Restoration of the face covering by means of selected skin in regional aesthetic units[J].Br J Plast Surg,1956,9(3):212-221.DOI: 10.1016/s0007-1226(56)80036-2.
|
| [3] |
EdgertonMT,HansenFC.Matching facial color with split thickness skin grafts from adjacent areas[J].Plast Reconstr Surg Transplant Bull,1960,25:455-464.DOI: 10.1097/00006534-196005000-00001.
|
| [4] |
冯少清,苏薇洁,喜雯婧,等.颈部烧伤后瘢痕挛缩畸形的手术策略[J].中华烧伤杂志,2015,31(4):280-284.DOI: 10.3760/cma.j.issn.1009-2587.2015.04.012.
|
| [5] |
LellouchAG,NgZY,PozzoV,et al.Reconstruction of post-burn anterior neck contractures using a butterfly design free anterolateral thigh perforator flap[J].Arch Plast Surg,2020,47(2):194-197.DOI: 10.5999/aps.2019.00591.
|
| [6] |
VinhVQ,Van AnhT,Gia TiênN,et al.Reconstruction of neck and face scar contractures using occipito-cervico-dorsal supercharged "super-thin flaps": a retrospective analysis of 82 cases in Vietnam[J].Burns,2018,44(2):462-467.DOI: 10.1016/j.burns.2017.07.020.
|
| [7] |
TsaiFC,YangJY,ChuangSS,et al.Combined method of free lateral leg perforator flap with cervicoplasty for reconstruction of anterior cervical scar contractures: a new flap[J].J Reconstr Microsurg,2002,18(3):185-190.DOI: 10.1055/s-2002-28470.
|
| [8] |
李青峰.关注面颈部重建治疗理念和技术的转变[J].中华整形外科杂志,2015,31(1):1-3.DOI: 10.3760/cma.j.issn.1009-4598.2015.01.001.
|
| [9] |
GaoY,LiH,GuB,et al.Postburn neck contracture: principles of reconstruction and a treatment algorithm[J].J Reconstr Microsurg,2018,34(7):514-521.DOI: 10.1055/s-0038-1641724.
|
| [10] |
陈建武,马显杰,郭树忠.以颈横动脉分支为蒂的锁骨上皮瓣和颈段皮支皮瓣的区别与联系[J].中华整形外科杂志,2018,34(3):239-242.DOI: 10.3760/cma.j.issn.1009-4598.2018.03.019.
|
| [11] |
赵思纯,王佳琦.扩张轴型皮瓣修复面颈部烧伤瘢痕的基础研究进展和临床应用[J].世界最新医学信息文摘,2018,18(30):45-47.DOI: 10.19613/j.cnki.1671-3141.2018.30.020.
|
| [12] |
韩军涛,王洪涛,李军,等.预扩张胸三角皮瓣修复面颈部烧伤瘢痕挛缩畸形的临床效果[J].中华医学美学美容杂志,2017,23(4):229-231.DOI: 10.3760/cma.j.issn.1671-0290.2017.04.005.
|
| [13] |
唐银科,楚菲菲,丁健科,等.颈部瘢痕挛缩治疗方案的优化选择及临床效果分析[J].中国美容整形外科杂志,2021,32(11):644-646,665.DOI: 10.3969/j.issn.1673-7040.2021.11.002.
|
| [14] |
OgawaR.Surgery for scar revision and reduction: from primary closure to flap surgery[J/OL].Burns Trauma,2019,7:7[2022-02-10]. https://pubmed.ncbi.nlm.nih.gov/30891462/.DOI: 10.1186/s41038-019-0144-5.
|
| [15] |
ZhangY,XiaoW,NgS,et al.Infrared thermography-guided designing and harvesting of pre-expanded pedicled flap for head and neck reconstruction[J].J Plast Reconstr Aesthet Surg,2021,74(9):2068-2075.DOI: 10.1016/j.bjps.2020.12.102.
|
| [16] |
中国整形美容协会瘢痕医学分会.瘢痕早期治疗全国专家共识(2020版)[J].中华烧伤杂志,2021,37(2):113-125.DOI: 10.3760/cma.j.cn501120-20200609-00300.
|
| [17] |
丁架月,朱薛锋,官剑.强脉冲光联合自黏性软聚硅酮敷料早期干预手术瘢痕的临床效果[J].中华医学美学美容杂志,2019,25(3):250-251.DOI: 10.3760/cma.j.issn.1671-0290.2019.03.022.
|
| [18] |
KimJC,KangSY,KimHO,et al.Efficacy of combined treatment with intense pulsed light and fractional erbium:YAG laser in scar prevention: a randomized split wound trial[J].Dermatol Ther,2021,34(5):e15061.DOI: 10.1111/dth.15061.
|
| [19] |
WangJ,WuJ,XuM,et al.A comprehensive reconstruction strategy for moderate to severe faciocervical scar contractures[J].Lasers Med Sci,2021,36(6):1275-1282.DOI: 10.1007/s10103-020-03178-w.
|
Figures(2) / Tables(1)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad:
