



Clinical effects of partially de-epithelized local flaps in repairing tubercular chest wall defects
-
摘要:
目的 探讨部分去表皮局部皮瓣修复结核性胸壁缺损创面的临床效果。 方法 采用回顾性观察性研究方法。2010年4月——2021年2月解放军总医院第八医学中心烧伤整形科收治12例符合入选标准的患者,其中男9例、女3例,年龄(42±18)岁。清创后结核性胸壁缺损范围为4 cm×3 cm×2 cm~16 cm×8 cm×5 cm,均采用部分去表皮局部皮瓣修复,皮瓣宽度等于缺损区的宽度,皮瓣长度较缺损区长度增加2 cm。其中1例患者局部皮瓣切取面积过大导致供区不能直接缝合,采用自体背部游离中厚皮片移植术修复;其余患者局部皮瓣切取面积均较小,供瓣区直接拉拢缝合。观察并记录手术时长、术中出血情况、术后引流管引流量和留置时长;术后2周皮瓣的存活情况、质地和颜色,受区有无皮下积液和皮肤破溃以及供区愈合情况,包括有无切口裂开、局部感染、血肿发生。术后1个月做胸部X线、CT或核磁共振成像,检查患者胸壁缺损创面及伴发的结核病部位有无新发的局部积液和骨质破坏。随访6个月以上,记录患者胸壁缺损创面的手术切口有无瘢痕增生、红肿、窦道等。 结果 患者手术时长为(104±18)min,术中出血量为(119±53)mL,引流管累计引流量为(134±49)mL,引流管留置时长为(5.3±1.7)d。术后2周,患者移植的局部皮瓣全部存活,皮瓣质地和颜色与周围正常皮肤接近,其中1例患者胸壁缺损区切口有渗液,部分切口裂开,行Ⅱ期手术后创面愈合良好;其余患者胸壁缺损区创面均无切口感染、皮下积液或切口裂开等情况。患者供区切口均愈合,无切口裂开和局部感染以及血肿发生。术后1个月,患者胸部影像学检查未观察到术区存在新的骨质破坏。随访6~96个月,1例患者术后12个月在胸壁缺损创面的手术部位切口出现肿胀、破溃及窦道,行Ⅱ期手术后创面愈合良好;其余患者胸壁缺损创面的手术切口愈合良好,无瘢痕、红肿、窦道等。 结论 胸壁结核导致的胸壁缺损创面采用部分去表皮局部皮瓣修复,具有供区损伤小、皮瓣设计灵活、术后创面愈合良好的优点。 Abstract:Objective To explore the clinical effects of partially de-epithelized local flaps in repairing tubercular chest wall defects. Methods A retrospective observational study was conducted. From April 2010 to February 2021, twelve patients who met the inclusion criteria were admitted to the Department of Burns and Plastic Surgery of the Eighth Medical Center of PLA General Hospital, including 9 males and 3 females with age of (42±18) years. The sizes of tubercular chest wall defects of patients were ranged from 4 cm×3 cm×2 cm to 16 cm×8 cm×5 cm, which were all repaired with partial de-epithelized local flaps. The widths of flaps were equal to the widths of the defects, and the lengths of flaps were 2 cm longer than those of the defects. In one patient, the local flap was too large to close the donor site directly by suturing, so an autologous back free medium thickness skin graft was used for repair. In other patients, the collection areas of local flaps were small, and the donor areas of flaps were directly closed. The duration of operation, intraoperative bleeding, and postoperative drainage volume and indwelling time of drainage tube were observed and recorded. In two weeks after operation, the survival, color, and texture of flaps, the presence of subcutaneous hydrops and skin ulcer, and donor site healing including wound disruption, local infection, hematoma were observed. Chest X-ray, CT scan, or nuclear magnetic resonance imaging was performed in one month after operation to check whether new local hydrops and bone destruction occurred in the chest wall defects and the concomitant tuberculose focus of patients. All patients were followed up for more than 6 months to record whether the surgical incisions of the chest wall defects of the patients were complicated by hypertrophic scar, redness, swelling, and sinus. Results In surgery, the patient had (104±18) min of operation duration, (119±53) mL of intraoperative bleeding, (134±49) mL of cumulative drainage of drainage tube, and (5.3±1.7) days of drainage tube indwelling time. In two weeks after operation, all the grafted local flaps survived, and the color and texture of flaps were similar to the surrounding normal skin. One patient had fluid leakage from the incision of chest wall defect area with the incision partially dehisced, which healed well after a phase Ⅱ operation; no wound infection, subcutaneous hydrops, or wound rupture occurred in other patients. The incisions of donor sites in all the patients healed well and no wound disruption, local infection, or hematoma occurred. One month after operation, no new bone destruction was observed in the operative region by chest imaging examination. Patients were followed up for 6 to 96 months, with one patient having wound swelling, ulceration, and sinus in the operative area of the chest wall defect in 12 months after surgery, which healed after phase Ⅱ operation; the incisions of chest wall defect wounds in other patients healed well and had no scar, redness and swelling, or sinus. Conclusions Partially de-epithelized local flap could be used in repairing tubercular chest wall defect wounds, with the advantages of flexible flap design, minimal donor site injury, and good postoperative wound healing. -
Key words:
- Wound healing /
- Tuberculosis /
- Thoracic wall /
- Skin /
- Local flap /
- De-epithelization
-
参考文献
(29) [1] KangW, YuJ, DuJ, et al. The epidemiology of extrapulmonary tuberculosis in China: a large-scale multi-center observational study[J]. PLoS One, 2020,15(8):e0237753. DOI: 10.1371/journal.pone.0237753. [2] PangY, AnJ, ShuW, et al. Epidemiology of extrapulmonary tuberculosis among inpatients, China, 2008-2017[J]. Emerg Infect Dis, 2019,25(3):457-464. DOI: 10.3201/eid2503.180572. [3] NatarajanA, BeenaPM, DevnikarAV, et al. A systemic review on tuberculosis[J]. Indian J Tuberc, 2020,67(3):295-311. DOI: 10.1016/j.ijtb.2020.02.005. [4] LiuY, ZhangXX, YuJJ, et al. Tuberculosis relapse is more common than reinfection in Beijing, China[J]. Infect Dis (Lond), 2020,52(12):858-865. DOI: 10.1080/23744235.2020.1794027. [5] GlaziouP, FloydK, RaviglioneMC. Global epidemiology of tuberculosis[J]. Semin Respir Crit Care Med, 2018,39(3):271-285. DOI: 10.1055/s-0038-1651492. [6] MajeedFA, AliA, ZafarU, et al. Outcome analysis of primary chest wall tuberculosis: a series of 32 cases[J]. J Ayub Med Coll Abbottabad, 2021,33(3):357-362. [7] NaranjeP, BhallaAS, SherwaniP. Chest tuberculosis in children[J]. Indian J Pediatr, 2019,86(5):448-458. DOI: 10.1007/s12098-018-02847-7. [8] HossainM, AzzadAK, IslamS, et al. Multiple chest wall tuberculous abscesses[J]. J Pak Med Assoc, 2010,60(7):589-591. [9] KabilanK, GulatiM, BandayIA, et al. Myriad faces of active tuberculosis: intrapulmonary bronchial artery pseudoaneurysm[J]. Vasc Endovascular Surg, 2021:15385744211051812. DOI: 10.1177/15385744211051812. [10] Moyano-BuenoD, BlancoJF, López-BernusA, et al. Cold abscess of the chest wall: a diagnostic challenge[J]. Int J Infect Dis, 2019,85:108-110. DOI: 10.1016/j.ijid.2019.05.031. [11] IgaN, FuchimotoY, KoyanagiT, et al. A rare case of chest wall tuberculosis: tuberculous scapulothoracic bursitis[J]. Respir Med Case Rep, 2021,34:101537. DOI: 10.1016/j.rmcr.2021.101537. [12] DidaceMM, IdaLL, IrèneO, et al. Management of tuberculous cutaneous fistula[J]. Case Rep Surg, 2020,2020:7840963. DOI: 10.1155/2020/7840963. [13] KunciwSE, de la CruzEC. Incidental finding of tuberculosis during evaluation for delayed wound healing[J]. Mil Med, 2021,186(3/4):e457-e460. DOI: 10.1093/milmed/usaa366. [14] KabiriEH, AlassaneEA, KamdemMK, et al. Tuberculous cold abscess of the chest wall: a clinical and surgical experience. Report of 16 cases(case series)[J]. Ann Med Surg (Lond),2020,51:54-58. DOI: 10.1016/j.amsu.2020.02.001. [15] HusseinM, AbdelhadiA, ElarabiA, et al. Extrapulmonary Tuberculosis masquerading as chest wall malignancy: just never ceases to surprise![J]. IDCases, 2021,24:e01114. DOI: 10.1016/j.idcr.2021.e01114. [16] 贾赤宇.结核性创面贾赤宇2017观点[M].北京:科学技术文献出版社,2017:12-15. [17] MalathiL, DasS, NairJ, et al. Chest wall reconstruction: success of a team approach-a 12-year experience from a tertiary care institution[J]. Indian J Thorac Cardiovasc Surg, 2020,36(1):44-51. DOI: 10.1007/s12055-019-00841-y. [18] ShamjiFM. Sepsis in the postpneumonectomy space: pathogenesis, recognition, and management[J]. Thorac Surg Clin, 2021,31(4):407-416. DOI: 10.1016/j.thorsurg.2021.08.001. [19] KimWJ, KimWS, KimHK, et al. Reconstruction of small chest wall defects caused by tubercular abscesses using two different flaps[J]. Ann Thorac Surg, 2018,106(5):e249-e251. DOI: 10.1016/j.athoracsur.2018.04.019. [20] ChoKD, ChoDG, JoMS, et al. Current surgical therapy for patients with tuberculous abscess of the chest wall[J]. Ann Thorac Surg, 2006,81(4):1220-1226. DOI: 10.1016/j.athoracsur.2005.10.044. [21] 李鹏程, 郑梦利, 邱亚斌, 等. 皮瓣联合真皮瓣填充修复胸壁结核性溃疡创面八例[J].中华烧伤杂志,2012,28(1):55-56. DOI: 10.3760/cma.j.issn.1009-2587.2012.01.014. [22] SotgiuG, CentisR, MiglioriGB. Post-tuberculosis sequelae and their socioeconomic consequences: worth investigating[J]. Lancet Glob Health, 2021,9(12):e1628-e1629. DOI: 10.1016/S2214-109X(21)00454-X. [23] AllwoodBW, van der ZalmMM, AmaralA, et al. Post-tuberculosis lung health: perspectives from the First International Symposium[J]. Int J Tuberc Lung Dis, 2020,24(8):820-828. DOI: 10.5588/ijtld.20.0067. [24] BehrMA, KaufmannE, DuffinJ, et al. Latent tuberculosis: two centuries of confusion[J]. Am J Respir Crit Care Med, 2021,204(2):142-148. DOI: 10.1164/rccm.202011-4239PP. [25] BarryCE, Mayer-BarberKD. Signature required: the transcriptional response to tuberculosis[J].J Exp Med, 2021,218(12):e20211665.DOI: 10.1084/jem.20211665. [26] SakurabaM, SagaraY, KomatsuH. Surgical treatment of tuberculous abscess in the chest wall[J]. Ann Thorac Surg, 2005,79(3):964-967. DOI: 10.1016/j.athoracsur.2004.09.004. [27] 江红,臧国庆.肺外结核[J].中华全科医学,2012, 10(1):103-104. [28] RayS, TalukdarA, KunduS, et al. Diagnosis and management of miliary tuberculosis: current state and future perspectives[J]. Ther Clin Risk Manag, 2013,9:9-26. DOI: 10.2147/TCRM.S29179. [29] GroverSB, JainM, DumeerS, et al. Chest wall tuberculosis--a clinical and imaging experience[J]. Indian J Radiol Imaging, 2011,21(1):28-33. DOI: 10.4103/0971-3026.76051. -

1 部分去表皮局部皮瓣修复结核性胸壁缺损的设计示意图。1A.ABCD围成区域为创面区,AEF围成区域为设计的局部皮瓣,BD=DF,AE稍长于AC;1B.皮瓣局部去表皮范围为AGE,GE的长度=创面的深度;1C.局部皮瓣AEF掀起后向上旋转修复创面,去表皮后的真皮脂肪筋膜组织AGE翻转填充到创面ABCD的深部,AG的皮肤边缘与ABC的皮肤相对缝合,G点与C点缝合,D点与F点缝合

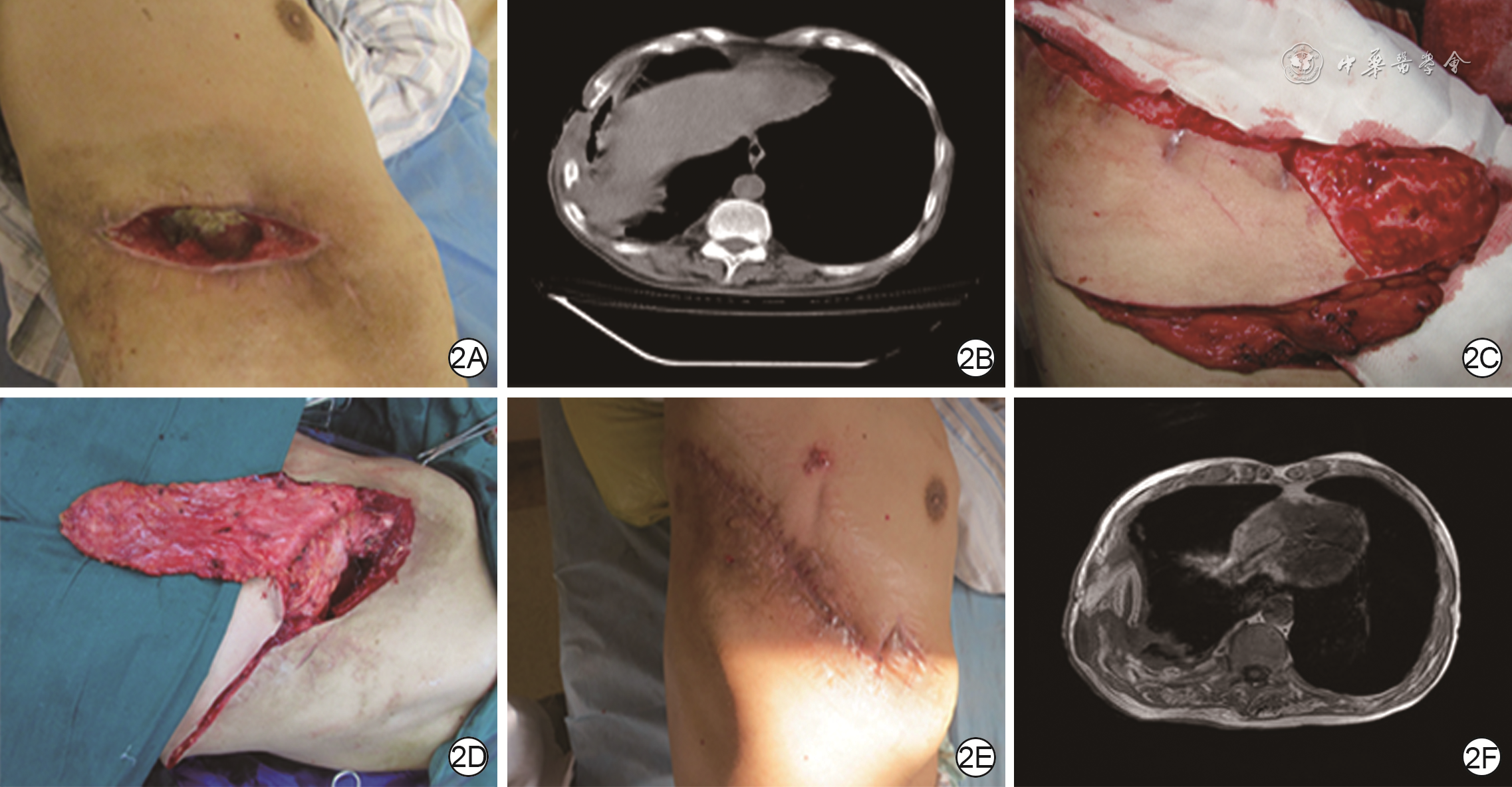
2 采用部分去表皮局部皮瓣修复例1患者结核性胸壁缺损创面。2A.结核性脓胸清创后可见胸壁形成口小底大的胸壁缺损;2B.CT显示肋骨部分缺失(既往手术切除),并有包裹性积液和肋骨的感染破坏;2C.局部皮瓣切取并去除部分表皮;2D.供瓣区直接缝合,部分去表皮局部皮瓣填充清创后的胸壁缺损;2E.第2次手术后3周,切口愈合良好;2F.第2次手术后3周,胸部CT显示胸壁缺损已经被软组织填充修复

3 采用部分去表皮局部皮瓣修复例2患者结核性胸壁缺损创面。3A.术前胸壁切口下可见有大量坏死组织;3B.设计的2个局部皮瓣部分去表皮后放置到胸壁缺损区待固定;3C.术后1年随访,可见创面愈合良好,无瘢痕增生、红肿、积液
表1 12例结核性胸壁缺损患者行部分去表皮局部皮瓣修复术的相关情况
患者编号 出血量(mL) 手术时间(min) 累计引流量(mL) 引流管留置时长(d) 随访时间(个月) 不良事件 病例1 80 100 95 4 54 无 病例2 105 80 155 6 31 无 病例3 95 110 187 7 35 远期窦道 病例4 112 120 166 8 22 无 病例5 90 75 120 5 30 无 病例6 89 120 150 7 18 无 病例7 155 90 246 6 20 切口裂开 病例8 125 100 90 4 30 无 病例9 50 120 113 5 92 无 病例10 85 80 72 3 12 无 病例11 205 130 115 5 96 无 病例12 240 120 95 4 6 无  下载: 导出CSV
下载: 导出CSV
-

 下载:
下载:



图(3) / 表(1)
计量
- 文章访问数: 471
- HTML全文浏览量: 164
- PDF下载量: 50
- 被引次数: 0
