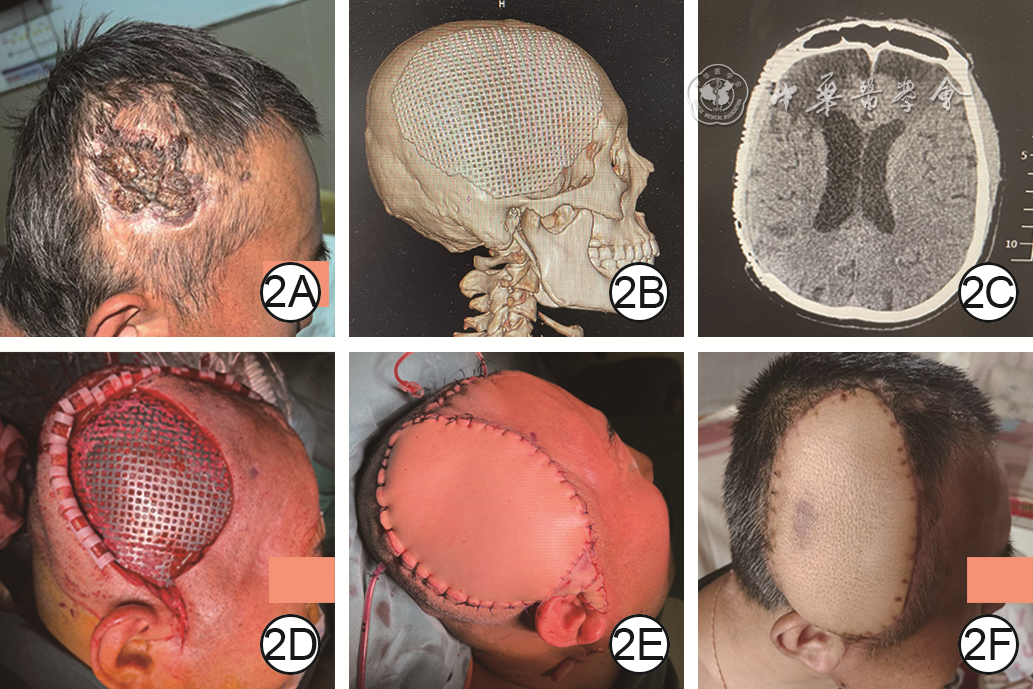
| Citation: | He L,Wang R,Zhu C,et al.Clinical effects of flaps or myocutaneous flaps transplantation after titanium mesh-retaining debridement in repairing the wounds with exposed titanium mesh after cranioplasty[J].Chin J Burns Wounds,2024,40(3):273-280.DOI: 10.3760/cma.j.cn501225-20231031-00163.

|
| [1] |
丛文凯,解东成,刘一然,等.颅骨修补术中应用聚醚醚酮与钛网的临床效果比较[J].中华神经医学杂志,2022,21(4):365-372.DOI: 10.3760/cma.j.cn115354-20220123-00050.
|
| [2] |
PolicicchioD,CasuG,DipellegriniG,et al.Comparison of two different titanium cranioplasty methods: custom-made titanium prostheses versus precurved titanium mesh[J].Surg Neurol Int,2020,11:148.DOI: 10.25259/SNI_35_2020.
|
| [3] |
YaoS, ZhangQ, MaiY, et al. Outcome and risk factors of complications after cranioplasty with polyetheretherketone and titanium mesh: a single-center retrospective study[J]. Front Neurol, 2022, 21,13: 926436. DOI: 10.3389/fneur.2022.926436.
|
| [4] |
SotoE,RestrepoRD,GrantJH3rd,et al.Outcomes of cranioplasty strategies for high-risk complex cranial defects: a 10-year experience[J].Ann Plast Surg,2022,88(5 Suppl 5):S449-454.DOI: 10.1097/SAP.0000000000003019.
|
| [5] |
BaderER,KobetsAJ,AmmarA,et al.Factors predicting complications following cranioplasty[J].J Craniomaxillofac Surg,2022,50(2):134-139.DOI: 10.1016/j.jcms.2021.08.001.
|
| [6] |
闫焦,王继华,何永静,等.颅骨成形术术后钛网外露原因及防治进展[J].中国医疗美容,2019(1):102-107.DOI: 10.19593/j.issn.2095-0721.2019.01.026.
|
| [7] |
MaqboolT,BinhammerA,BinhammerP,et al.Risk factors for titanium mesh implant exposure following cranioplasty[J].J Craniofac Surg,2018,29(5):1181-1186.DOI: 10.1097/SCS.0000000000004479.
|
| [8] |
RohH,KimJ,KimJH,et al.Analysis of complications after cranioplasty with a customized three-dimensional titanium mesh plate[J].World Neurosurg,2019,123:e39-e44.DOI: 10.1016/j.wneu.2018.10.227.
|
| [9] |
张旭,杨理坤,朱洁,等.颅脑创伤行颅骨修补术后发生钛网外露的危险因素分析[J].中华神经外科杂志,2021,37(11):1154-1158.DOI: 10.3760/cma.j.cn112050-20210517-00239.
|
| [10] |
OliverJD,BanuelosJ,Abu-GhnameA,et al.Alloplastic cranioplasty reconstruction: a systematic review comparing outcomes with titanium mesh, polymethyl methacrylate, polyether ether ketone, and norian implants in 3591 adult patients[J].Ann Plast Surg,2019,82(5S Suppl 4):S289-294.DOI: 10.1097/SAP.0000000000001801.
|
| [11] |
YoshiokaN,TominagaS.Titanium mesh implant exposure due to pressure gradient fluctuation[J].World Neurosurg,2018,119:e734-e739.DOI: 10.1016/j.wneu.2018.07.255.
|
| [12] |
陈佳磊,何征晖,冯军峰,等.颅骨缺损修补术后植入物外露的治疗策略及疗效分析[J].中华神经外科杂志,2023,39(4):390-394.DOI: 10.3760/cma.j.cn112050-20220214-00081.
|
| [13] |
YeapMC,TuPH,LiuZH,et al.Long-term complications of cranioplasty using stored autologous bone graft, three-dimensional polymethyl methacrylate, or titanium mesh after decompressive craniectomy: a single-center experience after 596 procedures[J].World Neurosurg,2019,128:e841-e850.DOI: 10.1016/j.wneu.2019.05.005.
|
| [14] |
罗丹,林祥坤,林幼华,等.保留钛网清创并皮瓣转移修复颅骨成形术后钛网外露的治疗体会[J].临床医药实践,2022,31(9):656-657.
|
| [15] |
EhrlichG,KindlingS,WenzH,et al.Immediate titanium mesh implantation for patients with postcraniotomy neurosurgical site infections: safe and aesthetic alternative procedure?[J].World Neurosurg,2017,99:491-499.DOI: 10.1016/j.wneu.2016.12.011.
|
| [16] |
ZhaoYH,FengYH,DengHT,et al.Therapeutic strategies for retention of cranioplasty titanium mesh after mesh exposure[J].Acta Neurochir (Wien),2022,164(12):3101-3106.DOI: 10.1007/s00701-022-05365-w.
|
| [17] |
WangW,VincentA,BahramiA,et al.Progressive scalp thinning over mesh cranioplasty and the role of lipotransfer[J].Laryngoscope,2020,130(8):1926-1931.DOI: 10.1002/lary.28463.
|
| [18] |
ChenB,LiW,ChenD,et al.Partial titanium mesh explantation cured post-cranioplasty implant-associated scalp infection[J].J Clin Neurosci,2017,44:196-202.DOI: 10.1016/j.jocn.2017.06.060.
|
| [19] |
华栋,吴苏州,方小魁,等.带蒂尺动脉腕上皮支皮瓣在颅骨钛网外露创面修复中的应用效果[J].临床医学研究与实践,2022,7(12):86-89.DOI: 10.19347/j.cnki.2096-1413.202212024.
|
| [20] |
DongL,DongY,LiuC,et al.Latissimus dorsi-myocutaneous flap in the repair of titanium mesh exposure and scalp defect after cranioplasty[J].J Craniofac Surg,2020,31(2):351-354.DOI: 10.1097/SCS.0000000000006016.
|
| [21] |
OthmanS,AzourySC,TecceMG,et al.Free flap reconstruction of complex oncologic scalp defects in the setting of mesh cranioplasty: risk factors and outcomes[J].J Craniofac Surg,2020,31(4):1107-1110.DOI: 10.1097/SCS.0000000000006421.
|
| [22] |
计鹏,胡大海,韩夫,等.扩张皮瓣修复钛网颅骨成形术后钛网外露创面的临床效果[J].中华烧伤杂志,2021,37(8):752-757.DOI: 10.3760/cma.j.cn501120-20200613-00306.
|
| [23] |
HanY,ChenY,HanY,et al.The use of free myocutaneous flap and implant reinsertion for staged cranial reconstruction in patients with titanium mesh exposure and large skull defects with soft tissue infection after cranioplasty: report of 19 cases[J].Microsurgery,2021,41(7):637-644.DOI: 10.1002/micr.30800.
|
| [24] |
王耿焕,颜羽,沈和平,等.皮肌瓣一次性分离技术在额颞部颅骨修补术中的应用[J].中华神经外科杂志,2023,39(3):274-278.DOI: 10.3760/cma.j.cn112050-20211108-00532.
|
| [25] |
KooHT,OhJ,HeoCY.Cranioplasty using three-dimensional-printed polycaprolactone implant and free latissimus dorsi musculocutaneous flap in a patient with repeated wound problem following titanium cranioplasty[J].Arch Plast Surg,2022,49(6):740-744.DOI: 10.1055/s-0042-1748656.
|
| [26] |
刘鑫, 韩愚弟, 崔蕾, 等. 分阶段游离背阔肌皮瓣移植及颅骨轮廓重建治疗头部钛网外露合并软组织感染[J]. 中国修复重建外科杂志, 2022, 36(7): 828-833. DOI: 10.7507/1002-1892.202202061.
|
| [27] |
包志军,许济,王治国,等.皮瓣转移修复颅骨修补术后钛网外露[J].中国医师进修杂志,2017,40(3):244-246.DOI: 10.3760/cma.j.jssn.1673-4904.2017.03.015.
|
| [28] |
ZeidermanMR,PuLLQ.Contemporary reconstruction after complex facial trauma[J/OL].Burns Trauma,2020,8:tkaa003[2023-10-31]. https://pubmed.ncbi.nlm.nih.gov/32341916/.DOI: 10.1093/burnst/tkaa003.
|
| [29] |
耿健,刘恒鑫,夏文森.头皮扩张皮瓣联合三维钛网修复颅骨修补术后钛网外露[J].中国美容整形外科杂志,2022,33(4):218-221.DOI: 10.3969/j.issn.1673-7040.2022.04.008.
|
| [30] |
温从吉,王书军,于海洲,等.组织扩张器在头皮缺损伴颅骨外露创面早期修复中的应用[J/CD].中华损伤与修复杂志(电子版),2019,14(6):452-454.DOI: 10.3877/cma.j.issn.1673-9450.2019.06.011.
|
| [31] |
董琛,余州,马显杰.皮肤软组织扩张方法与机制的研究进展[J].中华实验外科杂志,2019,36(8):1513-1517.DOI: 10.3760/cma.j.issn.1001-9030.2019.08.057.
|
| [32] |
马富鑫,任盼,曹瑾,等.三维打印预成形钛网联合游离背阔肌肌瓣在头顶部鳞状细胞癌伴颅骨缺损治疗中的临床应用[J].中华烧伤与创面修复杂志,2022,38(4):341-346.DOI: 10.3760/cma.j.cn501120-20201221-00538.
|
| [33] |
王宇, 孙炜, 王利清, 等. 颅骨修补术后修补材料外露的手术治疗[J]. 青岛大学学报(医学版), 2022, 58(6): 891-895. DOI: 10.11712/jms.2096-5532.2022.58.184.
|
| [34] |
赵卫良,李娟,郑永,等.颅骨修补术后钛网外露的临床特点及手术疗效[J].中华神经创伤外科电子杂志,2021,7(5):297-300.DOI: 10.3877/cma.j.issn.2095-9141.2021.05.009.
|
| [35] |
WeiZ,YangX,LinT,et al.Application of autogenous dermis combined with local flap transplantation in repair of titanium mesh exposure after cranioplasty[J].J Craniofac Surg,2023,34(2):759-763.DOI: 10.1097/SCS.0000000000009118.
|

Figures(3)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd

Lin WP,Mu X,Chen SH,et al.Clinical characteristics of 11 patients with Vibrio vulnificus infection and the establishment of a rapid diagnosis procedure for this disease[J].Chin J Burns Wounds,2024,40(3):266-272.DOI: 10.3760/cma.j.cn501225-20230803-00036.





 DownLoad:
DownLoad: