




Expert consensus on enteral nutrition treatment for burned children (2025 edition)
-
摘要: 烧伤会显著增加机体能量消耗,及时有效的营养支持对于烧伤治疗至关重要。儿童烧伤后的代谢反应与成人存在较大差异,在营养支持治疗方面也存在不同。中华医学会烧伤外科学分会小儿烧伤学组、中国女医师协会烧创伤专业委员会、北京人体损伤修复研究会儿童烧伤整形专业委员会组织专家通过文献查阅、问卷调查、证据筛选等环节,深入讨论后,在营养筛查、能量测算、营养时机和营养方式等方面达成了关于烧伤儿童肠内营养治疗的共识,以期为临床实践提供参考标准。Abstract: Burns lead to a substantial increase in energy expenditure of body, making timely and effective nutritional support essential for burn management. The metabolic responses to burns in children are significantly different from those in adults, necessitating distinct approaches for nutritional support and treatment. Through processes including literature review, questionnaire survey, and evidence screening, the experts from Pediatric Burn Study Group of Chinese Burn Association, Burn Trauma Professional Committee of Chinese Medical Women's Association, and Pediatric Burn and Plastic Surgery Professional Committee of Beijing Research Society for Human Body Injury Repair conducted in-depth discussions and reached a consensus on enteral nutrition treatment for burned children in terms of nutritional screening, energy calculation, nutritional timing, and nutritional modalities, hoping to provide reference standards for clinical practice.
-
Key words:
- Burns /
- Child /
- Nutritional treatment /
- Enteral nutrition /
- Expert consensus
-
参考文献
(62) [1] 中华医学会烧伤外科学分会, 中国医疗保健国际交流促进会烧伤医学分会. 成年严重烧伤患者肠内营养护理专家共识(2024版)[J]. 中华烧伤与创面修复杂志, 2024, 40(9): 801-811. DOI: 10.3760/cma.j.cn501225-20240229-00078. [2] 韩春茂, 周业平, 孙永华, 等. 成人烧伤营养支持指南[J].中华烧伤杂志,2009,25(3):238-240. DOI: 10.3760/cma.j.issn.1009-2587.2009.03.030. [3] RousseauAF, LosserMR, IchaiC, et al. ESPEN endorsed recommendations: nutritional therapy in major burns[J]. Clin Nutr, 2013,32(4):497-502. DOI: 10.1016/j.clnu.2013.02.012. [4] The Japanese Society for Burn Injuries (JSBI) clinical practice guidelines for management of burn care (3rd edition)[J]. Acute Med Surg, 2022,9(1):e739. DOI: 10.1002/ams2.739. [5] GuyattGH, OxmanAD, VistGE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations[J]. BMJ, 2008,336(7650):924-926. DOI: 10.1136/bmj.39489.470347.AD. [6] World Health Organization WHO handbook for guideline development, 2nd Edition 2023-01-02 2025-02-06 https://www.who.int/publications/i/item/9789241548960 World Health Organization. WHO handbook for guideline development, 2nd Edition[EB/OL]. (2023-01-02)[2025-02-06]. https://www.who.int/publications/i/item/9789241548960.
[7] Centre for Evidence-Based Medicine Levels of evidence 2023-01-02 2025-02-06 https://www.cebm.ox.ac.uk/resources/levels-of-evidence Centre for Evidence-Based Medicine. Levels of evidence[EB/OL]. (2023-01-02)[2025-02-06]. https://www.cebm.ox.ac.uk/resources/levels-of-evidence.
[8] AtkinsD, BestD, BrissPA, et al. Grading quality of evidence and strength of recommendations[J]. BMJ, 2004,328(7454):1490. DOI: 10.1136/bmj.328.7454.1490. [9] PereiraCT, HerndonDN. The pharmacologic modulation of the hypermetabolic response to burns[J]. Adv Surg, 2005,39:245-261. DOI: 10.1016/j.yasu.2005.05.005. [10] FlynnMB. Nutritional support for the burn-injured patient[J]. Crit Care Nurs Clin North Am, 2004,16(1):139-144. DOI: 10.1016/j.ccell.2003.09.004. [11] DickersonRN, GervasioJM, RileyML, et al. Accuracy of predictive methods to estimate resting energy expenditure of thermally-injured patients[J]. JPEN J Parenter Enteral Nutr, 2002,26(1):17-29. DOI: 10.1177/014860710202600117. [12] McClaveSA, TaylorBE, MartindaleRG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.)[J]. JPEN J Parenter Enteral Nutr, 2016,40(2):159-211. DOI: 10.1177/0148607115621863. [13] MosierMJ, PhamTN, KleinMB, et al. Early enteral nutrition in burns: compliance with guidelines and associated outcomes in a multicenter study[J]. J Burn Care Res, 2011,32(1):104-109. DOI: 10.1097/BCR.0b013e318204b3be. [14] KhorasaniEN, MansouriF. Effect of early enteral nutrition on morbidity and mortality in children with burns[J]. Burns, 2010,36(7):1067-1071. DOI: 10.1016/j.burns.2009.12.005. [15] TrockiO, MicheliniJA, RobbinsST, et al. Evaluation of early enteral feeding in children less than 3 years old with smaller burns (8-25 per cent TBSA)[J]. Burns, 1995,21(1):17-23. DOI: 10.1016/0305-4179(95)90775-u. [16] Romanowski KS Overview of nutrition support in burn patients 2024-09-20 2025-02-06 https://www.uptodate.com/contents/overview-of-nutrition-support-in-burn-patients RomanowskiKS. Overview of nutrition support in burn patients [EB/OL]. (2024-09-20)[2025-02-06]. https://www.uptodate.com/contents/overview-of-nutrition-support-in-burn-patients.
[17] BulC. Nutrition treatment in pediatric burns patients[J]. Clin Sci Nutr, 2020,2(2):53-67. DOI: 10.5152/ClinSciNutr.2021.978. [18] Fleet SE Overview of enteral nutrition in infants and children 2024-10-11 2025-02-06 https://www.uptodate.com/contents/overview-of-enteral-nutrition-in-infants-and-children FleetSE. Overview of enteral nutrition in infants and children [EB/OL]. (2024-10-11)[2025-02-06]. https://www.uptodate.com/contents/overview-of-enteral-nutrition-in-infants-and-children.
[19] ShaL, ShiX, ZhuM, et al. Implementation of STRONGkids for identifying nutritional risk in outpatients of child health care clinics: results of a multicentre study[J]. Clin Nutr, 2023,42(11):2207-2213. DOI: 10.1016/j.clnu.2023.09.020. [20] HuysentruytK, AllietP, MuyshontL, et al. The STRONG(kids) nutritional screening tool in hospitalized children: a validation study[J]. Nutrition, 2013,29(11/12):1356-1361. DOI: 10.1016/j.nut.2013.05.008. [21] BangYK, ParkMK, JuYS, et al. Clinical significance of nutritional risk screening tool for hospitalised children with acute burn injuries: a cross-sectional study[J]. J Hum Nutr Diet, 2018,31(3):370-378. DOI: 10.1111/jhn.12518. [22] DelsoglioM, AchamrahN, BergerMM, et al. Indirect calorimetry in clinical practice[J]. J Clin Med, 2019,8(9):1387. DOI: 10.3390/jcm8091387. [23] JeonJ, KymD, ChoYS, et al. Reliability of resting energy expenditure in major burns: comparison between measured and predictive equations[J]. Clin Nutr, 2019, 38(6):2763-2769. DOI: 10.1016/j.clnu.2018.12.003. [24] GalfoM, De BellisA, MeliniF. Nutritional therapy for burns in children[J]. J Emerg Crit Care Med, 2018,2(6):154. DOI: 10.21037/jeccm.2018.05.11. [25] SumanOE, MlcakRP, ChinkesDL, et al. Resting energy expenditure in severely burned children: analysis of agreement between indirect calorimetry and prediction equations using the Bland-Altman method[J]. Burns, 2006,32(3):335-342. DOI: 10.1016/j.burns.2005.10.023. [26] LiusuwanRA, PalmieriTL, KinoshitaL, et al. Comparison of measured resting energy expenditure versus predictive equations in pediatric burn patients[J]. J Burn Care Rehabil, 2005,26(6):464-470. DOI: 10.1097/01.bcr.0000185786.38365.3d. [27] MayesT, GottschlichMM, KhouryJ, et al. Evaluation of predicted and measured energy requirements in burned children[J]. J Am Diet Assoc, 1996,96(1):24-29. DOI: 10.1016/s0002-8223(96)00008-9. [28] HeW, WangY, WangP, et al. Intestinal barrier dysfunction in severe burn injury[J/OL]. Burns Trauma, 2019,7:24[2025-02-06]. https://pubmed.ncbi.nlm.nih.gov/31372365/. DOI: 10.1186/s41038-019-0162-3. [29] WiseAK, HromatkaKA, MillerKR. Energy expenditure and protein requirements following burn injury[J]. Nutr Clin Pract, 2019,34(5):673-680. DOI: 10.1002/ncp.10390. [30] MochizukiH, TrockiO, DominioniL, et al. Mechanism of prevention of postburn hypermetabolism and catabolism by early enteral feeding[J]. Ann Surg, 1984, 200(3):297-310. DOI: 10.1097/00000658-198409000-00007. [31] RaffT, GermannG, HartmannB. The value of early enteral nutrition in the prophylaxis of stress ulceration in the severely burned patient[J]. Burns, 1997,23(4):313-318. DOI: 10.1016/s0305-4179(97)89875-0. [32] KnackstedtR, GatherwrightJ. The role of thermal injury on intestinal bacterial translocation and the mitigating role of probiotics: a review of animal and human studies[J]. Burns, 2020, 46(5):1005-1012. DOI: 10.1016/j.burns.2019.07.007. [33] SljivicS, ChriscoL, LongCA, et al. 529 outcomes of total parenteral nutrition use in burn patients at a single institution[J]. J Burn Care Res, 2022, 43(Suppl 1):S99-100. DOI: 10.1093/jbcr/irac012.159. [34] ChenZ, WangS, YuB, et al. A comparison study between early enteral nutrition and parenteral nutrition in severe burn patients[J]. Burns, 2007,33(6):708-712. DOI: 10.1016/j.burns.2006.10.380. [35] 谢玉生, 黄蓉蓉, 赵雪, 等. 成人重度烧伤患者肠内肠外营养的证据总结[J].中华护理杂志,2024,59(9):1106-1113. DOI: 10.3761/j.issn.0254-1769.2024.09.012. [36] ValentiniM, SeganfredoFB, FernandesSA. Pediatric enteral nutrition therapy for burn victims: when should it be initiated?[J]. Rev Bras Ter Intensiva, 2019,31(3):393-402. DOI: 10.5935/0103-507X.20190062. [37] ClarkA, ImranJ, MadniT, et al. Nutrition and metabolism in burn patients[J/OL]. Burns Trauma, 2017,5:11[2025-02-06]. https://pubmed.ncbi.nlm.nih.gov/?term=Nutrition+and+metabolism+in+burn+patients&filter=datesearch.y_10. DOI: 10.1186/s41038-017-0076-x. [38] HamptonV, HamptonT, DheansaB, et al. Evaluation of high protein intake to improve clinical outcome and nutritional status for patients with burns: a systematic review[J]. Burns, 2021,47(8):1714-1729. DOI: 10.1016/j.burns.2021.02.028. [39] 罗月, 黎宁. 严重烧伤患者早期肠内营养治疗的研究进展[J].中华烧伤杂志,2021,37(9):880-884. DOI: 10.3760/cma.j.cn501120-20210621-00223. [40] AlexanderJW, MacMillanBG, StinnettJD, et al. Beneficial effects of aggressive protein feeding in severely burned children[J]. Ann Surg, 1980,192(4):505-517. DOI: 10.1097/00000658-198010000-00009. [41] ChanMM, ChanGM. Nutritional therapy for burns in children and adults[J]. Nutrition, 2009,25(3):261-269. DOI: 10.1016/j.nut.2008.10.011. [42] GottschlichMM, JenkinsM, WardenGD, et al. Differential effects of three enteral dietary regimens on selected outcome variables in burn patients[J]. JPEN J Parenter Enteral Nutr, 1990,14(3):225-236. DOI: 10.1177/0148607190014003225. [43] GarrelDR, RaziM, LarivièreF, et al. Improved clinical status and length of care with low-fat nutrition support in burn patients[J]. JPEN J Parenter Enteral Nutr, 1995,19(6):482-491. DOI: 10.1177/0148607195019006482. [44] MastersB, AarabiS, SidhwaF, et al. High-carbohydrate, high-protein, low-fat versus low-carbohydrate, high-protein, high-fat enteral feeds for burns[J]. Cochrane Database Syst Rev, 2012,1:CD006122. DOI: 10.1002/14651858.CD006122.pub3. [45] SheridanRL, YuYM, PrelackK, et al. Maximal parenteral glucose oxidation in hypermetabolic young children: a stable isotope study[J]. JPEN J Parenter Enteral Nutr, 1998,22(4):212-216. DOI: 10.1177/0148607198022004212. [46] WolfeRR. Maximal parenteral glucose oxidation in hypermetabolic young children[J]. JPEN J Parenter Enteral Nutr, 1998,22(4):190. DOI: 10.1177/0148607198022004190. [47] HartDW, WolfSE, ZhangXJ, et al. Efficacy of a high-carbohydrate diet in catabolic illness[J]. Crit Care Med, 2001,29(7):1318-1324. DOI: 10.1097/00003246-200107000-00004. [48] ShieldsBA, VanFossonCA, PruskowskiKA, et al. High-carbohydrate vs high-fat nutrition for burn patients[J]. Nutr Clin Pract, 2019,34(5):688-694. DOI: 10.1002/ncp.10396. [49] LeeJO, GauglitzGG, HerndonDN, et al. Association between dietary fat content and outcomes in pediatric burn patients[J]. J Surg Res, 2011,166(1):e83-90. DOI: 10.1016/j.jss.2010.10.006. [50] ŻwierełłoW, StyburskiD, MaruszewskaA, et al. Bioelements in the treatment of burn injuries-the complex review of metabolism and supplementation (copper, selenium, zinc, iron, manganese, chromium and magnesium)[J]. J Trace Elem Med Biol, 2020,62:126616. DOI: 10.1016/j.jtemb.2020.126616. [51] NordlundMJ, PhamTN, GibranNS. Micronutrients after burn injury: a review[J]. J Burn Care Res, 2014,35(2):121-133. DOI: 10.1097/BCR.0b013e318290110b. [52] HerndonDN. Total burn care[M]. Fifth ed. Philadelphia:W.B. Saunders Company Ltd, 2018. [53] 中华医学会肠外肠内营养学分会儿科协作组. 中国儿科肠内肠外营养支持临床应用指南[J].中华儿科杂志,2010,26(6):436-441. DOI: 10.3760/cma.j.issn.0578-1310.2010.06.008. [54] ZdolsekHJ, LindahlOA, AngquistKA, et al. Non-invasive assessment of intercompartmental fluid shifts in burn victims[J]. Burns, 1998,24(3):233-240. DOI: 10.1016/s0305-4179(98)00016-3. [55] HartDW, WolfSE, HerndonDN, et al. Energy expenditure and caloric balance after burn: increased feeding leads to fat rather than lean mass accretion[J]. Ann Surg, 2002,235(1):152-161. DOI: 10.1097/00000658-200201000-00020. [56] GravesC, SaffleJ, MorrisS. Comparison of urine urea nitrogen collection times in critically ill patients[J]. Nutr Clin Pract, 2005,20(2):271-275. DOI: 10.1177/0115426505020002271. [57] RettmerRL, WilliamsonJC, LabbéRF, et al. Laboratory monitoring of nutritional status in burn patients[J]. Clin Chem, 1992,38(3):334-337. [58] GravesC, SaffleJ, CochranA. Actual burn nutrition care practices: an update[J]. J Burn Care Res, 2009,30(1):77-82. DOI: 10.1097/BCR.0b013e3181921f0d. [59] YangX, LiR, ZhaiJ, et al. Effects of early enteral nutrition in patients with severe burns: a systematic review[J]. Medicine (Baltimore), 2024,103(7):e37023. DOI: 10.1097/MD.0000000000037023. [60] ThakkarK, KienCL, RosenblattJI, et al. Diarrhea in severely burned children[J]. JPEN J Parenter Enteral Nutr, 2005,29(1):8-11. DOI: 10.1177/014860710502900108. [61] NSW Agency for Clinical Innovation Clinical Practice Guidelines Nutrition Burn Patient Management NSW Statewide Burn Injury Service 2024-09-15 2025-02-06 https://aci.health.nsw.gov.au/__data/assets/pdf_file/0009/162639/ACI-Clinical-practice-guidelines-nutrition-burn-patient-management.pdf NSW Agency for Clinical Innovation. Clinical Practice Guidelines Nutrition Burn Patient Management NSW Statewide Burn Injury Service[EB/OL]. (2024-09-15)[2025-02-06]. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0009/162639/ACI-Clinical-practice-guidelines-nutrition-burn-patient-management.pdf.
[62] 耿岚岚, 谢静. 儿童肠内营养应用的研究进展[J].中华实用儿科临床杂志,2019,34(7):481-484. DOI: 10.3760/cma.j.issn.2095-428X.2019.07.001. -

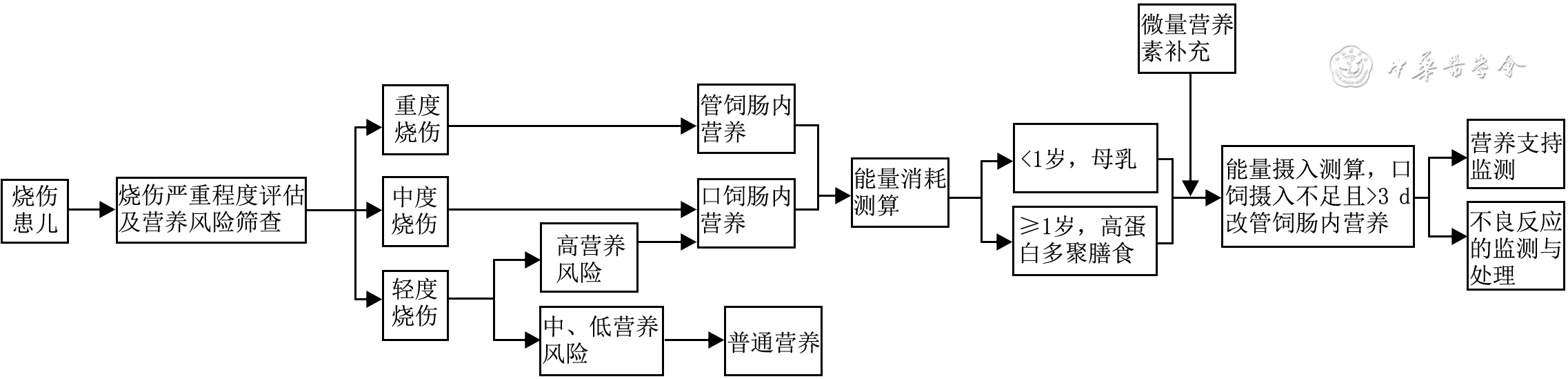
图 1 烧伤儿童肠内营养流程图
注:营养风险筛查采用营养状态和生长发育风险筛查工具;能量消耗测算采用Curreri公式(儿童版);<1岁患儿存在母乳禁忌证或母乳不足时,可选用强化铁配方奶;对口饲肠内营养进行能量摄入测算时,母乳能量密度按照每100毫升供能约300 kJ计算,配方奶及多聚膳食能量根据具体配方而定
Table 1. 2001版牛津大学循证医学中心证据等级标准
证据等级 具体描述 1a 同质RCT系统评价 1b 单个RCT(窄可信区间) 1c 全或无的病例报告,如传统治疗全部无效,系列病例报告全部死亡或存活 2a 同质队列研究的系统评价 2b 单个队列研究(包括低质量RCT,如随访率<80%的RCT) 2c 结果研究、生态学研究 3a 同质病例对照研究的系统评价 3b 单个病例对照研究 4 病例系列研究(包括低质量队列研究和病例对照研究) 5 基于经验,未经严格论证的专家意见 注:RCT为随机对照试验  下载: 导出CSV
下载: 导出CSV
Table 2. 营养状态和生长发育风险筛查工具的具体内容
评估项目 评估内容 分值(分) 无 有 主观临床评估 患儿是否营养不佳,包括肌肉和/或皮下脂肪减少和/或脸型消瘦 0 1 高营养风险疾病 患儿是否存在潜在的能引起营养不良的疾病,或者需要进行大手术。如,患儿存在神经性厌食、烧伤、支气管肺炎致呼吸困难、乳糜泻、囊性纤维化、早产或成熟障碍、慢性心脏病、传染病、炎症性肠病、癌症、慢性肝病、慢性肾病、胰腺炎、短肠综合征、肌肉疾病、代谢性疾病、创伤、精神障碍/发育迟缓等 0 2 营养摄入与丢失情况 是否存在以下情况中的1种:(1)最近几天,大便次数≥5次/d或呕吐次数≥3次/d;(2)入院前摄入减少;(3)入院前已进行营养干预;(4)因为疼痛缺乏足够的摄入 0 1 体重减轻或增加困难 在近几周/月内体重下降或1岁以下儿童体重增加缓慢 0 1 注:该表译自参考文献[19];总分为0表示营养不良低风险,1~3分表示营养不良中等风险,4~5分表示营养不良高风险
下载: 导出CSV
Table 3. Curreri公式(儿童版)
年龄(岁) 计算方法 <1 基础能量+15×烧伤总面积 1~3 基础能量+25×烧伤总面积 4~15 基础能量+40×烧伤总面积 注:该表译自参考文献[24];能量单位为kcal,1 kcal=4 184 J;基础能量估算如下,患儿年龄≤6个月为110~120 kcal·kg-1·d-1,7~12个月为95~100 kcal·kg-1·d-1,>1岁且≤3岁为90~100 kcal·kg-1·d-1,4~6岁为80~90 kcal·kg-1·d-1,7~12岁为70~85 kcal·kg-1·d-1,13~14岁为44~55 kcal·kg-1·d-1,15岁(接近成人)为50~60 kcal·kg-1·d-1
下载: 导出CSV
-
 王燕妮完整网刊.mp4
王燕妮完整网刊.mp4

-

 下载:
下载:



计量
- 文章访问数: 3388
- HTML全文浏览量: 902
- PDF下载量: 96
- 被引次数: 0
