



Clinical effects of transplantation of turbocharged bipedicle deep inferior epigastric perforator flap in breast reconstruction
-
摘要:
目的 探讨移植内增压式双侧血管蒂腹壁下动脉穿支皮瓣行乳房再造的临床效果。 方法 采用回顾性观察性研究。2008年12月—2016年12月湖南省肿瘤医院整形外科收治24例符合入选标准的乳腺癌术后患者,均为女性,年龄28~51(36.5±1.6)岁,均采用内增压式双侧血管蒂腹壁下动脉穿支皮瓣行Ⅱ期乳房再造。根据内增压吻合血管类型,将内增压式双侧血管蒂腹壁下动脉穿支皮瓣分为3种类型:吻合血管蒂主干远端型、吻合血管蒂主干主要分支型和吻合血管蒂肌支型。皮瓣长(27.5±0.3)cm、宽(12.8±1.4)cm。供瓣区予以彻底止血后,间断缝合修补前鞘,完成脐重建,留置2根负压引流管,逐层缝合皮下组织及皮肤。皮瓣血管蒂与受区胸廓内血管吻合具体方式包括吻合1支动脉和1支静脉近端、吻合1支动脉和1支静脉近远端、吻合1支动脉和2支静脉近端。术后观察皮瓣成活、血运情况。随访观察再造乳房外形满意度、供区并发症、腹壁功能及瘢痕增生情况。 结果 术后,采用内增压式双侧血管蒂腹壁下动脉穿支皮瓣行Ⅱ期乳房再造术患者的皮瓣均顺利成活且血运良好。随访14~56(20±6)个月,患者再造乳房外形满意,腹部供区无并发症且仅遗留线性瘢痕,腹壁功能无明显受限。 结论 对有明确适应证的患者行游离内增压式双侧血管蒂腹壁下动脉穿支皮瓣移植,是自体组织乳房再造安全可靠、效果满意的选择方案。 Abstract:Objective To explore the clinical effects of transplantation of turbocharged bipedicle deep inferior epigastric perforator (DIEP) flap in breast reconstruction. Methods A retrospective observational study was used. From December 2008 to December 2016, 24 patients who met the inclusion criteria were treated in the Department of Plastic Surgery of Hunan Cancer Hospital, all patients were female, aged 28-51 (36.5±1.6) years. All cases received turbocharged bipedicle DIEP flap for two-staged breast reconstruction. According to the patterns of turbocharged vessels anastomosis, the turbocharged bipedicle DIEP flaps with length of (27.5±0.3) cm and width of (12.8±1.4) cm, were divided into three types: distal end of pedicle anastomosis type, main branch of pedicle anastomosis type, and muscular branch of pedicle anastomosis type. After complete hemostasis in the donor region, the anterior sheath was repaired with intermittent suture, and umbilical reconstruction was completed. Two negative pressure drainage tubes were indwelled, and subcutaneous tissue and skin were sutured layer by layer. The specific ways of vascular anastomosis of the flap pedicle with the internal thoracic vessels of recipient site included anastomosing the proximal end of one artery and one vein, anastomosing the proximal and distal end of one artery and one vein, and anastomosing the proximal end of one artery and two veins. Postoperatively, the survival and blood supply of flaps were observed. The patients were followed up to observe the reconstructed breast shape satisfaction, donor site complications, abdominal wall function, and scar hyperplasia. Results All turbocharged bipedicle DIEP flaps for two-staged breast reconstruction survived well, with good blood supply. During follow-up for 14 to 56 (20±6) months, the shape of reconstructed breasts was satisfied. Only linear scar was left in the donor sites of abdomen with no complications, and the function of abdominal wall was not affected. Conclusions For patients with clear indications, transplantation of free turbocharged bipedicle DIEP flap is a safe, reliable, and satisfactory choice for breast reconstruction with autologous tissue. -
Key words:
- Surgical flaps /
- Mammaplasty /
- Skin /
- Turbocharge /
- Deep inferior epigastric perforator flap
-
参考文献
(27) [1] KoshimaI,MoriguchiT,FukudaH,et al.Free, thinned, paraumbilical perforator-based flaps[J].J Reconstr Microsurg,1991,7(4):313-316. [2] AllenRJ,TreeceP.Deep inferior epigastric perforator flap for breast reconstruction[J].Ann Plast Surg,1994,32(1):32-38.DOI: 10.1097/00000637-199401000-00007. [3] 宋达疆,李赞,周晓,等.局部晚期乳腺癌切除术后巨大复杂创面的整形外科修复[J].中华整形外科杂志,2018,34(8):630-635.DOI: 10.3760/cma.j.issn.1009-4598.2018.08.011. [4] SongD,LiuD,PafitanisG,et al.Extensive microsurgical reconstruction of chest wall defects for locally advanced breast cancer: a 10-year single-unit experience[J].Ann Plast Surg,2020,84(3):293-299.DOI: 10.1097/SAP.0000000000002000. [5] DemiriEC,TsimponisA,PagkalosA,et al.Fat-augmented latissimus dorsi versus deep inferior epigastric perforator flap: comparative study in delayed autologous breast reconstruction[J].J Reconstr Microsurg,2021,37(3):208-215.DOI: 10.1055/s-0040-1716348. [6] TaylorGI,PalmerJH.The vascular territories (angiosomes) of the body: experimental study and clinical applications[J].Br J Plast Surg,1987,40(2):113-141.DOI: 10.1016/0007-1226(87)90185-8. [7] MoonHK,TaylorGI.The vascular anatomy of rectus abdominis musculocutaneous flaps based on the deep superior epigastric system[J].Plast Reconstr Surg,1988,82(5):815-832.DOI: 10.1097/00006534-198811000-00014. [8] IngvaldsenCA,TønsethKA,PrippAH,et al.Microcirculatory evaluation of the abdominal skin in breast reconstruction with deep inferior epigastric artery perforator flap[J].Plast Reconstr Surg Glob Open,2016,4(2):e616.DOI: 10.1097/GOX.0000000000000602. [9] HartrampfCR,ScheflanM,BlackPW.Breast reconstruction with a transverse abdominal island flap[J].Plast Reconstr Surg,1982,69(2):216-225.DOI: 10.1097/00006534-198202000-00006. [10] RozenWM, WhitakerIS, AshtonMW. A combined anatomical and clinical study for quantitative analysis of the microcirculation in the classic perfusion zones of the deep inferior epigastric artery perforator flap[J]. Plast Reconstr Surg,2011,128(3):821-822.DOI: 10.1097/PRS.0b013e3182221525. [11] BaileySH,Saint-CyrM,WongC,et al.The single dominant medial row perforator DIEP flap in breast reconstruction: three- dimensional perforasome and clinical results[J].Plast Reconstr Surg,2010,126(3):739-751.DOI: 10.1097/PRS.0b013e3181e5f844. [12] PatelNG,RamakrishnanV.Microsurgical tissue transfer in breast reconstruction[J].Clin Plast Surg,2020,47(4):595-609.DOI: 10.1016/j.cps.2020.06.010. [13] TeotiaSS,DickeyRM,LiuY,et al.Intraoperative microvascular complications in autologous breast reconstruction: the effects of resident training on microsurgical outcomes[J].J Reconstr Microsurg,2021,37(4):309-314.DOI: 10.1055/s-0040-1716404. [14] BhullarH,Hunter-SmithDJ,RozenWM.Fat necrosis after DIEP flap breast reconstruction: a review of perfusion-related causes[J].Aesthetic Plast Surg,2020,44(5):1454-1461.DOI: 10.1007/s00266-020-01784-1. [15] HallockGG.The complete nomenclature for combined perforator flaps[J].Plast Reconstr Surg,2011,127(4):1720-1729.DOI: 10.1097/PRS.0b013e31820a662b. [16] HallockGG.Branch-based conjoined perforator flaps[J].Plast Reconstr Surg,2008,121(5):1642-1649.DOI: 10.1097/PRS.0b013e31816aa022. [17] PenningtonDG,NettleWJ,LamP.Microvascular augmentation of the blood supply of the contralateral side of the free transverse rectus abdominis musculocutaneous flap[J].Ann Plast Surg,1993,31(2):123-126; discussion 126-127.DOI: 10.1097/00000637-199308000-00006. [18] 宋达疆,李赞,周晓,等.股薄肌皮瓣联合大收肌穿支皮瓣在乳房重建中的应用[J].中国修复重建外科杂志,2018,32(6):707-713.DOI: 10.7507/1002-1892.201801001. [19] TugertimurB,DecW.Deep inferior epigastric artery perforator flap reconstruction for breast burn deformities[J].Plast Reconstr Surg Glob Open,2020,8(7):e2981.DOI: 10.1097/GOX.0000000000002981. [20] 张世民,宋达疆.穿支皮瓣的发现发展历史与临床启示[J].中国修复重建外科杂志,2017,31(7):769-772.DOI: 10.7507/1002-1892.201701082. [21] HolmC,MayrM,HöfterE,et al.Perfusion zones of the DIEP flap revisited: a clinical study[J].Plast Reconstr Surg,2006,117(1):37-43.DOI: 10.1097/01.prs.0000185867.84172.c0. [22] BoerVB,van WingerdenJJ,WeverCF,et al.Perforator mapping practice for deep inferior epigastric artery perforator flap reconstructions: a survey of the benelux region[J].J Reconstr Microsurg,2021,37(2):111-118.DOI: 10.1055/s-0040-1714427. [23] WongC,Saint-CyrM,MojallalA,et al.Perforasomes of the DIEP flap: vascular anatomy of the lateral versus medial row perforators and clinical implications[J].Plast Reconstr Surg,2010,125(3):772-782.DOI: 10.1097/PRS.0b013e3181cb63e0. [24] HillbergNS,van MulkenT,Meesters-CabergM,et al.Autologous breast reconstruction with a delay procedure of the deep inferior epigastric artery perforator flap because of venous congestion of the flap on pedicle: a case series[J].Ann Plast Surg,2019,82(5):537-540.DOI: 10.1097/SAP.0000000000001752. [25] AgarwalJP,GottliebLJ.Double pedicle deep inferior epigastric perforator/muscle-sparing TRAM flaps for unilateral breast reconstruction[J].Ann Plast Surg,2007,58(4):359-363.DOI: 10.1097/01.sap.0000239818.28900.81. [26] CuiH,DingM,MaoY,et al.Three-dimensional visualization for extended deep inferior epigastric perforator flaps[J].Ann Plast Surg,2020,85(6):e48-e53.DOI: 10.1097/SAP.0000000000002379. [27] O'NeillAC, HaywardV, ZhongT, et al. Usability of the internal mammary recipient vessels in microvascular breast reconstruction[J]. J Plast Reconstr Aesthet Surg,2016 ,69(7):907-911. DOI: 10.1016/j.bjps.2016.01.030. -

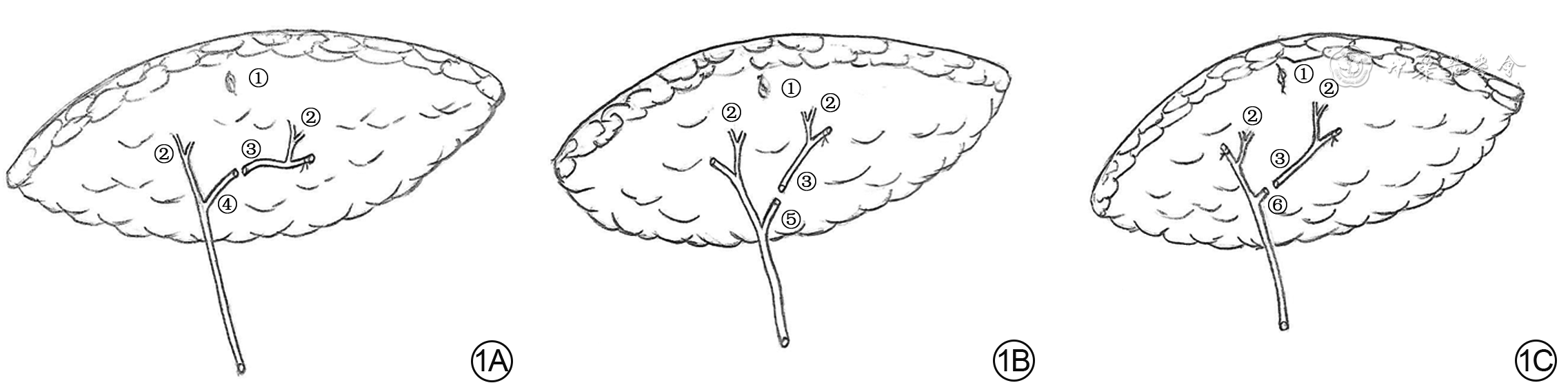
1 3种携带双侧血管蒂的腹壁下动脉穿支皮瓣内增压类型示意图。1A.对侧血管蒂与同侧血管蒂主干远端吻合型;1B. 对侧血管蒂与同侧血管蒂主干主要分支吻合型;1C.对侧血管蒂与同侧血管蒂肌支吻合型
注:①、②、③、④、⑤、⑥分别表示脐、穿支血管、对侧血管蒂、同侧血管蒂主干远端、同侧血管蒂主要分支、同侧血管蒂肌支

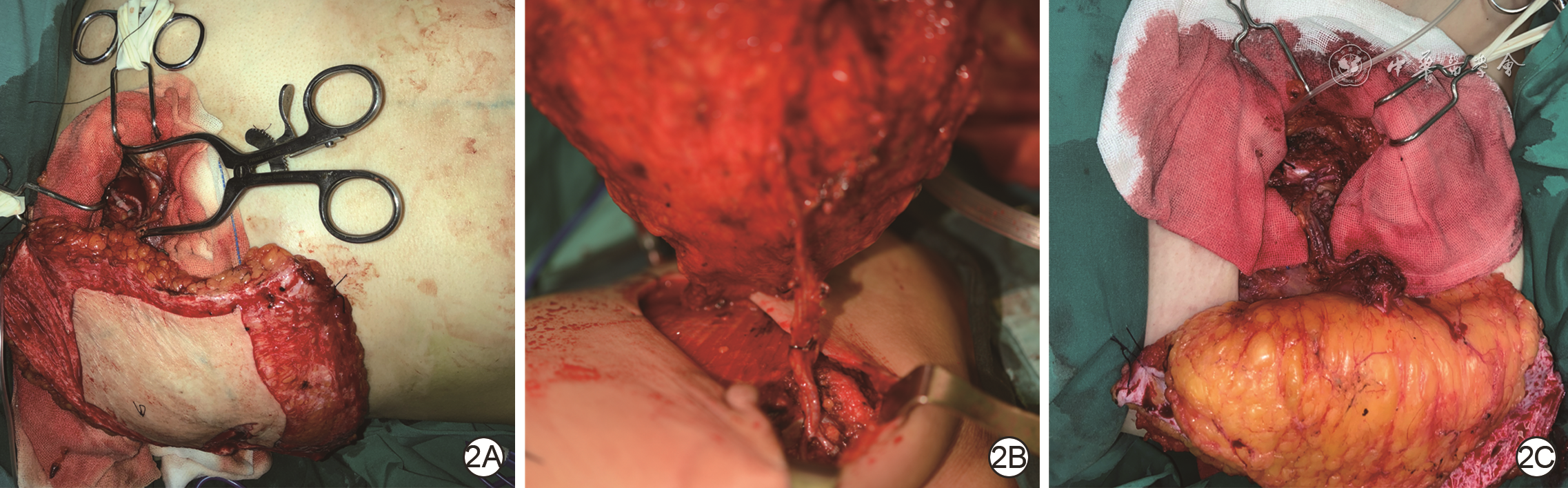
2 内增压式游离腹壁下动脉穿支皮瓣在乳房再造中的血运重建方式。2A.腹壁下动脉穿支吻合胸廓内1支动脉和1支静脉近端;2B.腹壁下动脉穿支吻合胸廓内1支动脉和1支静脉近远端;2C.腹壁下动脉穿支吻合胸廓内1支动脉和2支静脉近端

3 例1患者游离移植内增压式双侧血管蒂腹壁下动脉穿支皮瓣再造乳房。3A.术中设计,根据供区、受区情况确定手术范围;3B.受区胸廓内血管准备,显露左侧胸廓内动脉及其伴行静脉备用;3C.分离右侧腹壁血管蒂至接近其发出平面;3D.分离左侧腹壁下动脉穿支及血管蒂至其接近发出平面;3E.将右腹壁下动静脉近端与左腹壁下动静脉的肌支进行端端吻合,形成内增压;3F.内增压完成后,进一步完成左腹壁下动静脉和胸廓内动静脉近远端的端端吻合;3G.术后即刻;3H.术后32个月随访,乳房外形满意,腹部供区仅遗留线性瘢痕
注:图3F中的①、②分别表示右侧腹壁下血管近端、左侧腹壁下血管
-

 下载:
下载:


图(4)
计量
- 文章访问数: 987
- HTML全文浏览量: 162
- PDF下载量: 100
- 被引次数: 0
