



A prospective study on the development and application verification of the quantitative evaluation software for three-dimensional morphology of pathological scars based on photo modeling technology
-
摘要:
目的 开发一款基于照片建模技术的病理性瘢痕三维形态量化评估软件,并验证其在临床应用中的准确性和可行性。 方法 采用前瞻性观察性研究方法。解放军总医院第一医学中心2019年4月—2022年1月收治59例符合入选标准的病理性瘢痕患者(共107处瘢痕),其中男27例、女32例,年龄33(26,44)岁。以照片建模技术为基础,自主研发具有患者基本信息采集及瘢痕拍照、三维重建、模型浏览、报告生成等功能的病理性瘢痕三维形态测量软件。采用软件和临床常规方法(游标卡尺、彩色多普勒超声诊断仪及弹性体印模注水法测量)分别测量瘢痕的最长径、最大厚度及体积。统计建模成功瘢痕的数量、分布、患者数及使用软件和临床常规方法测量的瘢痕最长径、最大厚度、体积,统计建模失败瘢痕的数量、分布、类型及患者数。采用一元线性回归分析及Bland-Altman法分别分析软件和临床常规方法测量瘢痕最长径、最大厚度、体积的相关性和一致性,分别计算组内相关系数(ICC)、平均绝对误差、平均绝对百分误差。 结果 对54例患者的102处瘢痕成功建模,瘢痕位于胸部43处、肩背部27处、四肢12处、面颈部9处、耳廓6处、腹部5处。使用软件和临床常规方法测量的瘢痕最长径、最大厚度、体积分别为3.61(2.13,5.19)、3.53(2.02,5.11)cm,0.45(0.28,0.70)、0.43(0.24,0.72)cm,1.17(0.43,3.57)、0.96(0.36,3.26)mL。5例患者5处增生性瘢痕或耳廓瘢痕疙瘩建模失败。使用软件和临床常规方法测量的瘢痕最长径、最大厚度、体积均呈显著线性相关(r值分别为0.985、0.917、0.998,P<0.05)。使用软件和临床常规方法测量的瘢痕最长径、最大厚度、体积ICC分别为0.993、0.958、0.999(95%置信区间分别为0.989~0.995、0.938~0.971、0.998~0.999)。软件和临床常规方法测量的瘢痕最长径、最大厚度、体积一致性较好。Bland-Altman法分析显示,分别有3.92%(4/102)、7.84%(8/102)、8.82%(9/102)的瘢痕最长径、最大厚度、体积在95%一致性界限以外;在95%一致性界限以内,2.04%(2/98)的瘢痕最长径误差在0.5 cm以上,1.06%(1/94)的瘢痕最大厚度误差在0.2 cm以上,2.15%(2/93)的瘢痕体积误差在0.5 mL以上。软件与临床常规方法测量的瘢痕最长径、最大厚度、体积的平均绝对误差分别为0.21 cm、0.10 cm、0.24 mL,平均绝对百分误差分别为5.75%、21.21%、24.80%。 结论 基于照片建模技术的病理性瘢痕三维形态量化评估软件可以实现对大部分瘢痕的三维建模和形态参数测量。该软件测量结果与临床常规方法测量结果具有较好的一致性,误差在临床可接受范围内,能够作为病理性瘢痕临床诊断与治疗的辅助方法。 Abstract:Objective To develop a quantitative evaluation software for three-dimensional morphology of pathological scars based on photo modeling technology, and to verify its accuracy and feasibility in clinical application. Methods The method of prospective observational study was adopted. From April 2019 to January 2022, 59 patients with pathological scars (totally 107 scars) who met the inclusion criteria were admitted to the First Medical Center of Chinese PLA General Hospital, including 27 males and 32 females, aged 33 (26, 44) years. Based on photo modeling technology, a software for measuring three-dimensional morphological parameters of pathological scars was developed with functions of collecting patients' basic information, and scar photography, three-dimensional reconstruction, browsing the models, and generating reports. This software and the clinical routine methods (vernier calipers, color Doppler ultrasonic diagnostic equipment, and elastomeric impression water injection method measurement) were used to measure the longest length, maximum thickness, and volume of scars, respectively. For scars with successful modelling, the number, distribution of scars, number of patients, and the longest length, maximum thickness, and volume of scars measured by both the software and clinical routine methods were collected. For scars with failed modelling, the number, distribution, type of scars, and the number of patients were collected. The correlation and consistency of the software and clinical routine methods in measuring the longest length, maximum thickness, and volume of scars were analyzed by unital linear regression analysis and the Bland-Altman method, respectively, and the intraclass correlation coefficients (ICCs), mean absolute error (MAE), and mean absolute percentage error (MAPE) were calculated. Results A total of 102 scars from 54 patients were successfully modeled, which located in the chest (43 scars), in the shoulder and back (27 scars), in the limb (12 scars), in the face and neck (9 scars), in the auricle (6 scars), and in the abdomen (5 scars). The longest length, maximum thickness, and volume measured by the software and clinical routine methods were 3.61 (2.13, 5.19) and 3.53 (2.02, 5.11) cm, 0.45 (0.28, 0.70) and 0.43 (0.24, 0.72) cm, 1.17 (0.43, 3.57) and 0.96 (0.36, 3.26) mL. The 5 hypertrophic scars and auricular keloids from 5 patients were unsuccessfully modeled. The longest length, maximum thickness, and volume measured by the software and clinical routine methods showed obvious linear correlation (with r values of 0.985, 0.917, and 0.998, P<0.05). The ICCs of the longest length, maximum thickness, and volume of scars measured by the software and clinical routine methods were 0.993, 0.958, and 0.999 (with 95% confidence intervals of 0.989-0.995, 0.938-0.971, and 0.998-0.999, respectively). The longest length, maximum thickness, and volume of scars measured by the software and clinical routine methods had good consistency. The Bland-Altman method showed that 3.92% (4/102), 7.84% (8/102), and 8.82% (9/102) of the scars with the longest length, maximum thickness, and volume respectively were outside the 95% consistency limit. Within the 95% consistency limit, 2.04% (2/98) scars had the longest length error of more than 0.5 cm, 1.06% (1/94) scars had the maximum thickness error of more than 0.2 cm, and 2.15% (2/93) scars had the volume error of more than 0.5 mL. The MAE and MAPE of the longest length, maximum thickness, and volume of scars measured by the software and clinical routine methods were 0.21 cm, 0.10 cm, 0.24 mL, and 5.75%, 21.21%, 24.80%, respectively. Conclusions The quantitative evaluation software for three-dimensional morphology of pathological scars based on photo modeling technology can realize the three-dimensional modeling and measurement of morphological parameters of most pathological scars. Its measurement results were in good consistency with those of clinical routine methods, and the errors were acceptable in clinic. This software can be used as an auxiliary method for clinical diagnosis and treatment of pathological scars. -
Key words:
- Cicatrix /
- Software /
- Three-dimensional morphology /
- Quantitative assessment /
- Photo-based modeling
-
姜伟乾:研究操作、数据采集、论文撰写;潘锋:研究操作、数据采集;柴密、乌兰哈斯:研究病例招募、数据整理;于雪冬:软件研发;郭伶俐:研究指导、论文修改所有作者均声明不存在利益冲突
-
参考文献
(30) [1] WangPH,HuangBS,HorngHC,et al.Wound healing[J].J Chin Med Assoc,2018,81(2):94-101.DOI: 10.1016/j.jcma.2017.11.002. [2] GoldMH,NestorMS,BermanB,et al.Assessing keloid recurrence following surgical excision and radiation[J/OL].Burns Trauma,2020,8:tkaa031[2022-05-13].https://pubmed.ncbi.nlm.nih.gov/33225004/.DOI: 10.1093/burnst/tkaa031. [3] OgawaR,AkitaS,AkaishiS,et al.Diagnosis and treatment of keloids and hypertrophic scars-japan scar workshop consensus document 2018[J/OL].Burns Trauma,2019,7:39[2022-05-13].https://pubmed.ncbi.nlm.nih.gov/31890718/.DOI: 10.1186/s41038-019-0175-y. [4] LvK,XiaZ,Chinese consensus panel on the prevention and treatment of scars.Chinese expert consensus on clinical prevention and treatment of scar[J/OL].Burns Trauma,2018,6:27[2022-05-13].https://pubmed.ncbi.nlm.nih.gov/30263894/.DOI: 10.1186/s41038-018-0129-9. [5] MokosZB, JovićA, GrgurevićL, et al. Current therapeutic approach to hypertrophic scars [J]. Front Med (Lausanne), 2017, 4: 83.DOI: 10.3389/fmed.2017.00083. [6] 中国整形美容协会瘢痕医学分会常务委员会专家组.中国瘢痕疙瘩临床治疗推荐指南[J].中国美容整形外科杂志,2018,29(5):前插3-前插14.DOI: 10.3969/j.issn.1673-7040.2018.05.001. [7] FinlayV,BurrowsS,KendellR,et al.Modified Vancouver Scar Scale score is linked with quality of life after burn[J].Burns,2017,43(4):741-746.DOI: 10.1016/j.burns.2016.11.007. [8] ElrefaieAM,SalemRM,FaheemMH.High-resolution ultrasound for keloids and hypertrophic scar assessment[J].Lasers Med Sci,2020,35(2):379-385.DOI: 10.1007/s10103-019-02830-4. [9] DengH,Li-TsangCWP,LiJ.Measuring vascularity of hypertrophic scars by dermoscopy: construct validity and predictive ability of scar thickness change[J].Skin Res Technol,2020,26(3):369-375.DOI: 10.1111/srt.12812. [10] LobosN,WortsmanX,ValenzuelaF,et al.Color Doppler ultrasound assessment of activity in keloids[J].Dermatol Surg,2017,43(6):817-825.DOI: 10.1097/DSS.0000000000001052. [11] TaylorB,McGroutherDA,BayatA.Use of a non-contact 3D digitiser to measure the volume of keloid scars: a useful tool for scar assessment[J].J Plast Reconstr Aesthet Surg,2007,60(1):87-94.DOI: 10.1016/j.bjps.2005.12.051. [12] 沈丹枫,施远,夏玲玲,等.便携式高精度三维扫描仪在瘢痕量化评估中的应用——附10例瘢痕疙瘩临床报告[J].组织工程与重建外科杂志,2016,12(1):37-40.DOI: 10.3969/j.issn.1673-0364.2016.01.010. [13] 刘春军 三维扫描技术在乳房测量评估中的应用 北京 北京协和医学院 2014 刘春军. 三维扫描技术在乳房测量评估中的应用[D]. 北京:北京协和医学院, 2014.
[14] van der AaT, VerhielSH, ErendsM, et al. A simplified three-dimensional volume measurement technique in keloid scars: validity and reliability[J]. J Plast Reconstr Aesthet Surg, 2015,68(11):1574-1580. DOI: 10.1016/j.bjps.2015.07.001. [15] StekelenburgCM, JaspersME, NiessenFB, et al. In a clinimetric analysis, 3D stereophotogrammetry was found to be reliable and valid for measuring scar volume in clinical research[J]. J Clin Epidemiol, 2015,68(7):782-787. DOI: 10.1016/j.jclinepi.2015.02.014. [16] 吕开阳,肖仕初,夏照帆.“中国临床瘢痕防治专家共识”解读[J].中华整形外科杂志,2018,34(12):985-990.DOI: 10.3760/cma.j.issn.1009-4598.2018.12.001. [17] 中国临床瘢痕防治专家共识制定小组.中国临床瘢痕防治专家共识[J/CD].中华损伤与修复杂志:电子版,2017,12(6):401-406.DOI: 10.3877/cma.j.issn.1673-9450.2017.06.001. [18] BrownM, LoweDG. Unsupervised 3D object recognition and reconstruction in unordered datasets [G/OL]. International Conference on 3-D Digital Imaging & Modeling, 2005: 56-63[2022-05-13].https://xueshu.baidu.com/usercenter/paper/show?paperid=ebf9f00a096152a73c32ba12dd17f32c&site=xueshu_se. https://xueshu.baidu.com/usercenter/paper/show?paperid=ebf9f00a096152a73c32ba12dd17f32c&site=xueshu_se [19] 杨罗坤 基于多幅照片的三维人脸重建算法研究和实现 南京 南京邮电大学 2018 杨罗坤. 基于多幅照片的三维人脸重建算法研究和实现 [D].南京:南京邮电大学, 2018.
[20] 张婧秋,杨淑霞,涂平,等.74例瘢痕疙瘩疗效分析及超声在瘢痕疙瘩治疗中的监测作用[J].实用皮肤病学杂志,2017,10(3):136-141.DOI: 10.11786/sypfbxzz.1674-1293.20170303. [21] 唐家训.介绍一种小面积增生性瘢痕体积测量方法[J].中华整形外科杂志,2004,20(2):152.DOI: 10.3760/j.issn:1009-4598.2004.02.026. [22] 陈卉.Bland-Altman分析在临床测量方法一致性评价中的应用[J].中国卫生统计,2007,24(3):308-309,315.DOI: 10.3969/j.issn.1002-3674.2007.03.029. [23] VerhaegenPDHM, van der WalMBA, MiddelkoopE, et al. Objective scar assessment tools: a clinimetric appraisal [J]. Plast Reconstr Surg, 2011, 127(4): 1561-1570.DOI: 10.1097/PRS.0b013e31820a641a. [24] LeeKC,DretzkeJ,GroverL,et al.A systematic review of objective burn scar measurements[J/OL].Burns Trauma,2016,4:14[2022-05-13].https://pubmed.ncbi.nlm.nih.gov/27574684/.DOI: 10.1186/s41038-016-0036-x. [25] 谢春晖,高欣欣,贾冀斌,等.Antera 3D®相机在瘢痕疙瘩治疗效果评估中的临床应用[J].中华烧伤杂志,2018,34(2):117-119.DOI: 10.3760/cma.j.issn.1009-2587.2018.02.012. [26] 马欢欢, 赵清坡. Agisoft Photoscan照片建模技术在考古中的应用 [J]. 文物保护与考古科学, 2016, 28(4): 144-149.DOI: 10.16334/j.cnki.cn31-1652/k.2016.04.019. [27] 李波. Agisoft Photoscan多视点3D建模技术在校园虚拟漫游中的应用 [J]. 信息与电脑(理论版), 2019(6): 115-116. [28] MorganB,FordALJ,SmithMJ.Standard methods for creating digital skeletal models using structure-from-motion photogrammetry[J].Am J Phys Anthropol,2019,169(1):152-160.DOI: 10.1002/ajpa.23803. [29] 郭丽芳 白癜风诊断和病情评价人工智能模型的建立及临床应用 北京 中国医学科学院 2020 郭丽芳. 白癜风诊断和病情评价人工智能模型的建立及临床应用[D]. 北京:中国医学科学院, 2020.
[30] 侯奕辰,彭辉,谢俊章,等.改进Unet++在脑肿瘤图像分割的研究[J].计算机工程与设计,2022,43(6):1725-1731.DOI: 10.16208/j.issn1000-7024.2022.06.029. -

1 自主研发的病理性瘢痕三维形态量化评估软件与临床常规方法测量的54例患者102处病理性瘢痕三维形态参数Bland-Altman图。1A.最长径;1B.最大厚度;1C.体积
注:差值、平均值分别为软件测量与临床常规方法测量结果的差值和平均值,图中2条红色虚线代表差值的95%一致性界限的上下限,2条蓝色虚线代表临床可接受的误差上下限,黑色实线代表差值为0的线,黑色虚线代表差值的平均值(图1A中黑色虚线与黑色实线重合)
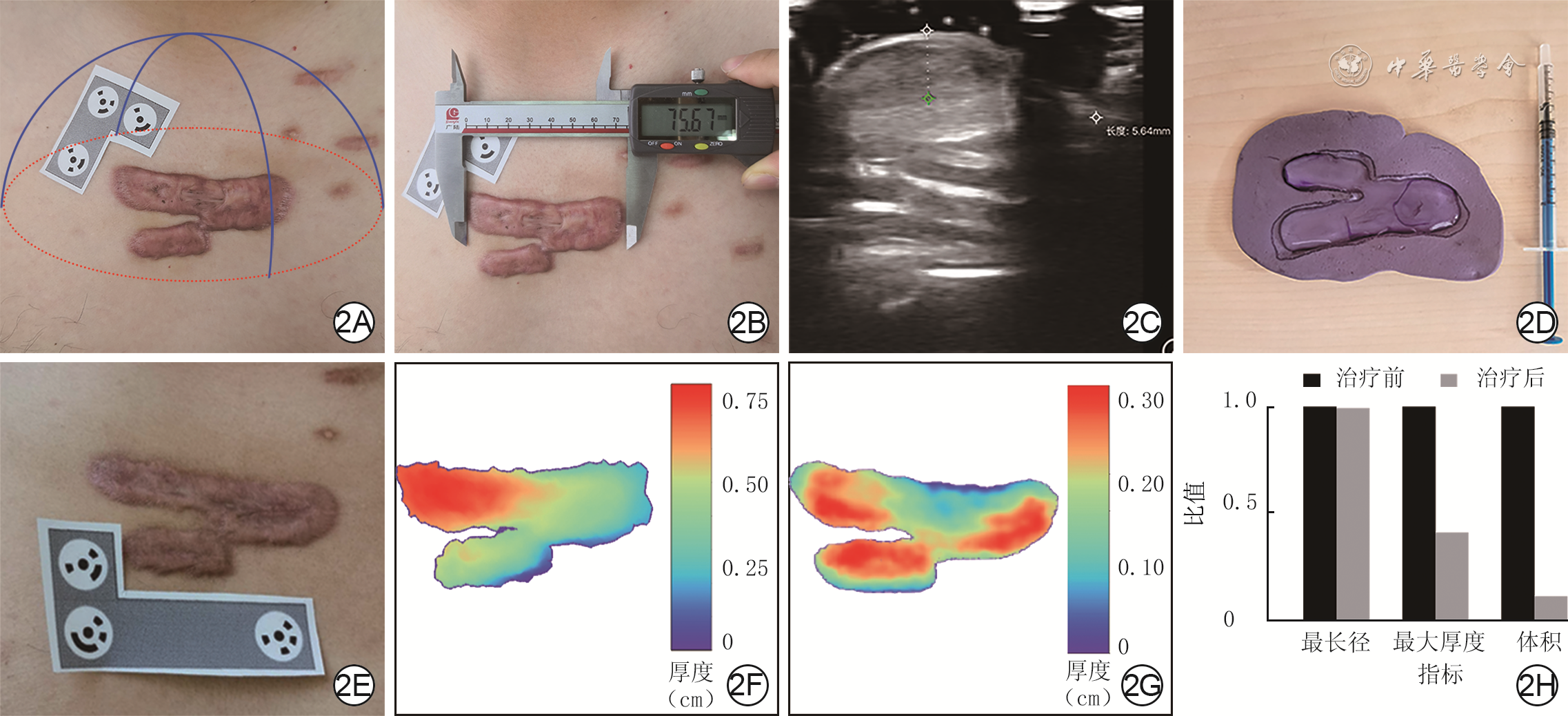
2 采用自主研发的病理性瘢痕三维形态量化评估软件与临床常规方法测量胸部瘢痕疙瘩患者瘢痕的三维形态参数。2A.使用软件对治疗前瘢痕拍照的示意图,在瘢痕周围粘贴标尺贴纸,红色椭圆表示连续拍照的主体为瘢痕和标尺贴纸,蓝色弧线表示软件在不同角度拍照的轨迹;2B.使用游标卡尺测量瘢痕治疗前的最长径;2C.使用手持彩色多普勒超声测量瘢痕治疗前的最大厚度;2D.使用弹性体印模材料在瘢痕治疗前取模,向印模凹槽内注水测量体积;2E.手术+放射治疗后6个月的瘢痕随访照片;2F、2G.分别为瘢痕治疗前后软件生成报告中的高程图,治疗前瘢痕最大厚度处位于图中左上角,约0.70 cm,治疗后最大厚度约为0.30 cm,且分散在瘢痕不同区域;2H.治疗前后的瘢痕三维形态参数对比图(以治疗前为1,计算治疗后与治疗前的比值),瘢痕治疗后的最大厚度、体积均较治疗前明显缩小
表1 自主研发的病理性瘢痕三维形态量化评估软件与临床常规方法测量的54例患者共102处病理性瘢痕的三维形态参数一致性分析
指标 差值平均值 95%一致性界限 平均绝对误差 最长径(cm) -0.07 -0.69~0.55 0.21 最大厚度(cm) -0.02 -0.27~0.24 0.10 体积(mL) -0.07 -0.67~0.53 0.24 注:差值为软件测量与临床常规方法测量结果的差值;软件与临床常规方法测量的最长径、最大厚度、体积的平均绝对百分误差分别为5.75%、21.21%、24.80%  下载: 导出CSV
下载: 导出CSV
-


计量
- 文章访问数: 1364
- HTML全文浏览量: 105
- PDF下载量: 19
- 被引次数: 0
