



Early predictive value of high density lipoprotein cholesterol for secondary acute kidney injury in sepsis patients
-
摘要:
目的 探讨脓毒症患者高密度脂蛋白胆固醇(HDL-C)水平的变化及其对该类患者继发急性肾损伤(AKI)的早期预测价值。 方法 采用回顾性病例系列研究方法。2019年6月—2021年6月,河北医科大学第二医院收治232例符合入选标准的脓毒症患者,其中男126例、女106例,年龄24~71岁。依据是否继发AKI,将患者分为非AKI组(158例)和AKI组(74例)。对比2组患者入院时性别、年龄、身体质量指数(BMI)、体温、心率、原发感染部位、合并基础疾病情况、急性生理学和慢性健康状况评价Ⅱ(APACHE Ⅱ)评分及脓毒症相关性器官功能衰竭评价(SOFA)评分,确诊脓毒症时检测的血清C反应蛋白(CRP)、降钙素原、肌酐、胱抑素C及HDL-C水平,对数据进行独立样本t检验、χ2检验。对2组比较差异有统计学意义的指标进行多因素logistic回归分析,筛选影响232例脓毒症患者继发AKI的独立危险因素,并以独立危险因素为基础构建联合预测模型。绘制独立危险因素与联合预测模型预测232例脓毒症患者继发AKI的受试者操作特征(ROC)曲线,计算曲线下面积(AUC)及最佳阈值与最佳阈值下的敏感度、特异度。采用Delong检验对前述AUC的质量进行比较,采用χ2检验对最佳阈值下的敏感度和特异度进行比较。 结果 2组患者性别、年龄、BMI、体温、心率、原发感染部位、合并基础疾病以及CRP水平均相近(P>0.05);AKI组患者降钙素原、肌酐、胱抑素C、APACHE Ⅱ评分及SOFA评分均明显高于非AKI组(t值分别为-3.21、-16.14、-12.75、-11.13、-12.88, P<0.01),HDL-C水平显著低于非AKI组(t=6.33,P<0.01)。多因素logistic回归分析显示,肌酐、胱抑素C、HDL-C是232例脓毒症患者继发AKI的独立危险因素(比值比分别为2.45、1.68、2.12,95%置信区间分别为1.38~15.35、1.06~3.86、0.86~2.56,P<0.01)。肌酐、胱抑素C、HDL-C、联合预测模型预测232例脓毒症患者继发AKI的ROC的AUC分别为0.69、0.79、0.89、0.93(95%置信区间分别为0.61~0.76、0.72~0.85、0.84~0.92、0.89~0.96,P值均<0.01),最佳阈值分别为389.53 μmol/L、1.56 mg/L、0.63 mmol/L、0.48,最佳阈值下的敏感度分别为76.6%、81.4%、89.7%、95.5%,最佳阈值下的特异度分别为78.6%、86.7%、88.6%、96.6%。胱抑素C的AUC质量明显优于肌酐(z=2.34,P<0.05),HDL-C的AUC质量及最佳阈值下的敏感度、特异度均明显优于胱抑素C(z=3.33,χ2值分别为6.43、7.87,P<0.01)与肌酐(z=5.34,χ2值分别为6.32、6.41,P<0.01),联合预测模型的AUC质量及最佳阈值下的敏感度、特异度均明显优于肌酐、胱抑素C、HDL-C(z值分别6.18、4.50、2.06,χ2值分别5.31、7.23、3.99,6.56、7.34、4.00,P<0.05或P<0.01)。 结论 脓毒症继发AKI患者HDL-C水平较未继发AKI患者明显降低,该指标是脓毒症患者继发AKI的独立危险因素,其诊断价值优于肌酐和胱抑素C,前述3个指标联合对脓毒症患者继发AKI的预测价值更高。 Abstract:Objective To investigate the changes of high density lipoprotein cholesterol (HDL-C) in sepsis patients and its early predictive value for secondary acute kidney injury (AKI) in such patients. Methods A retrospective case series study was conducted. From June 2019 to June 2021, 232 sepsis patients who met the inclusion criteria were admitted to the Second Hospital of Hebei Medical University, including 126 males and 106 females, aged 24 to 71 years. According to whether complicating secondary AKI, the patients were divided into non-AKI group (n=158) and AKI group (n=74). Data of patients between the two groups were compared and statistically analyzed with independent sample t test or chi-square test, including the sex, age, body mass index (BMI), body temperature, heart rate, primary infection site, combined underlying diseases, acute physiology and chronic health evaluation Ⅱ (APACHE Ⅱ) score and sepsis-related organ failure assessment (SOFA) score at admission, and the serum levels of C-reactive protein (CRP), procalcitonin, creatinine, cystatin C, and HDL-C measured at diagnosis of sepsis. The multivariate logistic regression analysis was performed on the indicators with statistically significant differences between the two groups to screen the independent risk factors for developing secondary AKI in 232 sepsis patients, and the joint prediction model was established based on the independent risk factors. The receiver operating characteristic (ROC) curve of the independent risk factors and the joint prediction model predicting secondary AKI in 232 sepsis patients were drawn, and the area under the curve (AUC), the optimal threshold, and the sensitivity and specificity under the optimal threshold were calculated. The quality of the above-mentioned AUC was compared by Delong test, and the sensitivity and specificity under the optimal threshold were compared using chi-square test. Results The sex, age, BMI, body temperature, heart rate, primary infection site, combined underlying diseases, and CRP level of patients between the two groups were similar (P>0.05). The procalcitonin, creatinine, cystatin C, and scores of APACHE Ⅱ and SOFA of patients in AKI group were all significantly higher than those in non-AKI group (with t values of -3.21, -16.14, -12.75, -11.13, and -12.88 respectively, P<0.01), while the HDL-C level of patients in AKI group was significantly lower than that in non-AKI group (t=6.33, P<0.01). Multivariate logistic regression analysis showed that creatinine, cystatin C, and HDL-C were the independent risk factors for secondary AKI in 232 sepsis patients (with odds ratios of 2.45, 1.68, and 2.12, respectively, 95% confidence intervals of 1.38-15.35, 1.06-3.86, and 0.86-2.56, respectively, P<0.01). The AUCs of ROC curves of creatinine, cystatin C, HDL-C, and the joint prediction model for predicting secondary AKI in 232 sepsis patients were 0.69, 0.79, 0.89, and 0.93, respectively (with 95% confidence intervals of 0.61-0.76, 0.72-0.85, 0.84-0.92, and 0.89-0.96, respectively, P values all below 0.01); the optimal threshold were 389.53 μmol/L, 1.56 mg/L, 0.63 mmol/L, and 0.48, respectively; the sensitivity under the optimal threshold were 76.6%, 81.4%, 89.7%, and 95.5%, respectively; the specificity under the optimal threshold values were 78.6%, 86.7%, 88.6%, and 96.6%, respectively. The AUC quality of cystatin C was significantly better than that of creatinine (z=2.34, P<0.05), the AUC quality and sensitivity and specificity under the optimal threshold of HDL-C were all significantly better than those of cystatin C (z=3.33, with χ2 values of 6.43 and 7.87, respectively, P<0.01) and creatinine (z=5.34, with χ2 values of 6.32 and 6.41, respectively, P<0.01); the AUC quality and sensitivity and specificity under the optimal threshold of the joint prediction model were all significantly better than those of creatinine, cystatin C, and HDL-C (with z values of 6.18, 4.50, and 2.06, respectively, χ2 values of 5.31, 7.23, 3.99, 6.56, 7.34, and 4.00, respectively, P<0.05 or P<0.01). Conclusions HDL-C level in sepsis patients with secondary AKI is significantly lower than that in patients without secondary AKI. This is an independent risk factor for secondary AKI in sepsis patients with a diagnostic value being superior to that of creatinine and cystatin C. The combination of the aforementioned three indicators would have higher predicative valuable for secondary AKI in sepsis patients. -
Key words:
- Sepsis /
- Prognosis /
- Acute kidney injury /
- Forecasting /
- High density lipoprotein cholesterol /
- Creatinine /
- Cystatin C
-
创面修复是整形外科常见的临床问题,换药是最常用的促进创面愈合的方法,选择合适的敷料对创面愈合至关重要。随着材料学的发展,目前已有多种敷料被应用于临床,主要分为5类,包括多聚膜敷料、藻酸盐敷料、壳聚糖敷料、泡沫敷料和水胶体敷料。壳聚糖作为一种天然生物多糖,具有良好的生物相容性和可降解性,已被广泛应用于制备新型敷料[1, 2, 3]。壳聚糖能够抗感染、消炎、止血、减少创面渗出,从而促进组织再生和创面愈合[4, 5]。壳聚糖有多种类型,其中温敏性壳聚糖通过化学修饰引入亲水性羟丁基,可由低温液态转变为体温条件下的凝胶态,便于在创面表面形成保护膜,且适合携带可促进组织再生的生物活性物质[6, 7, 8, 9]。目前,温敏性羟丁基壳聚糖水凝胶在止血、抗感染及药物传递方面的应用已有相关报道[6,9],但在促进创面愈合中应用的研究较少。本研究旨在探讨温敏性羟丁基壳聚糖水凝胶在大鼠全层皮肤缺损创面愈合中的作用和潜在机制,从而为其临床应用提供依据。
1. 材料与方法
本研究经解放军总医院实验动物福利伦理委员会审批通过,批号:2017-X13-12,并遵循国家有关实验动物管理和使用的相关规定。
1.1 动物及主要试剂来源
健康清洁级7~10周龄SD大鼠51只,雌雄不限,体重250~300 g,购自解放军总医院实验动物中心,许可证号:SYXK(军)2017-0017。HE和Masson染色试剂盒购自北京中杉金桥生物技术有限公司,温敏性羟丁基壳聚糖水凝胶和羧甲基壳聚糖凝胶购自惠众国际医疗器械(北京)有限公司,戊巴比妥钠购自上海科丰化学试剂有限公司,TGF-β1、IL-6、基质金属蛋白酶1(MMP-1)ELISA检测试剂盒购自泰科兰博(北京)生物技术有限公司,DSX500型光学数码显微镜购自日本Olympus公司。
1.2 动物分组与处理
取51只大鼠,室温下单鼠单笼饲养,术前禁食24 h、禁水12 h,麻醉前称重。每只大鼠腹腔注射20 g/L戊巴比妥钠(30 mg/kg)麻醉后,背部脱毛,碘伏消毒皮肤后,在大鼠背部距脊柱两侧约1.0 cm处,制造2个直径2 cm的圆形创面,切开皮肤全层至背脊肌筋膜,创面皮缘用无菌橡胶圈缝线固定,伤后3 d换药时拆除。将大鼠按随机数字表法分为温敏性水凝胶组、凝胶组和空白对照组,每组17只大鼠(34个创面)。温敏性水凝胶组和凝胶组大鼠创面伤后即刻分别涂抹0.3 mL温敏性羟丁基壳聚糖水凝胶和羧甲基壳聚糖凝胶,温敏性水凝胶在体温作用下约10 s变成固态凝胶;空白对照组大鼠创面不进行其他处理。所有创面均贴凡士林油纱,用无菌纱布覆盖,并用弹力绷带包扎,每日换药。
1.3 水凝胶/凝胶状态和凡士林油纱去除情况
每天换药时观察温敏性水凝胶组大鼠创面温敏性羟丁基壳聚糖水凝胶及凝胶组大鼠创面羧甲基壳聚糖凝胶状态,记录去除凡士林油纱的难易程度。
1.4 创面大体观察及创面愈合率
伤后3、7、10、14、21 d,观察3组大鼠所有创面愈合情况,包括是否有感染、渗血渗液、肉芽组织的生长、异味、结痂等并拍照记录,使用AutoCAD2010 图像分析软件(美国Auto desk公司)测量未愈合创面面积并计算创面愈合率。创面愈合率=(原始创面面积-未愈合创面面积)÷原始创面面积×100%。
1.5 创面标本采集
伤后3、7、10、14、21 d,行大体观察和创面测量之后,每组各取2只大鼠,断颈处死后取适量创缘皮肤及创面组织,部分组织固定于体积分数10%甲醛中;其余组织放入冻存管中并做好标记,立即放置于-80 ℃液氮中。
1.6 病理学观察及胶原容积分数检测
取甲醛中固定的3组大鼠伤后各时间点创缘皮肤及创面组织,石蜡包埋后切片(厚5 μm),并分成两部分。一部分行HE染色,100倍光学数码显微镜下观察炎症细胞浸润、血管新生、再上皮化等情况;另一部分行Masson染色,100倍光学数码显微镜下观察胶原纤维再生和重塑情况,并采用Image J 1.52a图像分析软件(美国国立卫生研究院)定量分析胶原容积分数,即被染为蓝色的阳性胶原面积与组织总面积的百分比。
1.7 细胞因子检测
取液氮中冻存的3组大鼠伤后各时间点创缘皮肤及创面组织,进行常规裂解、匀浆,在4 ℃下,以10 000×g离心20 min去除碎片和不溶性物质,获得上清液,采用ELISA法检测IL-6、TGF-β1、MMP-1的表达。
1.8 统计学处理
采用Stata 16.0统计软件进行数据分析。计量资料数据均符合正态分布,以
2. 结果
2.1 水凝胶/凝胶状态和凡士林油纱去除情况
伤后换药时,凝胶组大鼠创面羧甲基壳聚糖凝胶呈液态凝胶状,可随体位流动(图1A);而温敏性水凝胶组大鼠创面温敏性羟丁基壳聚糖水凝胶紧密贴附于创面,不随体位变化而流动,且较羧甲基壳聚糖凝胶分布更均匀(图1B)。伤后换药时,温敏性水凝胶组大鼠创面凡士林油纱较易去除,而其他2组大鼠创面凡士林油纱不易去除。
 1 2组全层皮肤缺损大鼠伤后3 d换药时创面羧甲基壳聚糖凝胶或温敏性羟丁基壳聚糖水凝胶状态。1A.凝胶组羧甲基壳聚糖凝胶呈液态凝胶状;1B.温敏性水凝胶组温敏性羟丁基壳聚糖水凝胶呈固态凝胶状
1 2组全层皮肤缺损大鼠伤后3 d换药时创面羧甲基壳聚糖凝胶或温敏性羟丁基壳聚糖水凝胶状态。1A.凝胶组羧甲基壳聚糖凝胶呈液态凝胶状;1B.温敏性水凝胶组温敏性羟丁基壳聚糖水凝胶呈固态凝胶状2.2 创面愈合情况观察
伤后各时间点,温敏性水凝胶组和凝胶组大鼠创面渗血较空白对照组减少,温敏性水凝胶组和凝胶组大鼠创面均未结痂,肉芽组织生长好,无分泌物及异味;空白对照组大鼠创面可见结痂,有分泌物及异味。温敏性水凝胶组及凝胶组大鼠创面伤后各时间点未见明显感染现象;空白对照组大鼠伤后3、5 d各有1只大鼠因感染而死亡,余未见感染。
随着伤后时间的延长,3组大鼠创面面积均不断缩小。伤后7、10 d,温敏性水凝胶组和凝胶组大鼠创面面积明显小于空白对照组。伤后14 d,温敏性水凝胶组大鼠创面基本愈合,凝胶组及空白对照组大鼠仍可见残余创面。伤后21 d,温敏性水凝胶组和凝胶组大鼠创面均完全愈合,可见线性瘢痕且凝胶组大鼠创面瘢痕较宽;空白对照组大鼠仍可见残余创面。见图2。
 2 3组全层皮肤缺损大鼠伤后各时间点创面愈合情况。2A、2B、2C.分别为温敏性水凝胶组伤后0(即刻)、10、21 d创面情况,图2C创面完全愈合;2D、2E、2F.分别为凝胶组伤后0、10、21 d创面情况,图2E创面面积明显大于图2B,图2F创面基本愈合;2G、2H、2I.分别为空白对照组伤后0、10、21 d创面情况,图2H创面面积明显大于图2B,图2I仍可见残余创面注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶
2 3组全层皮肤缺损大鼠伤后各时间点创面愈合情况。2A、2B、2C.分别为温敏性水凝胶组伤后0(即刻)、10、21 d创面情况,图2C创面完全愈合;2D、2E、2F.分别为凝胶组伤后0、10、21 d创面情况,图2E创面面积明显大于图2B,图2F创面基本愈合;2G、2H、2I.分别为空白对照组伤后0、10、21 d创面情况,图2H创面面积明显大于图2B,图2I仍可见残余创面注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶2.3 创面愈合率
伤后3 d,3组大鼠创面愈合率相近(P>0.05);伤后7、10、14、21 d,温敏性水凝胶组和凝胶组大鼠创面愈合率明显高于空白对照组(P<0.01);伤后10 d,温敏性水凝胶组大鼠创面愈合率明显高于凝胶组(P<0.05)。见表1。
表1 3组全层皮肤缺损大鼠伤后各时间点创面愈合率比较(%,组别 3 d 7 d 10 d 14 d 21 d 温敏性水凝胶组 13.95±3.12 61.99±9.15 84.70±3.84 95.80±2.04 99.97±0.10 凝胶组 13.32±1.04 59.82±11.10 82.33±5.87c 93.02±3.72 99.24±1.30 空白对照组 13.06±0.85 38.13±16.40ab 48.16± 2.79ab 81.25± 6.75ab 97.51± 1.36ab F值 0.87 8.38 10.78 9.56 11.95 P值 0.05 0.02 <0.01 <0.01 <0.01 注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶;伤后3、7、10、14、21 d,温敏性水凝胶组和凝胶组创面数分别为34、30、26、22、18个,空白对照组(伤后3、5 d各有1只大鼠死亡)创面数分别为32、26、22、18、14个;与温敏性水凝胶组比较,aP<0.01,cP<0.05;与凝胶组比较,bP<0.01 2.4 HE和Masson染色结果
HE染色显示,3组大鼠创面伤后3 d均有大量中性粒细胞和淋巴细胞浸润。伤后7 d,3组大鼠创面炎症细胞浸润均较伤后3 d减少,同时可见毛细血管增生,创伤边缘上皮开始移行修复。伤后10 d,温敏性水凝胶组和凝胶组大鼠创面炎症细胞进一步减少,毛细血管增生明显,创面可见连续的上皮覆盖,而空白对照组大鼠创面较伤后7 d变化不明显。伤后14 d,温敏性水凝胶组和凝胶组大鼠创面炎症细胞浸润消失,且可见复层鳞状上皮结构已完整覆盖创面;空白对照组大鼠创面仍可见少量炎症细胞浸润。伤后21 d,温敏性水凝胶组和凝胶组大鼠创面完全愈合,可见表皮层和真皮层,未见毛囊等皮肤附件;空白对照组大鼠创面未完全愈合。见图3。
 3 3组全层皮肤缺损大鼠伤后3、7、14 d创面炎症细胞浸润、血管新生和再上皮化情况 苏木精-伊红×100。3A、3B、3C.分别为温敏性水凝胶组、凝胶组及空白对照组伤后3 d,创面均有大量中性粒细胞和淋巴细胞浸润;3D、3E、3F.分别为温敏性水凝胶组、凝胶组及空白对照组伤后7 d,炎症细胞分别较图3A、3B、3C减少,且图3D、3E炎症细胞均较图3F明显减少,3组同时可见毛细血管增生,创面边缘上皮开始移行修复;3G、3H、3I.分别为温敏性水凝胶组、凝胶组及空白对照组伤后14 d,图3G和3H创面炎症细胞浸润消失,并可见复层鳞状上皮结构已完整覆盖创面,图3I仍可见少量炎症细胞浸润且复层鳞状上皮结构不完整注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶
3 3组全层皮肤缺损大鼠伤后3、7、14 d创面炎症细胞浸润、血管新生和再上皮化情况 苏木精-伊红×100。3A、3B、3C.分别为温敏性水凝胶组、凝胶组及空白对照组伤后3 d,创面均有大量中性粒细胞和淋巴细胞浸润;3D、3E、3F.分别为温敏性水凝胶组、凝胶组及空白对照组伤后7 d,炎症细胞分别较图3A、3B、3C减少,且图3D、3E炎症细胞均较图3F明显减少,3组同时可见毛细血管增生,创面边缘上皮开始移行修复;3G、3H、3I.分别为温敏性水凝胶组、凝胶组及空白对照组伤后14 d,图3G和3H创面炎症细胞浸润消失,并可见复层鳞状上皮结构已完整覆盖创面,图3I仍可见少量炎症细胞浸润且复层鳞状上皮结构不完整注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶Masson染色显示,伤后3 d 时3组大鼠创面可见新生胶原纤维组织,伤后7、10 d时3组大鼠创面新生胶原纤维组织较伤后3 d增多。与空白对照组比较,温敏性水凝胶组和凝胶组大鼠创面伤后14、21 d胶原纤维更加致密,排列整齐有序。见图4。伤后10、14、21 d,温敏性水凝胶组和凝胶组大鼠创面胶原容积分数显著高于空白对照组(P<0.01);伤后14 d,温敏性水凝胶组大鼠创面胶原容积分数显著高于凝胶组(P<0.01),见图5。
 4 3组全层皮肤缺损大鼠伤后3、14、21 d创面胶原纤维变化 Masson×100。4A、4B、4C.分别为温敏性水凝胶组、凝胶组及空白对照组伤后3 d,创面新生胶原纤维组织较少;4D、4E、4F.分别为温敏性水凝胶组、凝胶组及空白对照组伤后14 d,图4D、4E胶原纤维组织较图4F多且排列更整齐;4G、4H、4I.分别为温敏性水凝胶组、凝胶组及空白对照组伤后21 d,图4G、4H较图4I胶原纤维更加致密,且排列整齐有序注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶
4 3组全层皮肤缺损大鼠伤后3、14、21 d创面胶原纤维变化 Masson×100。4A、4B、4C.分别为温敏性水凝胶组、凝胶组及空白对照组伤后3 d,创面新生胶原纤维组织较少;4D、4E、4F.分别为温敏性水凝胶组、凝胶组及空白对照组伤后14 d,图4D、4E胶原纤维组织较图4F多且排列更整齐;4G、4H、4I.分别为温敏性水凝胶组、凝胶组及空白对照组伤后21 d,图4G、4H较图4I胶原纤维更加致密,且排列整齐有序注:温敏性水凝胶组、凝胶组大鼠创面分别涂抹温敏性羟丁基壳聚糖水溶胶、羧甲基壳聚糖凝胶 5 3组全层皮肤缺损大鼠伤后各时间点创面胶原容积分数比较(
5 3组全层皮肤缺损大鼠伤后各时间点创面胶原容积分数比较(2.5 细胞因子表达
伤后3、7、10 d,温敏性水凝胶组大鼠创面IL-6的表达显著高于凝胶组和空白对照组(P<0.01),凝胶组大鼠创面IL-6的表达显著低于空白对照组(P<0.01),见图6。伤后3、7、10 d,温敏性水凝胶组大鼠创面TGF-β1的表达显著高于凝胶组及空白对照组(P<0.01);伤后3、7 d,凝胶组大鼠创面TGF-β1的表达显著低于空白对照组(P<0.01);伤后10 d,凝胶组大鼠创面TGF-β1的表达显著高于空白对照组(P<0.01);伤后14 d,凝胶组大鼠创面TGF-β1的表达明显高于温敏性水凝胶组和空白对照组(P<0.01);伤后21 d,温敏性水凝胶组大鼠创面TGF-β1的表达显著低于凝胶组大鼠和空白对照组(P<0.01),凝胶组大鼠创面TGF-β1的表达显著低于空白对照组(P<0.01),见图7。伤后7 d,凝胶组大鼠创面MMP-1的表达显著高于温敏性水凝胶组和空白对照组(P<0.01);伤后10、14、21 d,温敏性水凝胶组大鼠创面MMP-1的表达显著高于凝胶组及空白对照组(P<0.01);伤后10 d,凝胶组大鼠创面MMP-1的表达显著低于空白对照组(P<0.01);伤后14、21 d,凝胶组大鼠创面MMP-1的表达显著高于空白对照组(P<0.01),见图8。
 6 3组全层皮肤缺损大鼠伤后各时间点创面白细胞介素6的表达比较(
6 3组全层皮肤缺损大鼠伤后各时间点创面白细胞介素6的表达比较( 7 3组全层皮肤缺损大鼠伤后各时间点创面转化生长因子β1的表达比较(
7 3组全层皮肤缺损大鼠伤后各时间点创面转化生长因子β1的表达比较( 8 3组全层皮肤缺损大鼠伤后各时间点创面基质金属蛋白酶1的表达(
8 3组全层皮肤缺损大鼠伤后各时间点创面基质金属蛋白酶1的表达(3. 讨论
创面愈合是一个复杂有序的生物学过程,大致分为4个阶段,包括止血、炎症反应、增生、组织重塑阶段,各阶段相互交叉、重叠。当新鲜的肉芽形成时,表皮细胞从创面边缘向创面中心迁移、增殖和分化,创面的愈合需要一个湿润环境[10],合适的敷料有助于加速创面愈合。
既往研究证实,壳聚糖具有抗感染作用,本研究中温敏性水凝胶组及凝胶组大鼠创面无感染现象,具有良好的愈合表现。温敏性羟丁基壳聚糖水凝胶和羧甲基壳聚糖凝胶具备壳聚糖的止血、抗感染及促愈合等优势,且凝胶能使创面床保持湿润,提供一个非黏附的环境,且凝胶的吸水性有助于吸收创面渗出物;而空白对照组创面环境干燥,易形成痂皮,不能保持湿润环境,不利于创面的愈合。另外,由于羟丁基壳聚糖水凝胶具有独特的温敏特性,低温环境(2~4 ℃)下为可流动的黏性液体,方便涂抹于创面;而当接触创面组织后,由于温度升高,转变为不流动的固体凝胶状,紧密贴附于创面,不随体位变化而流动,不容易流失及被外层敷料吸走。羧甲基壳聚糖凝胶由于其流动性,导致发挥作用的壳聚糖凝胶变少,影响其效果。换药时观察到,温敏性水凝胶组大鼠创面凡士林油纱较另外2组更易去除,可减少换药过程中对上皮组织的破坏而影响创面愈合。
本研究结果表明,温敏性水凝胶组和凝胶组大鼠创面渗血较空白对照组少,说明2种壳聚糖凝胶具有止血作用。随着伤后时间的延长,温敏性水凝胶组大鼠创面面积明显小于凝胶组和空白对照组,且温敏性水凝胶组和凝胶组大鼠伤后7~21 d创面愈合率明显高于空白对照组,说明2种壳聚糖凝胶均可促进创面愈合,且温敏性羟丁基壳聚糖水凝胶的效果可能更佳。组织学染色观察到,温敏性水凝胶组大鼠创面胶原纤维、毛细血管增生较凝胶组及空白对照组出现得更早。炎症细胞在伤后早期迅速增多,以发挥抗炎、抗感染、促进组织修复的作用;后期更早减少和消失。愈合环境炎症细胞的变化促使胶原纤维组织大量增生、重建,排列整齐有序,使创面得以填充并引起收缩,创面迅速愈合,并可见更完整的复层鳞状上皮结构覆盖创面。以上结果显示,温敏性羟丁基壳聚糖水凝胶和羧甲基壳聚糖凝胶通过调控炎症细胞,改善创面愈合的微环境,促进创面组织再生。胶原容积分数[11, 12]分析结果显示伤后10、14、21 d温敏性水凝胶组和凝胶组大鼠创面胶原容积分数明显高于空白对照组,说明在创面修复的全过程中,温敏性羟丁基壳聚糖水凝胶能够促进胶原蛋白大量合成,有助于创面更好、更快地愈合。
创面修复早期为炎症反应阶段,IL-6含量直接影响该阶段创面的上皮化和肉芽组织生成,在创伤修复过程中IL-6缺失或低水平表达都会妨碍创面的正常愈合,而IL-6过度表达常常会导致瘢痕形成[13, 14]。本研究结果显示,温敏性水凝胶组和凝胶组大鼠创面IL-6的表达在伤后早期迅速增多,伤后14、21 d,2组大鼠创面IL-6水平已经降到正常水平,这与创面修复早期为炎症反应阶段,然后进入组织修复阶段,炎症因子恢复至正常水平相符。
TGF-β1主要由白细胞、巨噬细胞、Fb和KC产生,发生创伤后,血小板立即释放大量TGF-β1[15, 16, 17],并趋化中性粒细胞、巨噬细胞和Fb向创面迁移,这些迁移的细胞又进一步提高了TGF-β1的水平[18]。肉芽组织中的TGF-β1可以促进血管再生、Fb增殖、肌Fb分化以及基质的沉淀。有研究表明,外源性TGF-β1可以缩短创面愈合时间,并提高愈合的机械强度,可见TGF-β1对创面的愈合至关重要[19]。有研究表明,在创面修复早期,TGF-β1能作用于创面中的Fb,介导Ⅰ、Ⅲ型胶原蛋白,整合素,弹性蛋白,纤维连接蛋白等多种ECM成分大量合成,并抑制ECM降解酶的产生,加强基质与细胞的结合,促进创面张力增加和创面局部纤维化,从而促进创面愈合[20, 21];但在创面修复后期,TGF-β1的过度表达可导致瘢痕形成[22, 23, 24]。本研究中温敏性水凝胶组大鼠创面TGF-β1的表达在创面修复的早期至中期(伤后3~10 d)呈现上升趋势;在修复后期,即伤后14~21 d呈现下降的趋势,在创面愈合后期呈现低表达状态,无明显促进瘢痕增生的表现。以上结果显示,温敏性水凝胶通过调控创面TGF-β1的表达,加速组织修复,提高创面愈合强度,缩短创面愈合时间并减少瘢痕形成。
MMP是ECM降解最主要的水解酶,MMP-1是第1个被定性的MMP,属于胶原酶,主要功能是分解胶原,调节ECM沉积[25, 26, 27]。胶原酶活性与创面重塑密切相关,胶原的合成和降解是影响创面愈合的重要因素[28],而其降解主要由胶原酶来调控。正常组织中胶原酶组织抑制物的含量均较低,创伤、组织重塑过程等刺激Fb分泌MMP-1,增加其在组织中的含量[29, 30, 31]。对创面处MMP-1的表达测定结果表明,在创面组织重塑阶段(伤后10~21 d),温敏性水凝胶组大鼠创面MMP-1的表达显著高于凝胶组及空白对照组,温敏性水凝胶组大鼠创面愈合后胶原排列整齐,与正常皮肤组织基本一致。以上结果显示,温敏性水凝胶通过调控创面处胶原酶MMP-1的高度表达,从而加速对创面处胶原的分解和调节,使创面愈合良好,并有助于减少瘢痕的形成[32]。
IL-6、TGF-β1、MMP-1等细胞因子的分泌量与创面愈合之间的关系复杂而微妙,处于一种细微的平衡,这些细胞因子过多或不足的都会影响创面愈合质量。本研究通过动物实验观察到,温敏性水凝胶可通过调节细胞因子(IL-6、TGF-β1和MMP-1)的表达,促进创面愈合。因此,本课题组推断温敏性羟丁基壳聚糖水凝胶可能通过某种机制,为创面提供一种信号,以调节细胞因子的分泌量,并为创面修复提供良好的愈合环境,促进创面修复,但这种复杂的促进创面修复的机制尚未明确,需要进一步深入研究。
综上所述,温敏性壳聚糖水凝胶在创面愈合的不同阶段,能够提高创面处IL-6、TGF-β1的含量,从而加速创面的愈合;并能够提高创面处MMP-1的含量,使新生胶原排列有序,从而提高创面愈合质量和强度。本研究结果表明温敏性羟丁基壳聚糖水凝胶促进创面愈合的效果显著优于传统敷料,且比同类产品羧甲基壳聚糖凝胶的效果更佳,可为温敏性羟丁基壳聚糖水凝胶的临床应用奠定基础。
·科技快讯·
高压氧联合血红蛋白喷雾剂治疗放射性溃疡的病例报告和文献综述
李京宴:论文撰写、数据整理、统计学分析;姚咏明、田英平: 研究指导、论文修改、经费支持所有作者均声明不存在利益冲突本刊编辑委员会 -
参考文献
(35) [1] LudwigKR,HummonAB.Mass spectrometry for the discovery of biomarkers of sepsis[J].Mol Biosyst,2017,13(4):648-664.DOI: 10.1039/c6mb00656f. [2] Belgian Outcome in Burn Injury Study Group. Development and validation of a model for prediction of mortality in patients with acute burn injury[J]. Br J Surg, 2009, 96(1):111-117. DOI: 10.1002/bjs.6329. [3] MouriT, KawaharaH, MatsumotoT, et al. Respiratory disorder at the end of surgery for peritonitis due to colorectal perforation is a critical predictor of postoperative sepsis[J]. In Vivo, 2019, 33(4):1329-1332. DOI: 10.21873/invivo.11607. [4] VincentJL,RelloJ,MarshallJ,et al.International study of the prevalence and outcomes of infection in intensive care units[J].JAMA,2009,302(21):2323-2329.DOI: 10.1001/jama.2009.1754. [5] RelloJ, Valenzuela-SánchezF, Ruiz-RodriguezM, et al. Sepsis: a review of advances in management[J].Adv Ther, 2017, 34(11):2393-2411. DOI: 10.1007/s12325-017-0622-8. [6] 夏照帆,伍国胜.浅谈细胞因子在脓毒症中的作用及临床应用现状[J].中华烧伤杂志,2019,35(1):3-7.DOI: 10.3760/cma.j.issn.1009-2587.2019.01.002. [7] 中国医疗保健国际交流促进会急诊医学分会,中华医学会急诊医学分会,中国医师协会急诊医师分会,等.中国“脓毒症早期预防与阻断”急诊专家共识[J].中华危重病急救医学,2020, 32(5):518-530.DOI: 10.3760/cma.j.cn121430-20200514-00414. [8] CzuraCJ."Merinoff symposium 2010: sepsis"-speaking with one voice[J].Mol Med,2011,17(1/2):2-3.DOI: 10.2119/molmed.2010.00001.commentary. [9] WuL,FengQ,AiML,et al.The dynamic change of serum S100B levels from day 1 to day 3 is more associated with sepsis- associated encephalopathy[J].Sci Rep,2020,10(1):7718.DOI: 10.1038/s41598-020-64200-3. [10] AngusDC,van der PollT.Severe sepsis and septic shock[J].N Engl J Med,2013,369(9):840-851.DOI: 10.1056/NEJMra1208623. [11] CoopersmithCM,WunschH,FinkMP,et al.A comparison of critical care research funding and the financial burden of critical illness in the United States[J].Crit Care Med,2012,40(4):1072-1079.DOI: 10.1097/CCM.0b013e31823c8d03. [12] WiersingaWJ,LeopoldSJ,CranendonkDR,et al.Host innate immune responses to sepsis[J].Virulence,2014,5(1):36-44.DOI: 10.4161/viru.25436. [13] SchulteW,BernhagenJ,BucalaR.Cytokines in sepsis: potent immunoregulators and potential therapeutic targets--an updated view[J].Mediators Inflamm,2013,2013:165974.DOI: 10.1155/2013/165974. [14] SmithLE.High-density lipoproteins and acute kidney injury[J].Semin Nephrol,2020,40(2):232-242.DOI: 10.1016/j.semnephrol.2020.01.013. [15] SingerM,DeutschmanCS,SeymourCW,et al.The third international consensus definitions for sepsis and septic shock (sepsis-3)[J].JAMA,2016,315(8):801-810.DOI: 10.1001/jama.2016.0287. [16] KhwajaA.KDIGO clinical practice guidelines for acute kidney injury[J].Nephron Clin Pract,2012,120(4):c179-184.DOI: 10.1159/000339789. [17] 黄祺,孙宇,罗莉,等.ICU创伤患者并发脓毒症预警评分系统的建立[J]. 中华危重病急救医学,2019,31(4):422-427. DOI: 10.3760/cma.j.issn.2095-4352.2019.04.010. [18] 杨建华,王旭,张安强,等.创伤脓毒症风险预警诊断和预后评估模型建立与评价[J].中华创伤杂志,2017,33(5):447-452.DOI: 10.3760/cma.j.issn.1001-8050.2017.05.013. [19] JainS. Sepsis: an update on current practices in diagnosis and management[J]. Am J Med Sci, 2018, 356(3): 277-286.DOI: 10.1016/j.amjms.2018.06.012. [20] FleischmannC, ScheragA, AdhikariNK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations[J]. Am J Respir Crit Care Med, 2016, 193(3): 259-272.DOI: 10.1164/rccm.201504-0781OC. [21] RhodesA, EvansLE, AlhazzaniW, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016[J]. Intensive Care Med, 2017,43(3): 304-377.DOI: 10.1007/s00134-017-4683-6. [22] TabetF,VickersKC,Cuesta TorresLF,et al.HDL-transferred microRNA-223 regulates ICAM-1 expression in endothelial cells[J].Nat Commun,2014,5:3292.DOI: 10.1038/ncomms4292. [23] van ZonneveldAJ,RabelinkTJ,BijkerkR.miRNA-coordinated networks as promising therapeutic targets for acute kidney injury[J].Am J Pathol,2017,187(1):20-24.DOI: 10.1016/j.ajpath.2016.10.017. [24] RenGL,ZhuJ,LiJ,et al.Noncoding RNAs in acute kidney injury[J].J Cell Physiol,2019,234(3):2266-2276.DOI: 10.1002/jcp.27203. [25] LevyMM,EvansLE,RhodesA.The surviving sepsis campaign bundle: 2018 update[J].Crit Care Med,2018,44(6):997-1000.DOI: 10.1097/CCM.0000000000003119. [26] Nunez LopezO,Cambiaso-DanielJ,BranskiLK,et al.Predicting and managing sepsis in burn patients: current perspectives[J].Ther Clin Risk Manag,2017,13:1107-1117.DOI: 10.1097/CCM.0000000000003119. [27] XieY,WangQ,WangC,et al.Association between the levels of urine kidney injury molecule-1 and the progression of acute kidney injury in the elderly[J].PLoS One,2017,12(2):e0171076.DOI: 10.1371/journal.pone.0171076. [28] SinghIM,ShishehborMH,AnsellBJ.High-density lipoprotein as a therapeutic target: a systematic review[J].JAMA,2007,298(7):786-798.DOI: 10.1001/jama.298.7.786. [29] Roveran GengaK,LoC,CirsteaM,et al.Two-year follow-up of patients with septic shock presenting with low HDL: the effect upon acute kidney injury, death and estimated glomerular filtration rate[J].J Intern Med,2017,281(5):518-529.DOI: 10.1111/joim.12601. [30] GuoL,AiJ,ZhengZ,et al.High density lipoprotein protects against polymicrobe-induced sepsis in mice[J].J Biol Chem,2013,288(25):17947-17953.DOI: 10.1074/jbc.M112.442699. [31] MurphyAJ,WoollardKJ,HoangA,et al.High-density lipoprotein reduces the human monocyte inflammatory response[J].Arterioscler Thromb Vasc Biol,2008,28(11):2071-2077.DOI: 10.1161/ATVBAHA.108.168690. [32] De NardoD,LabzinLI,KonoH,et al.High-density lipoprotein mediates anti-inflammatory reprogramming of macrophages via the transcriptional regulator ATF3[J].Nat Immunol,2014,15(2):152-160.DOI: 10.1038/ni.2784. [33] LeeDW,FaubelS,EdelsteinCL.Cytokines in acute kidney injury (AKI)[J].Clin Nephrol,2011,76(3):165-173.DOI: 10.5414/cn106921. [34] HuP,ChenY,PangJ,et al.Association between IL-6 polymorphisms and sepsis[J].Innate Immun,2019,25(8):465-472.DOI: 10.1177/1753425919872818. [35] RochwergB,OczkowskiSJ,SiemieniukR,et al.Corticosteroids in sepsis: an updated systematic review and meta-analysis[J].Crit Care Med,2018,46(9):1411-1420.DOI: 10.1097/CCM.0000000000003262. -
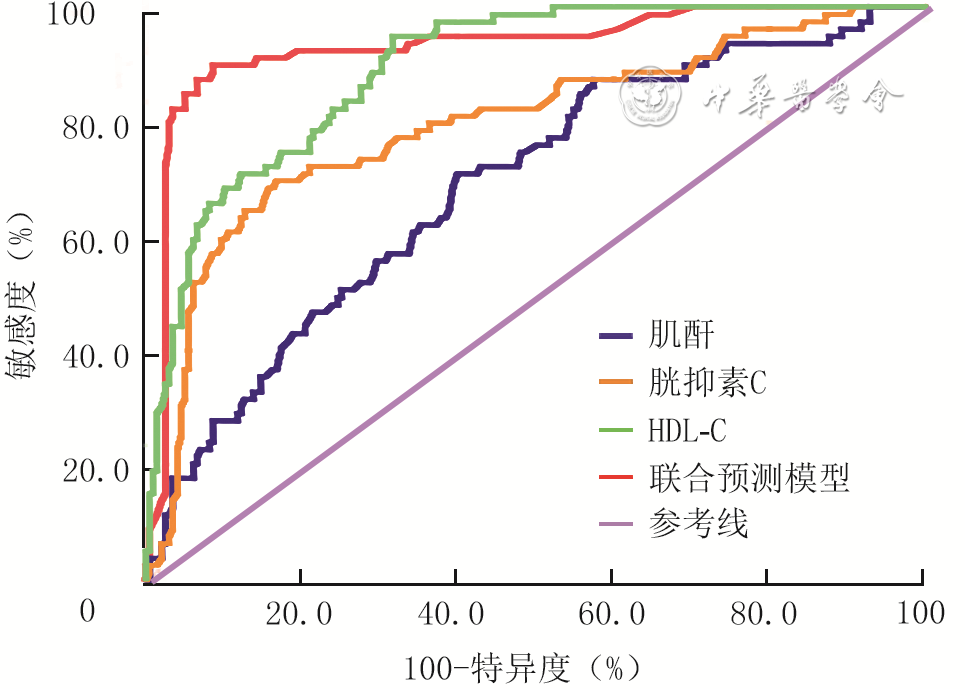
1 3种独立危险因素与联合预测模型预测232例脓毒症患者继发急性肾损伤的受试者操作特征曲线
注:HDL-C为高密度脂蛋白胆固醇;联合预测模型以肌酐、胱抑素C与HDL-C为基础
表1 2组脓毒症患者临床资料比较
组别 例数 性别(例) 年龄(岁, BMI(kg/m2, 体温(℃, 心率(次/min, 合并基础疾病(例) 高血压 冠心病 糖尿病 COPD 脑血管疾病 脑血管疾病 男 女 非AKI组 158 82 76 54±12 21.8±2.9 38.5±0.9 97±17 57 28 32 15 22 10 AKI组 74 44 30 55±9 22.5±3.6 38.8±0.8 101±18 22 13 21 10 13 8 统计量值 χ2=1.16 t=-0.71 t=-1.43 t=-1.60 t=-1.79 χ2=0.90 χ2=0.01 χ2=1.89 χ2=0.85 χ2=0.52 χ2=1.41 P值 0.323 0.477 0.153 0.109 0.073 0.375 0.977 0.182 0.370 0.555 0.292 注:AKI为急性肾损伤,BMI为身体质量指数,COPD为慢性阻塞性肺疾病,APACHE Ⅱ为急性生理学和慢性健康状况评价Ⅱ,SOFA为脓毒症相关性器官功能衰竭评价,CRP为C反应蛋白,HDL-C为高密度脂蛋白胆固醇  下载: 导出CSV
下载: 导出CSV
表2 232例脓毒症患者继发急性肾损伤的多因素logistic回归分析结果
因素 回归系数 标准误 比值比 95%置信区间 P值 降钙素原(ng/mL) 0.21 0.33 0.59 0.56~0.71 0.055 肌酐(μmol/L) 4.13 4.62 2.45 1.38~15.35 <0.001 胱抑素C(mg/L) 0.91 0.53 1.68 1.06~3.86 <0.001 HDL-C(mmol/L) 1.02 0.41 2.12 0.86~2.56 <0.001 APACHE Ⅱ评分(分) 0.07 0.02 0.96 0.91~1.53 0.083 SOFA评分(分) 0.28 0.15 1.31 0.78~1.72 0.112 注:HDL-C为高密度脂蛋白胆固醇,APACHE Ⅱ为急性生理学和慢性健康状况评价Ⅱ,SOFA为脓毒症相关性器官功能衰竭评价
下载: 导出CSV
表3 3种独立危险因素与联合预测模型对232例脓毒症患者继发AKI预测的受试者操作特征曲线的曲线下面积质量及最佳阈值下敏感度和特异度比较
对比因素或模型 曲线下面积 敏感度 特异度 曲线下面积差值 标准误 95%置信区间 z值 P值 χ2值 P值 χ2值 P值 肌酐与胱抑素C 0.10 0.05 0.02~0.20 2.34 0.019 3.43 0.213 3.22 0.108 肌酐与HDL-C 0.20 0.04 0.13~0.28 5.34 0.001 6.32 0.001 6.41 0.001 肌酐与联合预测模型 0.24 0.04 0.17~0.32 6.18 0.001 5.31 0.001 6.56 0.001 胱抑素C与HDL-C 0.10 0.03 0.04~0.16 3.33 0.001 6.43 0.001 7.87 0.001 胱抑素C与联合预测模型 0.14 0.03 0.08~0.20 4.50 0.001 7.23 0.001 7.34 0.001 HDL-C与联合预测模型 0.04 0.02 0.01~0.07 2.06 0.039 3.99 0.028 4.00 0.023 注:AKI为急性肾损伤,HDL-C为高密度脂蛋白胆固醇;联合预测模型以肌酐、胱抑素C与HDL-C为基础
下载: 导出CSV
脱细胞真皮基质(ADM) 重症监护病房(ICU) 动脉血氧分压(PaO2) 丙氨酸转氨酶(ALT) 白细胞介素(IL) 磷酸盐缓冲液(PBS) 急性呼吸窘迫综合征(ARDS) 角质形成细胞(KC) 反转录-聚合酶链反应(RT-PCR) 天冬氨酸转氨酶(AST) 半数致死烧伤面积(LA50) 全身炎症反应综合征(SIRS) 集落形成单位(CFU) 内毒素/脂多糖(LPS) 超氧化物歧化酶(SOD) 细胞外基质(ECM) 丝裂原活化蛋白激酶(MAPK) 动脉血氧饱和度(SaO2) 表皮生长因子(EGF) 最低抑菌浓度(MIC) 体表总面积(TBSA) 酶联免疫吸附测定(ELISA) 多器官功能障碍综合征(MODS) 转化生长因子(TGF) 成纤维细胞(Fb) 多器官功能衰竭(MOF) 辅助性T淋巴细胞(Th) 成纤维细胞生长因子(FGF) 一氧化氮合酶(NOS) 肿瘤坏死因子(TNF) 3-磷酸甘油醛脱氢酶(GAPDH) 负压伤口疗法(NPWT) 血管内皮生长因子(VEGF) 苏木精-伊红(HE) 动脉血二氧化碳分压(PaCO2) 负压封闭引流(VSD)
下载: 导出CSV
期刊类型引用(21)
1. 隋磊,谢强,孔宇,王晓雪,郝宇,李小东. 双层人工真皮联合负压封闭引流和自体刃厚皮片移植治疗慢性难愈合创面的疗效. 局解手术学杂志. 2025(02): 125-129 .  百度学术
百度学术2. 付全有,邢福席,李林,李勇,刘继松. 人工真皮联合自体瘢痕表皮移植修复大面积烧伤后期关节部位瘢痕畸形. 中国组织工程研究. 2024(10): 1533-1539 . 百度学术3. 李飞,何延奇,李东杰. 负压创面治疗技术的机制及在烧伤整形外科中的应用. 海南医学. 2024(01): 143-148 . 百度学术4. 蒋丹,刘亚兰,李胜,朱澳博. 不同人工真皮结合自体刃厚皮片移植修复骨质肌腱外露创面的疗效对比. 中国美容医学. 2024(04): 37-41 . 百度学术5. 彭祥,高玥,姜文华,李浩,章晓玲,张颖,何智灵,单记春,双峰,杨迪,万得恩. 人工真皮联合自体富血小板血浆凝胶修复骨/肌腱外露创面的早期临床疗效. 中华骨与关节外科杂志. 2024(06): 552-557 . 百度学术6. 刘江涛,陈蓝,王一勇,欧阳容兰,黄书润. 负压封闭引流联合含银液体敷料治疗糖尿病足的临床疗效研究. 感染、炎症、修复. 2024(02): 87-91+82 . 百度学术7. 刘江涛,曾纯,李丽香,王一勇,黄书润. 负压封闭引流联合腓动脉穿支皮瓣修复外踝部毁损伤创面的疗效. 吉林医学. 2024(08): 1802-1805 . 百度学术8. 孙浩博,贾志刚,虞俊杰. 3种不同创基准备程序性治疗方法在慢性难愈性创面中的效果观察. 中国现代医学杂志. 2023(05): 68-73 . 百度学术9. 刘江涛,王一勇,欧阳容兰,黄书润. 指背动脉穿支皮瓣修复手指深度创面的临床疗效. 安徽医学. 2023(06): 722-725 . 百度学术10. 陈永新,张元文,姚志慧,赵耀,唐文明,潘文东. 人工真皮与自体皮片复合移植联合负压封闭引流整复关节部位瘢痕的效果. 中华整形外科杂志. 2023(06): 590-595 . 百度学术11. 刘江涛,王一勇,林奕锋,黄书润. 掌背动脉穿支皮瓣修复手指深度创面的临床效果. 武警医学. 2023(08): 668-671+677 . 百度学术12. 刘海涛,韩志新,牛大伟,杜卫祺. 重组牛碱性成纤维细胞生长因子联合复合皮修复糖尿病患者功能部位皮肤软组织缺损的临床效果. 慢性病学杂志. 2023(12): 1780-1784 . 百度学术13. 杨焕纳,梁琰,韩大伟,刘磊,谢江帆,田社民,夏成德,魏莹. 人工真皮联合自体皮修复儿童手指电烧伤后骨骼和/或肌腱外露创面的效果. 中华烧伤与创面修复杂志. 2023(12): 1180-1184 .  本站查看
本站查看14. 冯颜杰,欧阳欢庆,涂智鑫,袁剑,吴伟强. 双层人工真皮在手部或足部骨质肌腱外露创面治疗中的应用效果分析. 世界复合医学. 2023(10): 54-56+60 . 百度学术15. 吴磊,周济宏,杨婷,蒋琪霞. 人工真皮替代物应用于伤口护理的研究进展. 护理学报. 2022(05): 42-46 . 百度学术16. 戚建武,陈邵,孙斌鸿,柴益铜,黄剑,李一,杨科跃,孙赫阳,陈宏. 游离背阔肌肌皮瓣联合人工真皮及刃厚皮治疗下肢脱套伤的临床效果. 中华烧伤与创面修复杂志. 2022(04): 347-353 . 本站查看17. 刘江涛,黄书润,欧阳容兰,王一勇. 小腿穿支皮瓣修复足踝部皮肤软组织缺损. 中国现代手术学杂志. 2022(02): 114-119 . 百度学术18. 曾皓,张烁,徐泽华,罗文跃,龙丽芸. 双层人工真皮在骨质肌腱外露创面中的应用. 临床医药实践. 2022(08): 583-585+618 . 百度学术19. 王春书,张鹏飞,王亮,薛士辉,杜康,汪剑龄,孙中洋. 人工真皮与游离植皮修复指腹皮肤软组织缺损的比较研究. 实用骨科杂志. 2022(09): 778-781+851 . 百度学术20. 刘江涛,欧阳容兰,李丽香,黄书润,李小毅. 膝降动脉穿支皮瓣应用于膝周软组织缺损创面修复的效果分析. 东南国防医药. 2022(05): 486-489 . 百度学术21. 由夫超,田文平,曹立鹤,高晗,马昌志,何雪峰. 人工真皮联合全厚皮移植在手指局部软组织缺损中的应用. 手术电子杂志. 2022(06): 26-31 . 百度学术其他类型引用(6)
-

 下载:
下载:
 百度学术
百度学术
计量
- 文章访问数: 1610
- HTML全文浏览量: 110
- PDF下载量: 30
- 被引次数: 27
