Abstract:
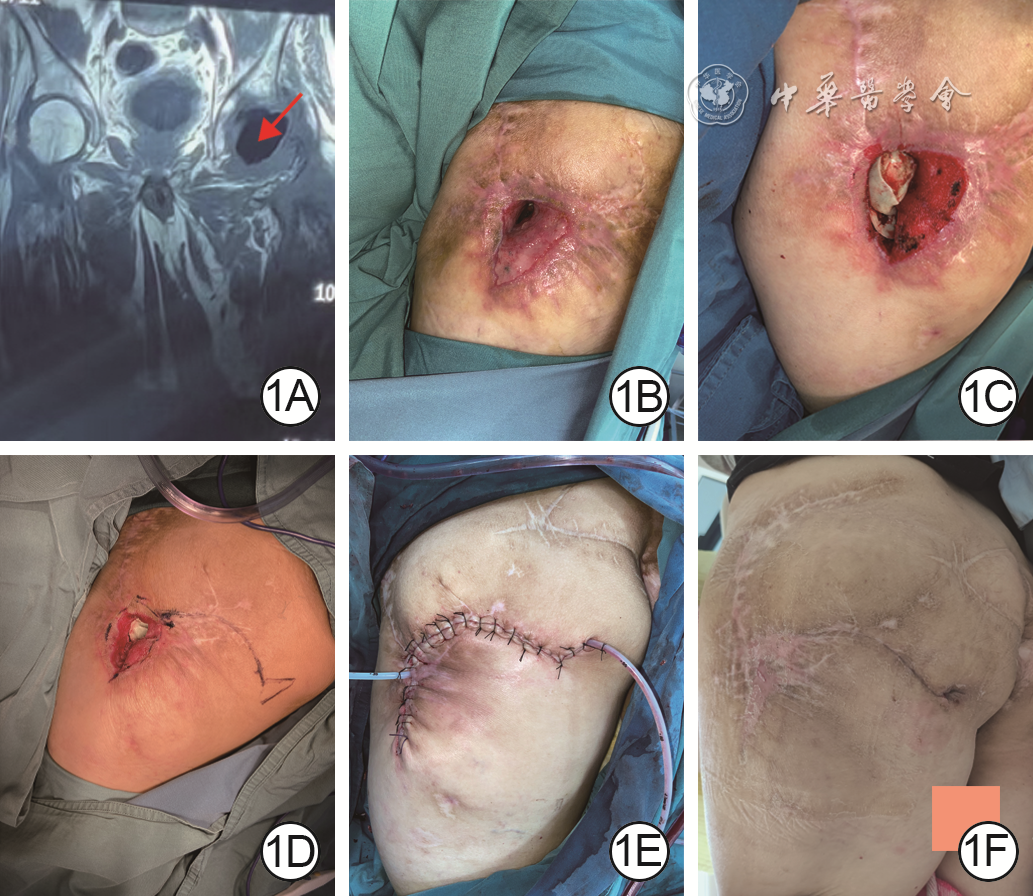
Objective To investigate the clinical efficacy of membrane induction technique combined with local myocutaneous flap in repairing sinus cavity pressure injury in the greater trochanteric region. Methods The study was a retrospective case series study. From January 2020 to January 2023, 12 patients with sinus cavity pressure injury in the greater trochanteric region combined with varying degrees of infection who met the inclusion criteria were admitted to the Department of Burns and Cutaneous Surgery of the First Affiliated Hospital of Air Force Medical University, including 8 males and 4 females, aged 42-76 years. There were 9 patients with unilateral greater trochanteric pressure injury, 3 patients with bilateral greater trochanteric pressure injury, and 3 patients complicated with sepsis. The external wound opening area of pressure injury before debridement was 1.5 cm×1.0 cm-3.0 cm×3.0 cm, and the internal cavity area measured during intraoperative debridement was 10.0 cm×8.5 cm-20.0 cm×10.0 cm. After the general condition of the whole body was improved, the covering/filling with antibiotic bone cement after debridement was performed in stage Ⅰ, the wound was repaired with local myocutaneous flap with the area of 10.0 cm×9.0 cm-22.5 cm×11.5 cm in stage Ⅱ, and the wound in the donor area was sutured directly. The levels of inflammatory indicators including white blood cell count, C-reactive protein, procalcitonin, and erythrocyte sedimentation rate, as well as the positive proportions of bacterial culture in wound exudation samples of all patients before and 7 days after the stage Ⅰ operation were compared. The mental status, body temperature, heart rate, and respiratory rate of patients complicated with sepsis before and 3 days after the stage Ⅰ operation were recorded. The survival of local myocutaneous flap and wound healing were observed in all patients after the stage Ⅱ operation. The recurrence of pressure injury and the appearance and texture of the flap were followed up in all patients. Results Compared with those before stage Ⅰ operation, the white blood cell count, C-reactive protein level, procalcitonin level, and erythrocyte sedimentation rate of 12 patients on post stage Ⅰ operation day 7 were significantly decreased (with t values of 6.67, 7.71, 2.72, and 3.52, respectively, P<0.05). The proportion of positive bacterial culture in wound exudation samples on post stage Ⅰ operation day 7 was 2/12, which was significantly lower than 11/12 before stage Ⅰ operation ( P<0.05). The mental state of 3 patients complicated with sepsis improved significantly 3 days after stage Ⅰ operation, which was improved as compared with that before stage Ⅰ operation, their body temperature returned to normal, heart rate was <90 times/min, and respiratory rate was <20 times/min. A total of 15 wounds were repaired by local myocutaneous flaps, 14 local myocutaneous flaps survived well after stage Ⅱ operation and the wounds were healed, while a partial necrosis occurred at the distal end of one local myocutaneous flap, which was healed 14 days after bedside debridement and suturing. Follow-up for 3 to 24 months after stage Ⅱ operation showed that the pressure injury was not recurrent in any patient, the flap was not bloated, the color of the flap was similar to the surrounding skin tissue, and the flap texture was soft. Conclusions Membrane induction technique combined with local myocutaneous flap in the treatment of sinus cavity pressure injury in the greater trochanteric region can decrease the level of inflammatory indicators and alleviate the bacterial load of the wound by covering or filling with antibiotic bone cement, and form the induction membrane to provide a good basis for stage Ⅱ wound repair. The local myocutaneous flap shows good clinical effects including a high survival rate, few complications, and the recurrence rate of postoperative pressure injury was low.
Tong Lin,Zhang Wanfu,Han Fei,et al.Clinical efficacy of membrane induction technique combined with local myocutaneous flap in repairing sinus cavity pressure injury in the greater trochanteric region[J].Chin J Burns Wounds,2024,40(4):1-7.DOI: 10.3760/cma.j.cn501225-20231029-00144.



 Abstract
Abstract PDF
PDF