



Prospective study on the analysis of intestinal microflora changes and prediction on metabolic function in severe burn patients at early stage by 16S ribosomal RNA high-throughput sequencing
-
摘要:
目的 基于16S核糖体RNA(16S rRNA)高通量测序分析严重烧伤患者早期肠道菌群变化并进行代谢功能预测。 方法 本前瞻性观察性研究将2018年1月—2019年12月江苏大学附属医院烧伤整形科收治的48例符合入选标准的严重烧伤患者纳入烧伤组,将同时期于江苏大学附属医院体检中心进行健康检查的符合入选标准的40名健康志愿者纳入健康组。收集烧伤组患者入院后1周左右的粪便标本及健康组志愿者体检当天粪便标本,进行16S rRNA V4区基因测序,分析各类菌属的相对丰度;应用Mothur软件进行操作分类单元(OTU)划分,分析优势菌群;通过QIIME1.9.0软件分析粪便菌群OTU数目、Chao1指数、Ace指数、Shannon指数;采用Canoco Software 5.0对粪便菌群相对丰度做主成分分析;采用京都基因和基因组数据库预测粪便菌群代谢功能。对数据行独立样本t检验、Mann-Whitney U检验。 结果 烧伤组患者粪便中拟杆菌属、肠球菌属、不动杆菌属、巨球型菌属、葡萄球菌属相对丰度明显高于健康组志愿者(Z=-5.20、-2.37、-5.17、-4.41、-6.03,P<0.05或P<0.01),而健康组志愿者粪便中未分类的毛螺杆菌科、普氏菌属、盲杆菌属、未分类的瘤胃球菌科、假丁酸弧菌属、布劳特菌属、未分类的消化链球菌科(Z=-8.03、-3.21、-7.63、-5.88、-8.05、-8.05、-6.77, P<0.01)等19种菌属的相对丰度明显高于烧伤组患者。健康组志愿者粪便菌群多样性优于烧伤组患者,其主要优势菌群为拟杆菌属、未分类的毛螺杆菌科、普氏菌属、未分类的肠杆菌科、布劳特菌属、副拟杆菌属和大肠志贺杆菌属等,而烧伤组患者粪便主要优势菌群为拟杆菌属、普氏菌属、未分类的肠杆菌科和副拟杆菌属。烧伤组患者粪便菌群OTU数目、Ace指数、Chao1指数、Shannon指数分别为(149±47)个、199±45、190±45、2.0±0.9,显著少/低于健康组志愿者的(266±57)个、323±51、318±51、3.8±0.5(t=10.325、11.972、12.224、11.662,P<0.01)。健康组志愿者和烧伤组患者粪便菌群相对丰度在主成分1 被清晰地区分为2个群体,主成分1贡献率为32.50%,P<0.01;健康组志愿者粪便菌群在主成分2上较为集中,烧伤组患者粪便菌群在主成分2上散布较大,主成分2贡献率为13.44%,P>0.05。烧伤组患者粪便菌群氨基酸中丙氨酸-天冬氨酸-谷氨酸、精氨酸-脯氨酸、半胱氨酸-蛋氨酸、甘氨酸-丝氨酸-苏氨酸、苯丙氨酸、色氨酸、酪氨酸以及碳水化合物中三羧酸循环、果糖和甘露糖、半乳糖、酵解/糖异生、淀粉和蔗糖代谢水平显著低于健康组志愿者(Z=-4.75、-4.54、-4.75、-4.62、-3.71、-3.28、-4.19,-3.82、-4.72、-4.35、-4.75、-4.71,P<0.01),硫辛酸代谢和辅酶Q合成水平明显高于健康组志愿者(Z= -6.07、-4.51,P<0.01),花生四烯酸代谢水平与健康组志愿者相近(P>0.05)。 结论 基于16S rRNA高通量测序得出,严重烧伤患者早期肠道菌群和健康人群存在明显差异,烧伤患者肠道菌群种类减少,多样性降低,营养代谢水平降低。 Abstract:Objective To analyze the changes of intestinal microflora and to predict the metabolic function of intestinal microflora in severe burn patients at early stage by 16S ribosomal RNA (rRNA) high-throughput sequencing. Methods In this prospective observational study, 48 patients with severe burns who met the inclusion criteria were admitted to Department of Burns and Plastic Surgery of Affiliated Hospital of Jiangsu University from January 2018 to December 2019 were included in burn group, and 40 healthy volunteers who met the inclusion criteria and underwent physical examination at the Physical Examination Center of Affiliated Hospital of Jiangsu University in the same period were included in healthy group. Fecal samples were collected from patients in burn group in about 1 week after admission and from volunteers in healthy group on the day of physical examination. The 16S rRNA V4 gene sequencing was performed in the feces of patients in burn group and volunteers in healthy group to analyze the relative abundance of various bacteria. The operational classification unit (OTU) was divided by Mothur software to analyze the dominant bacteria. The OTU number, Chao1 index, Ace index, and Shannon index of fecal microflora were analyzed by QIIME1.9.0 software. The principal component analysis for relative abundance of fecal microflora was performed by Canoco Software 5.0. The metabolic function of fecal microflora was predicted by Kyoto Encyclopedia of Genes and Genomes. Data were statistically analyzed with independent sample t test, and Mann-Whitney U test, and Bonferroni correction. Results The relative abundance of Bacteroides, Enterococcus, Acinetobacter, Macrococcus, and Staphylococcus in feces of patients in burn group was significantly higher than that of volunteers in healthy group (Z=-5.20, -2.37, -5.17, -4.41, -6.03, P<0.05 or P<0.01), and the relative abundance of unclassified-Helicobacillae, Prevotella, Cecobacteria, unclassified-Rumencocci, Pseudobutyrivibrio, Brautia, and unclassified-Digiestive Streptococcaceae (Z=-8.03, -3.21, -7.63, -5.88, -8.05, -8.05, -6.77, P<0.01) and other 12 species of bacteria in the feces of volunteers in healthy group was significantly higher than that of patients in burn group. The diversity of fecal microflora of volunteers in healthy group was better than that of patients in burn group, the main dominant microflora of volunteers in healthy group were Bacteroides, unclassified-Helicobacillae, Prevotella, unclassified- Enterobacteriaceae, Brautia, Parabacteroides, Escherichia coli, etc., and the main dominant microflora of patients in burn group were Bacteroides, Prevotella, unclassified-Enterobacteriaceae, and Parabacteroides. The OTU number, Ace index, Chao1 index, and Shannon index of fecal microflora of patients in burn group were 149±47, 199±45, 190±45, 2.0±0.9, which were significantly lower than 266±57, 323±51, 318±51, 3.8±0.5 of volunteers in healthy group (t=10.325, 11.972, 12.224, 11.662, P<0.01). The relative abundance of fecal microflora of patients in burn group and volunteers in healthy group was clearly divided into two groups by principal component 1, and the contribution rate of principal component 1 was 32.50%, P<0.01. The fecal microflora of volunteers in healthy group were more concentrated on principal component 2, the fecal microflora of patients in burn group were dispersed in principal component 2, and the contribution rate of principal component 2 was 13.44%, P>0.05. The metabolic levels of alanine-aspartate-glutamate, arginine- proline, cysteine-methionine, glycine-serine-threonine, phenylalanine, tryptophan, and tyrosine in amino acid, tricarboxylic acid cycle, glucose and mannose, galactolipin, glycolysis/gluconiogenesis, starch and sucrose in carbohydrate of fecal microflora of patients in burn group were significantly lower than those of volunteers in healthy group (Z=-4.75, -4.54, -4.75, -4.62, -3.71, -3.28, -4.19, -3.82, -4.72, -4.35, -4.75, -4.71, P<0.01). The levels of lipoic acid metabolism and coenzyme Q synthesis of fecal microflora of patients in burn group were significantly higher than those of volunteers in healthy group (Z=-6.07, -4.51, P<0.01). The metabolic level of arachidonic acid of fecal microflora of patients in burn group was similar to that of volunteers in healthy group (P>0.05). Conclusions There are significant differences in intestinal microflora between severe burn patients at the early stage and healthy people, and the species and diversity of microflora are decreased, and the nutrient metabolism level is decreased in burn patients by 16S rRNA high-throughput sequencing. -
参考文献
(31) [1] SandersME,MerensteinDJ,ReidG,et al.Probiotics and prebiotics in intestinal health and disease: from biology to the clinic[J].Nat Rev Gastroenterol Hepatol,2019,16(10):605-616.DOI: 10.1038/s41575-019-0173-3. [2] WangC,LiQ,RenJ.Microbiota-immune interaction in the pathogenesis of gut-derived infection[J].Front Immunol,2019,10:1873.DOI: 10.3389/fimmu.2019.01873. [3] WallaceTC,GuarnerF,MadsenK,et al.Human gut microbiota and its relationship to health and disease[J].Nutr Rev,2011,69(7):392-403.DOI: 10.1111/j.1753-4887.2011.00402.x. [4] BeckmannN,PughAM,CaldwellCC.Burn injury alters the intestinal microbiome's taxonomic composition and functional gene expression[J].PLoS One,2018,13(10):e0205307.DOI: 10.1371/journal.pone.0205307. [5] 张军毅,朱冰川,徐超,等. 基于分子标记的宏基因组16S rRNA基因高变区选择策略[J].应用生态学报,2015,26(11):3545- 3553. [6] 吴悦妮,冯凯,厉舒祯,等.16S/18S/ITS扩增子高通量测序引物的生物信息学评估和改进[J].微生物学通报,2020,47(9):2897-2912.DOI: 10.13344/j.microbiol.china.200054. [7] ParkS,ChoiHS,LeeB,et al.hc-OTU: a fast and accurate method for clustering operational taxonomic units based on homopolymer compaction[J].IEEE/ACM Trans Comput Biol Bioinform,2018,15(2):441-451.DOI: 10.1109/TCBB.2016.2535326. [8] 黄树武,闵凡贵,王静,等.常见SPF级小鼠和大鼠肠道菌群多样性研究[J].中国实验动物学报,2019,27(2):229-235.DOI: 10.3969/j.issn.1005-4847.2019.02.016. [9] 罗亚,唐贇,张丁,等.不同年龄大熊猫肠道菌群及其酶活特征分析[J].畜牧兽医学报,2020,51(4):763-771.DOI: 10.11843/j.issn.0366-6964.2020.04.012. [10] SegataN,IzardJ,WaldronL,et al.Metagenomic biomarker discovery and explanation[J].Genome Biol,2011,12(6):R60.DOI: 10.1186/gb-2011-12-6-r60. [11] RametteA.Multivariate analyses in microbial ecology[J].FEMS Microbiol Ecol,2007,62(2):142-160.DOI: 10.1111/j.1574-6941.2007.00375.x. [12] HuJ,BaoY,ZhuY,et al.The preliminary study on the association between PAHs and air pollutants and microbiota diversity[J].Arch Environ Contam Toxicol,2020,79(3):321-332.DOI: 10.1007/s00244-020-00757-4. [13] 袁林,李万利,杜晨红,等.黄连解毒散和黄霉素对不同日龄肉鸡回肠菌群结构的影响[J].河南农业科学,2020,49(2):142-149.DOI: 10.15933/j.cnki.1004-3268.2020.02.019. [14] 陈宾,况芳,李孝建,等.四例严重烧伤患者并发早期急性肾损伤的原因及治疗方法分析[J].中华烧伤杂志,2019,35(2):110-115.DOI: 10.3760/cma.j.issn.1009-2587.2019.02.006. [15] 刘峰,黄正根,彭毅志,等.严重烧伤早期行连续性血液净化治疗的可行性及疗效随机对照临床试验[J].中华烧伤杂志,2016,32(3):133-139.DOI: 10.3760/cma.j.issn.1009-2587.2016.03.002. [16] 李晓亮,肖宏涛,李延仓,等.柠檬酸对行连续性肾脏替代治疗的严重烧伤并发急性肾损伤患者的影响[J].中华烧伤杂志,2019,35(8):568-573.DOI: 10.3760/cma.j.issn.1009-2587.2019.08.003. [17] Sebastián DomingoJJ,SánchezSánchez C.From the intestinal flora to the microbiome[J].Rev Esp Enferm Dig,2018,110(1):51-56.DOI: 10.17235/reed.2017.4947/2017. [18] LynchSV,PedersenO.The human intestinal microbiome in health and disease[J].N Engl J Med,2016,375(24):2369-2379.DOI: 10.1056/NEJMra1600266. [19] KataokaK.The intestinal microbiota and its role in human health and disease[J].J Med Invest,2016,63(1/2):27-37.DOI: 10.2152/jmi.63.27. [20] HuangG,SunK,YinS,et al.Burn injury leads to increase in relative abundance of opportunistic pathogens in the rat gastrointestinal microbiome[J].Front Microbiol,2017,8:1237.DOI: 10.3389/fmicb.2017.01237. [21] ZhangDY,QiuW,JinP,et al.Role of autophagy and its molecular mechanisms in mice intestinal tract after severe burn[J].J Trauma Acute Care Surg,2017,83(4):716-724.DOI: 10.1097/TA.0000000000001624. [22] TapkingC,PoppD,HerndonDN,et al.Cardiac dysfunction in severely burned patients: current understanding of etiology, pathophysiology, and treatment[J].Shock,2020,53(6):669-678.DOI: 10.1097/SHK.0000000000001465. [23] SavetamalA.Infection in elderly burn patients: what do we know?[J].Surg Infect (Larchmt),2021,22(1):65-68.DOI: 10.1089/sur.2020.322. [24] SalyerCE,BomholtC,BeckmannN,et al.Novel therapeutics for the treatment of burn infection[J].Surg Infect (Larchmt),2021,22(1):113-120.DOI: 10.1089/sur.2020.104. [25] LiuJ,LiuY,LiuS,et al.Hypocoagulation induced by broad-spectrum antibiotics in extensive burn patients[J/OL].Burns Trauma,2019,7:13[2020-09-16].https://pubmed.ncbi.nlm.nih.gov/31058197/. DOI: 10.1186/s41038-019-0150-7. [26] 王泽臣 烧伤患者创面菌群分布变化及创面感染影响因素分析 天津 天津医科大学 2015 王泽臣. 烧伤患者创面菌群分布变化及创面感染影响因素分析[D]. 天津:天津医科大学, 2015.
[27] 张莎莎, 吴振聪, 杨转, 等. 利用Illumina Miseq测序技术研究鲍内脏多肽对小鼠肠道微生物的影响[J]. 安徽农业科学, 2019, 47(8):93-97. DOI: 10.3969/j.issn.0517-6611.2019.08.024. [28] OjuederieOB, BalogunMO, AkandeSR, et al. Intraspecific variability in agro-morphological traits of African yam bean Sphenostylis stenocarpa (Hochst ex. A. Rich) harms[J]. Journal of Crop Science & Biotechnology, 2015, 18(2):53-62. DOI: 10.1007/s12892-014-0109-y. [29] 雍和礼, 刘宓, 宁磊. 重症胰腺炎患者感染病原菌耐药及相关因素分析[J]. 中国病原生物学杂志, 2015, 10(11):1035-1039. DOI: 10.13350/j.cjpb.151118. [30] 王津, 刘爽, 邹妍,等. 膳食纤维和肠道微生物及相关疾病的研究进展[J]. 食品研究与开发, 2020, 41(11):201-207. DOI: 10.12161/j.issn.1005-6521.2020.11.033. [31] QuraishiMNN, YalchinM, BlackwellC, et al. STOP-colitis pilot trial protocol: a prospective, open-label, randomised pilot study to assess two possible routes of faecal microbiota transplant delivery in patients with ulcerative colitis[J]. BMJ Open,2019,9(11):e030659. DOI: 10.1136/bmjopen-2019-030659. -

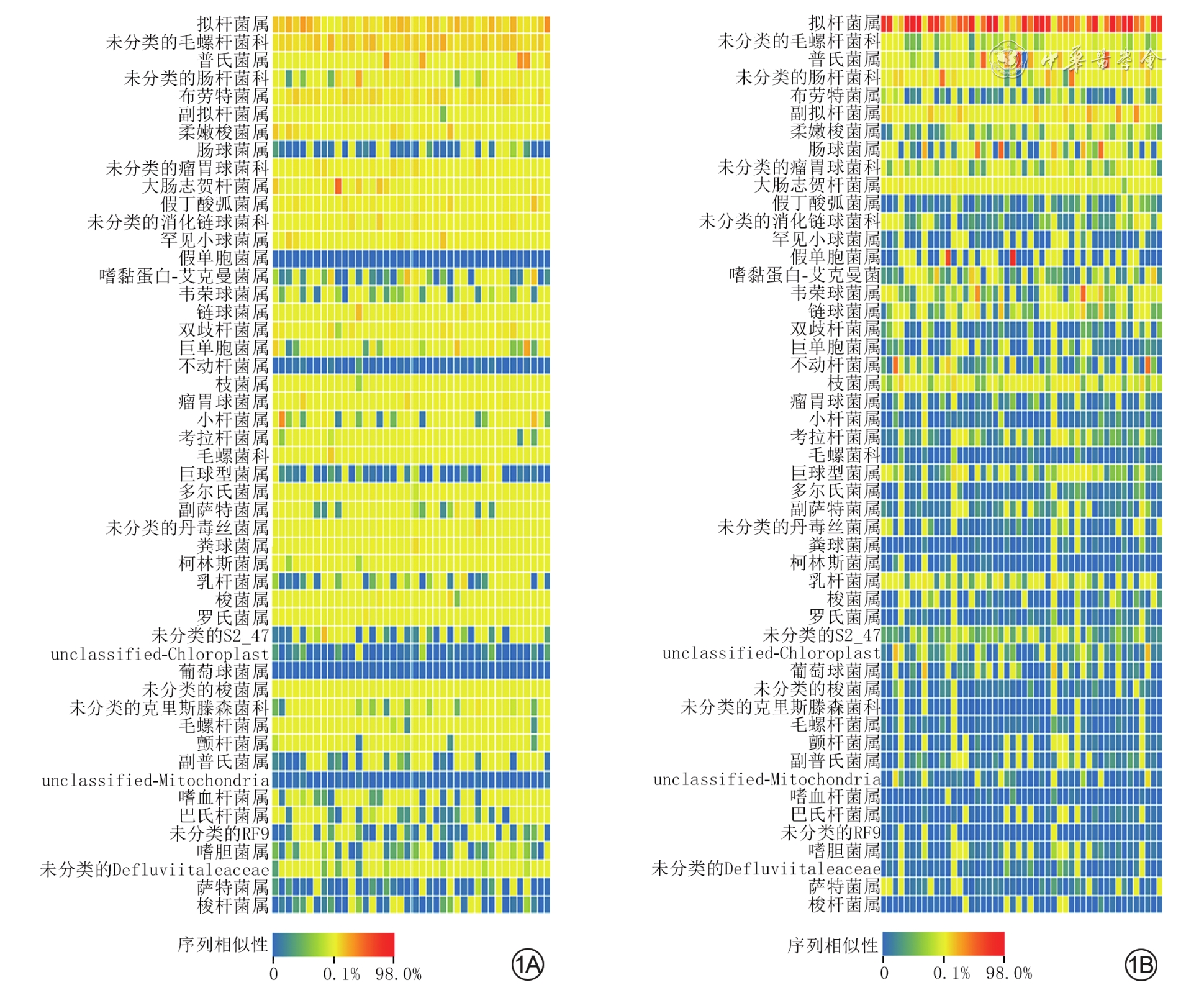
1 健康组40名健康志愿者和烧伤组48例严重烧伤患者伤后早期粪便菌群结构热力图。1A.健康组;1B.烧伤组
注:1A、1B中每行从左到右的40、48个色块代表40名健康志愿者和48例烧伤患者的样本

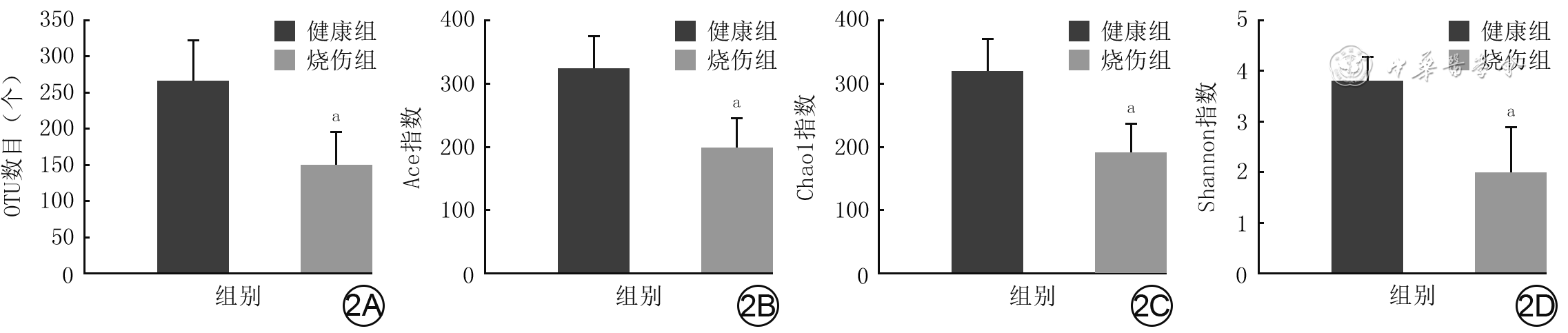
2 健康组40名健康志愿者和烧伤组48例严重烧伤患者伤后早期粪便菌群操作分类单元(OTU)数目及α多样性指数比较(
注:与健康组相比,aP<0.01

3 健康组40名健康志愿者和烧伤组48例严重烧伤患者伤后早期粪便菌群主成分分析图
注:每个色块代表一个样本,每个色块分别垂直于横、纵坐标上的距离代表样本受主成分1和主成分2影响的程度,样本间越聚集,说明相识程度越高
表1 健康组健康志愿者和烧伤组严重烧伤患者伤后早期粪便菌群科或属水平相对丰度比较[%,M(P25,P75)]
组别 人数/例数 拟杆菌属 未分类的毛螺杆菌科 普氏菌属 未分类的肠杆菌科 副拟杆菌属 盲杆菌属 肠球菌属 未分类的瘤胃球菌科 大肠志贺杆菌属 健康组 40 12.65(6.88,20.56) 11.38(8.10,18.79) 1.38(0.22,2.23) 0.36(0.12,1.68) 0.69(0.22,1.48) 3.89(2.33,10.24) 0.01(0,0.04) 3.52(1.91,5.37) 0.87(0.31,2.98) 烧伤组 48 51.82(24.89,81.99) 0.06(0.04,1.25) 0.16(0.08,0.68) 1.51(0.16,3.97) 1.78(0.16,7.50) 0.04(0.02,0.25) 0.06(0.01,0.13) 0.05(0.03,0.68) 0.32(0.09,1.00) Z值 -5.20 -8.03 -3.21 -1.47 -1.69 -7.63 -2.37 -5.88 -3.37 P值 <0.001 <0.001 0.002 0.152 0.103 <0.001 0.022 <0.001 0.001 注:罕见小球菌属、嗜黏蛋白-艾克曼菌属、萨特菌属等23种菌群相对丰度太小,未列出  下载: 导出CSV
下载: 导出CSV
表2 健康组健康志愿者和烧伤组严重烧伤患者伤后早期粪便菌群代谢水平比较[%,M(P25,P75)]
组别 人数/例数 氨基酸代谢 丙氨酸-天冬氨酸-谷氨酸代谢 精氨酸-脯氨酸代谢 半胱氨酸-蛋氨酸代谢 甘氨酸-丝氨酸-苏氨酸代谢 苯丙氨酸代谢 色氨酸代谢 酪氨酸代谢 健康组 40 2.14(1.59,2.75) 2.53(1.97,3.22) 1.85(1.50,2.41) 1.59(1.30,2.00) 0.34(0.28,0.44) 0.25(0.17,0.31) 0.63(0.52,0.83) 烧伤组 48 1.22(1.09,1.31) 1.29(1.08,1.50) 0.91(0.81,0.99) 0.84(0.72,0.93) 0.22(0.19,0.26) 0.10(0.09,0.17) 0.35(0.31,0.42) Z值 -4.75 -4.54 -4.75 -4.62 -3.71 -3.28 -4.19 P值 <0.001 <0.001 <0.001 <0.001 <0.001 0.001 <0.001
下载: 导出CSV
-

 下载:
下载:


图(3) / 表(2)
计量
- 文章访问数: 3361
- HTML全文浏览量: 130
- PDF下载量: 48
- 被引次数: 0
