



Comparative study of three scores in predicting the death risk of severe burn patients
-
摘要:
目的 探讨改良Baux评分、比利时烧伤预后评分、Ryan评分对严重烧伤患者死亡风险的预测价值,并进行对比研究。 方法 采用回顾性病例系列研究方法。2018年2月—2019年11月,南昌大学第一附属医院烧伤科收治260例符合入选标准的严重烧伤患者,其中男158例、女102例,年龄36(3,53)岁。根据最终结局,将患者分为存活组(229例)和死亡组(31例),比较2组患者入院时性别、年龄、烧伤原因、烧伤部位、烧伤总面积、烧伤深度、合并吸入性损伤情况、合并基础疾病情况,以及根据前述部分资料计算的改良Baux评分、比利时烧伤预后评分、Ryan评分,对数据进行χ2检验或Mann-Whitney U检验。采用Kendall tau-b系数法对260例严重烧伤患者前述3种评分结果进行一致性分析。分别绘制前述3种评分预测260例严重烧伤患者死亡风险的受试者操作特征曲线(ROC),计算曲线下面积(AUC)及最佳阈值与最佳阈值下的敏感度、特异度。采用Delong检验对前述3种评分AUC的质量进行比较。 结果 2组患者性别、烧伤部位、烧伤深度均相近(P>0.05);死亡组患者年龄、烧伤总面积、火焰烧伤比例、合并吸入性损伤比例、合并基础疾病比例均明显大于存活组(Z值分别为5.53、7.18,χ2值分别为16.23、15.89、17.78,P<0.01);死亡组患者改良Baux评分、比利时烧伤预后评分、Ryan评分分别为142(115,155)、7(5,7)、2(2,3)分,均明显高于存活组的64(27,87)、1(0,3)、0(0,1)分(Z值分别为7.91、7.64、7.61,P<0.01)。在260例严重烧伤患者中,改良Baux评分与Ryan评分、改良Baux评分与比利时烧伤预后评分、Ryan评分与比利时烧伤预后评分结果均具有显著一致性(Kendall tau-b系数分别为0.75、0.71、0.86,P<0.01)。改良Baux评分、比利时烧伤预后评分、Ryan评分对260例严重烧伤患者死亡风险预测的ROC的AUC分别为0.92、0.89、0.85(95%置信区间分别为0.86~0.98、0.83~0.95、0.78~0.93,P<0.01),最佳阈值分别为106.5、4.5、1.5分,最佳阈值下的敏感度分别为88.5%、76.9%、73.1%,最佳阈值下的特异度分别为88.5%、87.2%、86.3%。改良Baux评分与比利时烧伤预后评分的AUC质量相近(z=1.25,P>0.05),均明显优于Ryan评分(z值分别为2.35、2.11,P<0.05)。 结论 改良Baux评分、比利时烧伤预后评分、Ryan评分对严重烧伤患者死亡风险均有较好的预测能力,从临床实践考虑,改良Baux评分更适合作为严重烧伤患者的预后预测工具。 Abstract:Objective To explore the predictive values of the modified Baux score, Belgian Outcome in Burn Injury score, and Ryan score on the death risk of severe burn patients. Methods A retrospective case series study was conducted. From February 2018 to November 2019, 260 severe burn patients who met the inclusion criteria were admitted to the Department of Burns of the First Affiliated Hospital of Nanchang University, including 158 males and 102 females, aged 36 (3, 53) years. According to the final outcome, the patients were divided into survival group (n=229) and death group (n=31). Data of patients were compared and statistically analyzed with chi-square test or Mann-Whitney U test between the two groups, including the gender, age, cause of burn, site of burn, total burn area, depth of burn, combined inhalation injury, and combined underlying diseases on admission, and the modified Baux score, Belgian Outcome in Burn Injury score, and Ryan score calculated based on part of the aforementioned data. The Kendall tau-b coefficient method was used to analyze the consistency of the above-mentioned three scores in 260 severe burn patients. The receiver operating characteristic (ROC) curves of the above-mentioned three scores predicting the death risk of 260 severe burn patients were drawn, and the area under the curve (AUC), the optimal threshold, and the sensitivity and specificity under the optimal threshold were calculated. The quality of AUC of the above-mentioned three scores was compared by Delong test. Results The gender, site of burn, and depth of burn of patients between the two groups were all similar (P>0.05). The age, total burn area, proportion of flame burn, proportion of combined inhalation injury, and proportion of combined underlying diseases of patients in death group were significantly higher than those in survival group (with Z values of 5.53 and 17.78, respectively, χ2 values of 16.23, 15.89, and 17.78, respectively, P<0.01); the modified Baux score, Belgian Outcome in Burn Injury score, and Ryan score of patients in death group were 142 (115, 155), 7 (5, 7), 2 (2, 3), all significantly higher than 64 (27, 87), 1 (0, 3), 0 (0, 1) in survival group (with Z values of 7.91, 7.64, and 7.61, respectively, P<0.01). In 260 severe burn patients, the results between the modified Baux score and Ryan score, modified Baux score and Belgian Outcome in Burn Injury score, Ryan score and Belgian Outcome in Burn Injury score were significantly consistent (with Kendall tau-b coefficients of 0.75, 0.71, and 0.86, respectively, P<0.01). The AUCs of ROC curves of the modified Baux score, Belgian Outcome in Burn Injury score, and Ryan score for predicting the death risk of 260 severe burn patients were 0.92, 0.89, and 0.85, respectively (with 95% confidence intervals of 0.86-0.98, 0.83-0.95, and 0.78-0.93, respectively, P<0.01); the optimal thresholds were 106.5, 4.5, and 1.5 points, respectively; the sensitivity under the optimal threshold were 88.5%, 76.9%, and 73.1%, respectively, and the specificity under the optimal threshold were 88.5%, 87.2%, and 86.3%, respectively. The modified Baux score was similar to Belgian Outcome in Burn Injury score in the AUC quality (z=1.25, P>0.05), which were both significantly better than the AUC quality of Ryan score (with z values of 2.35 and 2.11, respectively, P<0.05). Conclusions The modified Baux score, Belgian Outcome in Burn Injury score, and Ryan score have good ability in predicting the death risk of severe burn patients. From the perspective of clinical practice, the modified Baux score is more suitable as a predictive tool for the prognosis of severe burn patients. -
Key words:
- Burns /
- Prognosis /
- Forecasting
-
烧伤是一种特殊的创伤类型,对烧伤死亡风险的预测有利于优化预检分诊流程、合理分配医疗资源、加强患者风险管理以及调整护理计划[1]。患者因素(性别、年龄、基础疾病)和烧伤因素(烧伤总面积、吸入性损伤、烧伤深度)等都会影响烧伤患者预后[2, 3, 4, 5],其中烧伤面积、年龄和吸入性损伤是临床实践中明确的烧伤致死的3个重要预测因子[6, 7]。有研究者认为,预后预测工具的评估内容应该纳入患者特征和烧伤特征,这样将会更加科学和准确[8]。故现有针对创伤预后的预测工具,如创伤评分、创伤严重程度评分、创伤严重度特征评分和急性生理学和慢性健康状况评价评分等因只涉及创伤因素,均不适合用来预测烧伤患者的预后[9, 10]。查阅文献可知,改良Baux评分、比利时烧伤预后评分、Ryan评分[7,11, 12, 13]这3种烧伤患者预后评分在国外被证实是有效的[14],遗憾的是,上述评分系统的开发和验证多基于发达国家的人口学病历资料,其可靠性在我国尚鲜见报道。本研究旨在探讨改良Baux评分、比利时烧伤预后评分、Ryan评分对我国严重烧伤患者死亡风险的预测效果,并比较何种评分最简便实用,何种评分对临床指导价值最大,以期为国内烧伤患者提供快速、准确的预后评估工具,降低严重烧伤患者的病死率。
1. 对象与方法
1.1 伦理学声明
本回顾性病例系列研究只涉及严格匿名收集的临床记录,在不泄露患者身份的前提下对其病历资料进行分析、使用,并且该研究已获得南昌大学第一附属医院伦理委员会豁免。
1.2 入选标准
纳入标准:(1)住院时间>24 h,已完善各项指标检查者;(2)采用中国新九分法[15]和烧伤分度[16]判定为重度及以上的热力损伤患者。排除标准:(1)病历资料不完整者;(2)有恶性肿瘤合并症者;(3)电击伤、化学烧伤者。
1.3 临床资料和分组统计及质量控制
2018年2月—2019年11月,南昌大学第一附属医院烧伤科收治260例符合入选标准的严重烧伤患者,其中男158例(60.8%),女102例(39.2%),年龄36(3,53)岁。
根据最终结局,将患者分为存活组(229例)和死亡组(31例),比较2组患者以下指标:(1)入院时的一般资料,包括患者的性别、年龄。(2)入院时的疾病相关资料,包括烧伤原因、烧伤部位、烧伤总面积、烧伤深度、合并吸入性损伤情况、合并基础疾病情况。(3)根据前述部分资料计算的改良Baux评分、比利时烧伤预后评分、Ryan评分。改良Baux评分=年龄+烧伤总面积+17×吸入性损伤,其中年龄和烧伤总面积为实际值,吸入性损伤赋值为有=1、无=0;比利时烧伤预后评分=年龄+烧伤总面积+吸入性损伤,其中年龄赋值为<50岁=0分、50~64岁=1分、65~79岁=2分、≥80岁=3分,烧伤总面积赋值为<20%TBSA=0、20%TBSA~39%TBSA=1、40%TBSA~59%TBSA=2、60%TBSA~79%TBSA=3、80%TBSA=4,吸入性损伤赋值为有=3、无=0;Ryan评分涉及3个危险因素,包括年龄≥60岁、烧伤总面积≥40%TBSA和合并吸入性损伤,根据存在危险因素的个数0、1、2、3,分别对应得分为0、1、2、3分。
为减少病例数据收集时出现的信息偏倚,数据采集由2位受过专业数据采集培训的临床护士完成,并采用双人录入的方式汇总。评分由本文第7、8作者独立完成,数据分析由本文第6作者独立进行,即评分者和数据分析者互盲。
1.4 统计学处理
采用MedCalcl 2.7.8.0统计软件与SPSS 23.0统计软件处理数据。计量资料数据均不符合正态分布,以M(Q1,Q3)表示,等级资料数据以频数(百分数)表示,组间比较均行Mann-Whitney U检验;计数资料数据以频数(百分数)表示,组间比较行χ2检验。采用Kendall tau-b系数法对260例严重烧伤患者改良Baux评分、比利时烧伤预后评分、Ryan评分结果进行一致性分析。分别绘制前述3种评分预测260例严重烧伤患者死亡风险的受试者操作特征曲线(ROC),计算曲线下面积(AUC)及最佳阈值与最佳阈值下的敏感度、特异度;采用Delong检验对前述3种评分AUC的质量进行比较。P<0.05为差异有统计学意义。
2. 结果
2.1 2组患者的临床资料与3种评分
2组患者性别、烧伤部位、烧伤深度均相近(P>0.05),死亡组患者年龄、烧伤总面积、火焰烧伤比例、合并吸入性损伤比例、合并基础疾病比例均明显大/高于存活组(P<0.01)。见表1。死亡组患者改良Baux评分、比利时烧伤预后评分、Ryan评分的得分分别为142(115,155)、7(5,7)、2(2,3)分,均明显高于存活组的64(27,87)、1(0,3)、0(0,1)分(Z值分别为7.91、7.64、7.61,P<0.001)。
表1 2组严重烧伤患者一般资料比较组别 例数 性别[例(%)] 年龄[岁,M(Q1,Q3)] 烧伤原因[例(%)] 烧伤部位[例(%)] 男 女 火焰 其他 1处 ≥2处 存活组 229 139(60.7) 90(39.3) 32(2,50) 137(59.8) 92(40.2) 46(20.1) 183(79.9) 死亡组 31 19(61.3) 12(38.7) 61(50,72) 30(96.8) 1(3.2) 3(9.7) 28(90.3) 统计量值 χ2<0.01 Z=5.53 χ2=16.23 χ2=1.94 P值 0.950 <0.001 <0.001 0.164 注:TBSA为体表总面积 2.2 3种评分的一致性
在260例严重烧伤患者中,改良Baux评分与Ryan评分、改良Baux评分与比利时烧伤预后评分、Ryan评分与比利时烧伤预后评分结果均具有显著一致性(Kendall tau-b系数分别为0.75、0.71、0.86,P<0.001),见表2, 3, 4。
表2 260例严重烧伤患者改良Baux评分与Ryan评分结果的一致性情况(例)改良Baux 评分(分) 例数 Ryan评分 0分 1分 2分 3分 0~50 91 85 6 0 0 51~100 108 40 62 6 0 101~150 51 0 16 29 6 151~200 10 0 0 7 3 合计 260 125 84 32 9 表3 260例严重烧伤患者改良Baux评分与比利时烧伤预后评分结果的一致性情况(例)改良Baux 评分(分) 例数 比利时烧伤预后评分 0~2分 3~5分 6~8分 0~50 91 86 5 0 51~100 108 59 49 0 101~150 51 0 28 23 151~200 10 0 0 10 合计 260 145 75 33 表4 260例严重烧伤患者Ryan评分与比利时烧伤预后评分结果的一致性情况(例)Ryan评分(分) 例数 比利时烧伤预后评分 0~2分 3~5分 6~8分 0 125 124 1 0 1 84 21 63 0 2 32 0 18 24 3 9 0 0 9 合计 260 145 72 33 2.3 3种评分预测严重烧伤患者死亡风险的性能与相关参数比较
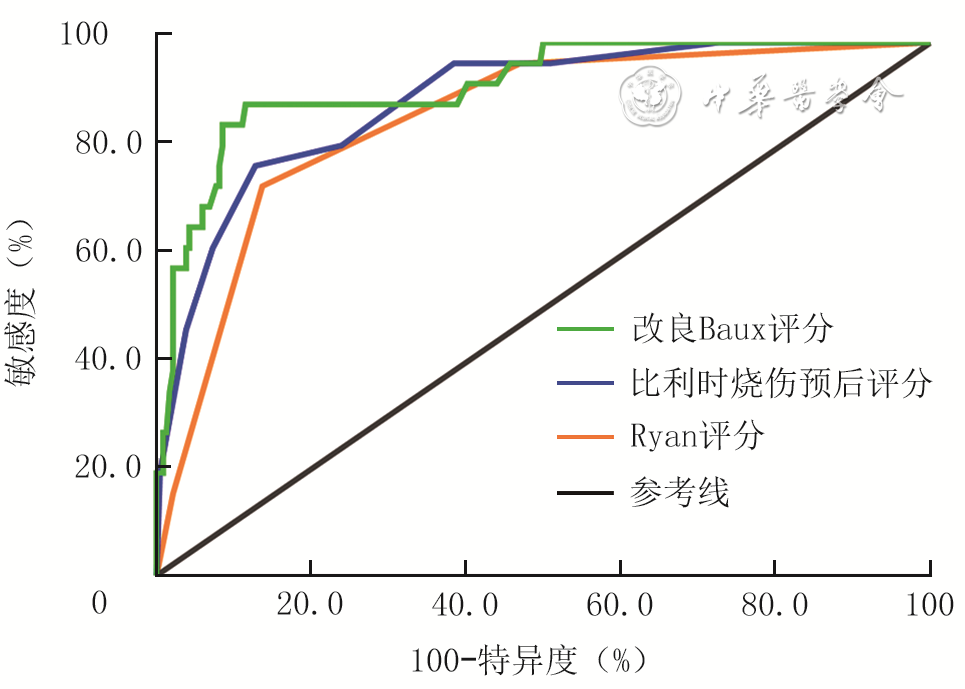
改良Baux评分、比利时烧伤预后评分、Ryan评分对260例严重烧伤患者死亡风险预测的ROC的AUC分别为0.92、0.89、0.85(95%置信区间分别为0.86~0.98、0.83~0.95、0.78~0.93,P<0.001),最佳阈值分别为106.5、4.5、1.5分,最佳阈值下的敏感度分别为88.5%、76.9%、73.1%,最佳阈值下的特异度分别为88.5%、87.2%、86.3%。见图1。
改良Baux评分与比利时烧伤预后评分的AUC质量相近(P>0.05),均明显优于Ryan评分(P<0.05),见表5。
表5 3种评分对260例严重烧伤患者死亡风险预测的受试者操作特征曲线下的曲线面积质量比较评分 曲线下面积差值 标准误 95%置信区间 z值 P值 改良Baux评分与比利时烧伤预后评分 0.03 0.02 -0.02~0.08 1.25 0.210 改良Baux评分与Ryan评分 0.07 0.03 0.01~0.12 2.35 0.019 比利时烧伤预后评分与Ryan评分 0.04 0.02 <0.01~0.07 2.11 0.035 3. 讨论
本研究描述了患者的人口统计学与疾病相关特征。与存活组相比,死亡组患者年龄更大,烧伤总面积更大,吸入性损伤发生率更高,改良Baux评分、比利时烧伤预后评分、Ryan评分的得分更高,这与以往研究的结果[17, 18]一致,证实了年龄、烧伤总面积、吸入性损伤这三大因素对严重烧伤患者预后的意义。前述3种评分越高的患者,其病死率越高,这说明评分越高的患者,伤情越严重,以往研究[8, 9]也证实了这一点。值得注意的是,本研究未观察到性别、烧伤部位和深度对病死率的影响;而Nygaard和Endorf[19]则认为相比于女性,男性在烧伤早期生存率更高。得出本研究结果的原因之一可能是本研究样本量偏小而出现的假阴性;原因之二,相对于烧伤总面积、年龄和吸入性损伤,性别和烧伤深度的差异对病死率的影响较小[20, 21, 22, 23]。此外,本研究结果显示死亡组患者合并基础疾病比例较高,该组患者可能因基础疾病加剧自身营养消耗,从而导致病情进一步恶化。因此,也应提高对存在基础疾病的严重烧伤患者的关注度。
本研究的优势之一在于对改良Baux评分、比利时烧伤预后评分、Ryan评分结果进行了一致性分析,类似研究报道少见。本研究结果表明,3种评分间有较强的一致性,说明基于南昌大学第一附属医院烧伤科的数据,3种国外预后评分工具间评分条目的一致性得到了验证。其中,比利时烧伤预后评分和Ryan评分之间的Kendall tau-b系数高达0.86,原因可能在于两者的评分方式较为相似,均对年龄、烧伤总面积、吸入性损伤进行分段式评分,不同于改良Baux评分的定量式评分。
本研究显示,改良Baux评分、比利时烧伤预后评分、Ryan评分都具有良好的严重烧伤患者死亡风险预测能力(AUC均>0.80),能对严重烧伤患者的死亡风险作出较为准确的判断。但是Ryan评分预测性能相对欠佳,可能是因为Ryan评分只把“年龄≥60岁、烧伤总面积≥40%TBSA、合并吸入性损伤”作为影响烧伤患者病死率的因子,当3种因子都存在时,每种因素只有1分,总分仅为3分,并且Ryan评分的最佳阀值为1.5分,对不同烧伤年龄、烧伤总面积患者的针对性不强。与本研究结果类似,Brusselaers等[13]分析认为Ryan评分预测性能相对欠佳的原因可能在于该评分对老年患者的过分关注,年龄≥60岁才被确定为风险因子。吸入性损伤主要与接触封闭区域的高温烟雾或爆炸有关,但目前对其诊断还存在争议,而吸入性损伤这一预测因子在Ryan评分中占比较另外2种预测工具高,所以Ryan评分误差也最大。故在使用Ryan评分之前,更加需要对吸入性损伤的诊断进行标准化[2]。与本研究结果相反,Tsurumi等[1]认为Ryan评分的预测准确性要好于改良Baux评分。本研究中合并吸入性损伤的患者仅占约30%,远低于其研究中55%的合并吸入性损伤比例,这可能是导致结果不同的主要原因。
本研究中比利时烧伤预后评分预测严重烧伤患者死亡的最佳阈值为4.5分,与印度尼西亚的一项研究结果[24]近似。值得注意的是,在理论上,新生儿及儿童因免疫不成熟,烧伤后的病死率应较成人高,但本研究结果却与上述理论假设相悖,本研究中存活组有25%的患者年龄≤2岁,这可能与新生儿及儿童的皮肤再生功能强有关。比利时烧伤预后评分开发团队的结果与本研究结果类似,其结果显示,即使研究对象中4岁以下的患儿占16%,但亚组分析时仅有1.8%的病死率[12],只有1名4岁以下的患儿死亡,他们认为危及生命的烧伤在儿童中极为罕见。此外,比利时烧伤预后评分纳入了3个风险因子,每个因子都被细分为不同的评分区间,但其评分区间定义过于随意(50~64、65~79岁),也较难识记,这也许是比利时烧伤预后评分尚未得到更广泛使用的原因所在[25]。
本研究显示,改良Baux评分预测严重烧伤患者死亡的ROC的AUC最大,说明其预测性能最佳,该结果与日本的一项多中心研究结果[26]一致。该评分的最佳阈值为106.5分,在此最佳阈值下,敏感度和特异度均高达88.5%,表明使用该评分确定高死亡风险患者的能力与排除高死亡风险患者的能力一致。但此最佳阈值略低于Christofides等[14]确定的112分,原因可能在于本研究纳入对象为严重烧伤患者,病情相对危重。相比于比利时烧伤预后评分和Ryan评分,改良Baux评分采用定量式评分,获得的最佳阀值更加精确。而且有研究者认为,改良Baux评分对年龄在20~80岁、烧伤总面积在30%~80%TBSA时表现出较好的预测性能[9,27]。本研究纳入的研究对象也多集中于上述年龄段内,故研究结果可靠。在临床实践中,改良Baux评分操作更为简单[28],临床护士或医师完全可以通过心算得出总分,非常适合在临床环境中使用。但为了精确预测患者死亡风险,未来可以采用列线图或转化成评分区间-死亡风险对应表,缩短评分时间,以便提供及时、有效的治疗方案以降低病死率。
综上所述,改良Baux评分、比利时烧伤预后评分、Ryan评分均能有效预测严重烧伤患者的预后,其中改良Baux评分预测性能更优。改良Baux评分简单、准确,对严重烧伤患者的风险管理具有较高的临床价值。利用该评分有助于明确严重烧伤患者的死亡风险,把握患者病情进展,并及时调整救护方案。然而,本研究为单中心小样本研究,可能存在选择偏倚,同时本研究不是前瞻性研究,无法控制许多混杂因素。为了验证本研究结论,今后还需开展前瞻性、大样本的多中心研究,以期探寻出更多影响严重烧伤患者预后的危险因素,并进一步验证改良Baux评分的预测效能。
谢志勤、王水连:论文撰写;郭光华、杨珍、易含笑:研究指导、经费支持、论文修改;唐鑫荣、刘德广、曾彦德:数据整理、统计分析所有作者均声明不存在利益冲突 -
参考文献
(28) [1] TsurumiA,QueYA,YanS,et al.Do standard burn mortality formulae work on a population of severely burned children and adults?[J].Burns,2015,41(5):935-945.DOI: 10.1016/j.burns.2015.03.017. [2] SheridanRL.Burn care: results of technical and organizational progress[J].JAMA,2003,290(6):719-722.DOI: 10.1001/jama.290.6.719. [3] 曾庆玲,王庆梅,陶利菊,等.特重度烧伤患者死亡风险列线图预测模型的建立及预测价值[J].中华烧伤杂志,2020,36(9):845-852.DOI: 10.3760/cma.j.cn501120-20190620-00280. [4] SaffleJR.Predicting outcomes of burns[J].N Engl J Med,1998,338(6):387-388.DOI: 10.1056/NEJM199802053380610. [5] LipHTC,IdrisMAM,ImranFH,et al.Predictors of mortality and validation of burn mortality prognostic scores in a Malaysian burns intensive care unit[J].BMC Emerg Med,2019,19(1):66.DOI: 10.1186/s12873-019-0284-8. [6] OslerT,GlanceLG,HosmerDW.Simplified estimates of the probability of death after burn injuries: extending and updating the baux score[J].J Trauma,2010,68(3):690-697.DOI: 10.1097/TA.0b013e3181c453b3. [7] RyanCM,SchoenfeldDA,ThorpeWP,et al.Objective estimates of the probability of death from burn injuries[J].N Engl J Med,1998,338(6):362-366.DOI: 10.1056/NEJM199802053380604. [8] SalehiSH, As'adiK, Abbaszadeh-KasbiA, et al. Comparison of six outcome prediction models in an adult burn population in a developing country[J]. Ann Burns Fire Disasters, 2017, 30(1): 13-17. [9] PrasadA,ThodeHCJr,SingerAJ.Predictive value of quick SOFA and revised Baux scores in burn patients[J].Burns,2020,46(2):347-351.DOI: 10.1016/j.burns.2019.03.006. [10] 樊钧豪,孙义方,伍国胜,等.基于改良全身炎症反应综合征评分建立的联合预测模型对大面积烧伤患者入院早期死亡风险的预测价值[J].中华烧伤杂志,2020,36(1):42-47.DOI: 10.3760/cma.j.issn.1009-2587.2020.01.008. [11] TsaiSY,LioCF,YaoWC,et al.Cost-drivers of medical expenses in burn care management[J].Burns,2020,46(4):817-824.DOI: 10.1016/j.burns.2020.01.004. [12] Belgian Outcome in Burn Injury Study Group.Development and validation of a model for prediction of mortality in patients with acute burn injury[J].Br J Surg,2009,96(1):111-117.DOI: 10.1002/bjs.6329. [13] BrusselaersN,AgbenorkuP,Hoyte-WilliamsPE.Assessment of mortality prediction models in a Ghanaian burn population[J].Burns,2013,39(5):997-1003.DOI: 10.1016/j.burns.2012.10.023. [14] ChristofidesC,MooreR,NelM.Baux score as a predictor of mortality at the CHBAH Adult Burns Unit[J].J Surg Res,2020,251:53-62.DOI: 10.1016/j.jss.2020.01.018. [15] 罗茉莉,郑建锋.实践教学中如何快速准确计算烧伤面积[J].当代护士(上旬刊),2019,26(4):158-159.DOI: 10.3969/j.issn.1006-6411.2019.04.078. [16] 李乐之,路潜.外科护理学[M].6版.北京:人民卫生出版社,2017. [17] LamNN,DucNM,HungNT.Influence of pre-existing medical condition and predicting value of modified Elixhauser comorbidity index on outcome of burn patients[J].Burns,2020,46(2):333-339.DOI: 10.1016/j.burns.2019.08.004. [18] XuY,JinX,ShaoX,et al.Valuable prognostic indicators for severe burn sepsis with inhalation lesion: age, platelet count, and procalcitonin[J/OL].Burns Trauma,2018,6:29[2020-11-13]. https://pubmed.ncbi.nlm.nih.gov/30397617/. DOI: 10.1186/s41038-018-0132-1. [19] NygaardRM,EndorfFW.Nonmedical factors influencing early deaths in burns: a study of the National Burn Repository[J].J Burn Care Res,2020,41(1):3-7.DOI: 10.1093/jbcr/irz139. [20] 朱丹,曹钰,何亚荣,等.4种评分对成人重度热力烧伤患者的死亡风险预测价值[J].西部医学,2015,27(12):1788-1791.DOI: 10.3969/j.issn.1672-3511.2015.12.008. [21] ChenCC,ChenLC,WenBS,et al.Objective estimates of the probability of death in acute burn injury: a proposed Taiwan burn score[J].J Trauma Acute Care Surg,2012,73(6):1583-1589.DOI: 10.1097/TA.0b013e318265ff5a. [22] RontoyanniVG, MalagarisI, HerndonDN, et al. Skeletal muscle mitochondrial function is determined by burn severity, sex, and sepsis, and is associated with glucose metabolism and functional capacity in burned children[J]. Shock,2018,50(2):141-148. DOI: 10.1097/SHK.0000000000001074. [23] JeschkeMG, PintoR, CostfordSR, et al. Threshold age and burn size associated with poor outcomes in the elderly after burn injury[J]. Burns,2016,42(2):276-281. DOI: 10.1016/j.burns.2015.12.008. [24] FitriA, SaputraD, PutraAE. Perbandingan R-Baux score dengan BOBI score sebagai prediktor mortalitas pasien luka bakar di RSUP Dr. M. Djamil Padang[J]. Majalah Kedokteran Bandung, 2018,50(2):79-85. DOI: 10.15395/mkb.v50n2.1326. [25] WilliamsDJ,WalkerJD.A nomogram for calculation of the Revised Baux Score[J].Burns,2015,41(1):85-90.DOI: 10.1016/j.burns.2014.05.001. [26] YoshimuraY,SaitohD,YamadaK,et al.Comparison of prognostic models for burn patients: a retrospective nationwide registry study[J].Burns,2020,46(8):1746-1755.DOI: 10.1016/j.burns.2020.10.008. [27] SaadatGH,ToorR,MazharF,et al.Severe burn injury: body mass index and the Baux score[J].Burns,2021,47(1):72-77.DOI: 10.1016/j.burns.2020.10.017. [28] HalgasB,BayC,FosterK.A comparison of injury scoring systems in predicting burn mortality[J].Ann Burns Fire Disasters,2018,31(2):89-93. -
表1 2组严重烧伤患者一般资料比较
组别 例数 性别[例(%)] 年龄[岁,M(Q1,Q3)] 烧伤原因[例(%)] 烧伤部位[例(%)] 男 女 火焰 其他 1处 ≥2处 存活组 229 139(60.7) 90(39.3) 32(2,50) 137(59.8) 92(40.2) 46(20.1) 183(79.9) 死亡组 31 19(61.3) 12(38.7) 61(50,72) 30(96.8) 1(3.2) 3(9.7) 28(90.3) 统计量值 χ2<0.01 Z=5.53 χ2=16.23 χ2=1.94 P值 0.950 <0.001 <0.001 0.164 注:TBSA为体表总面积  下载: 导出CSV
下载: 导出CSV
表2 260例严重烧伤患者改良Baux评分与Ryan评分结果的一致性情况(例)
改良Baux 评分(分) 例数 Ryan评分 0分 1分 2分 3分 0~50 91 85 6 0 0 51~100 108 40 62 6 0 101~150 51 0 16 29 6 151~200 10 0 0 7 3 合计 260 125 84 32 9
下载: 导出CSV
表3 260例严重烧伤患者改良Baux评分与比利时烧伤预后评分结果的一致性情况(例)
改良Baux 评分(分) 例数 比利时烧伤预后评分 0~2分 3~5分 6~8分 0~50 91 86 5 0 51~100 108 59 49 0 101~150 51 0 28 23 151~200 10 0 0 10 合计 260 145 75 33
下载: 导出CSV
表4 260例严重烧伤患者Ryan评分与比利时烧伤预后评分结果的一致性情况(例)
Ryan评分(分) 例数 比利时烧伤预后评分 0~2分 3~5分 6~8分 0 125 124 1 0 1 84 21 63 0 2 32 0 18 24 3 9 0 0 9 合计 260 145 72 33
下载: 导出CSV
表5 3种评分对260例严重烧伤患者死亡风险预测的受试者操作特征曲线下的曲线面积质量比较
评分 曲线下面积差值 标准误 95%置信区间 z值 P值 改良Baux评分与比利时烧伤预后评分 0.03 0.02 -0.02~0.08 1.25 0.210 改良Baux评分与Ryan评分 0.07 0.03 0.01~0.12 2.35 0.019 比利时烧伤预后评分与Ryan评分 0.04 0.02 <0.01~0.07 2.11 0.035
下载: 导出CSV
-

 下载:
下载:

计量
- 文章访问数: 363
- HTML全文浏览量: 75
- PDF下载量: 47
- 被引次数: 0
