




Effects of early debridement and conservative eschar removal followed by wound coverage with acellular dermal matrix in the treatment of children with deep burns
-
摘要:
目的 探讨早期清创保守去痂后外覆脱细胞真皮基质(ADM)即早期手术治疗小儿深度烧伤的效果。 方法 该研究为回顾性队列研究。2017年1月—2022年12月,山东第一医科大学附属中心医院收治符合入选标准的1~7岁住院深度烧伤患儿278例。根据治疗过程不同,将行早期手术+常规换药治疗的134例患儿纳入去痂+换药组[男77例、女57例,年龄1(1,2)岁],将仅行常规换药治疗的144例患儿纳入单纯换药组[男90例、女54例,年龄1(1,2)岁]。将去痂+换药组中无Ⅲ度烧伤的51例患儿纳入去痂+换药1组[男26例、女25例,年龄1(1,2)岁],将该组存在Ⅲ度烧伤的83例患儿中未在早期手术的同期行自体皮移植(称为早期植皮)的57例患儿纳入去痂+换药2组[男37例、女20例,年龄1(1,2)岁]。将单纯换药组中无Ⅲ度烧伤的76例患儿纳入单纯换药1组[男51例、女25例,年龄1(1,3)岁],将该组存在Ⅲ度烧伤的68例患儿纳入单纯换药2组[男39例、女29例,年龄1(1,2)岁]。针对去痂+换药组深Ⅱ度和较小面积Ⅲ度烧伤创面,以保留薄层变性真皮从而保全创基健康组织为基准进行去痂,去痂后创面均外敷ADM;针对该组较大面积Ⅲ度烧伤创面,尤其是位于关节功能部位的创面,则去痂至有生机组织平面并行早期植皮。当患儿较浅创面已愈合或趋于愈合后评估残余创面情况,若其难以在14 d内治愈则行择期自体皮移植。统计去痂+换药组、单纯换药组以及去痂+换药1组、单纯换药1组患儿深Ⅱ度烧伤创面的愈合时间、干预愈合时间、手术/换药次数、干预手术/换药次数。末次随访(随访期设为7~12个月)时,统计去痂+换药组54例、单纯换药组48例患儿深Ⅱ度烧伤愈合创面瘢痕增生最严重区域的改良温哥华瘢痕量表(mVSS)评分。统计去痂+换药组、单纯换药组患儿全部烧伤创面愈合时间及手术/换药次数,以及去痂+换药2组、单纯换药2组患儿Ⅲ度烧伤创面愈合时间及手术/换药次数。统计去痂+换药组、单纯换药组患儿创面愈合期间创面感染、脓毒症、发热及烧伤5 d后发热发生情况。 结果 与单纯换药组相比,去痂+换药组患儿深Ⅱ度烧伤创面的愈合时间、干预愈合时间均明显缩短,手术/换药次数和干预手术/换药次数均明显减少( Z值分别为-11.00、-11.33、-12.64、-11.65, P<0.05)。与单纯换药1组相比,去痂+换药1组患儿深Ⅱ度烧伤创面的愈合时间、干预愈合时间均明显缩短,手术/换药次数和干预手术/换药次数均明显减少( Z值分别为6.57、6.46、8.04、6.57, P<0.05)。末次随访时,去痂+换药组54例患儿深Ⅱ度烧伤愈合创面瘢痕增生最严重区域的mVSS评分为4.00(3.00,5.00)分,明显低于单纯换药组48例患儿的6.50(5.00,7.00)分( Z=-4.67, P<0.05)。与单纯换药组相比,去痂+换药组患儿全部烧伤创面愈合时间明显缩短,手术/换药次数明显减少( Z值分别为-5.20、-6.34, P值均<0.05);与单纯换药2组相比,去痂+换药2组患儿Ⅲ度烧伤创面愈合时间明显缩短,手术/换药次数明显减少( Z值分别为-5.22、-5.73, P值均<0.05)。创面愈合期间,去痂+换药组患儿发热、烧伤5 d后发热概率均明显低于单纯换药组( χ 2值分别为4.13、3.91, P<0.05),仅单纯换药组1例患儿发生脓毒症,2组患儿创面感染发生率比较的差异无统计学意义( P>0.05)。 结论 对小儿深度烧伤创面行早期手术并根据需要行早期植皮或择期自体皮移植术,其近远期效果优于不行早期手术。 Abstract:Objective To explore the effects of early debridement and conservative eschar removal followed by wound coverage with acellular dermal matrix (ADM), i.e., early surgery, in the treatment of children with deep burns. Methods This study was a retrospective cohort study. From January 2017 to December 2022, 278 deep burned hospitalized children aged 1-7 years who met the inclusion criteria were admitted to Central Hospital Affiliated to Shandong First Medical University. According to the differences in treatment processes, 134 children who underwent early surgery+routine dressing change were enrolled in eschar removal+dressing change group (77 males and 57 females, aged 1 (1, 2) years), and 144 children who underwent only routine dressing change were enrolled in dressing change alone group (90 males and 54 females, aged 1 (1, 2) years). Fifty-one children without full-thickness burns in eschar removal+dressing change group were enrolled in eschar removal+dressing change group 1 (26 males and 25 females, aged 1 (1, 2) years), and 57 cases of the 83 children with full-thickness burns who did not undergo autologous skin grafting at the same time of early surgery (namely early skin grafting) in eschar removal+dressing change group were included in eschar removal+dressing change group 2 (37 males and 20 females, aged 1 (1, 2) years). Seventy-six children without full-thickness burns in dressing change alone group were included in dressing change alone group 1 (51 males and 25 females, aged 1 (1, 3) years), and 68 children with full-thickness burns in dressing change alone group were included in dressing change alone group 2 (39 males and 29 females, aged 1 (1, 2) years). For deep partial-thickness burn wounds and small full-thickness burn wounds in eschar removal+dressing change group, the eschar removal was performed on the basis of retaining a thin layer of denatured dermis so as to preserve the healthy tissue of the wound base, and ADM was applied to all wounds externally after eschar removal. For larger full-thickness burn wounds in this group, especially those located in the functional part of joints, eschar removal to the plane layer of viable tissue and early autologous skin grafting was needed. When the superficial wounds of children healed or tended to heal, the residual wounds were evaluated, and elective autologous skin grafting was performed if it was difficult to heal within 14 days. The healing time, intervention healing time, times of operation/dressing change, and times of intervention operation/dressing change in children with deep partial-thickness burn wounds of children in eschar removal+dressing change group, dressing change alone group, eschar removal+dressing change group 1, and dressing change alone group 1 were recorded. At the last follow-up (follow-up period was set to 7-12 months), the modified Vancouver scar scale (mVSS) scores of the most severe area of scar hyperplasia of healed deep partial-thickness burn wounds of 54 children in eschar removal+dressing change group and 48 children in dressing change alone group were recorded. The healing time and times of operation/dressing change of all burn wounds of children in eschar removal+dressing change group and dressing change alone group, and the healing time and times of operation/dressing change of full-thickness burn wounds of children in eschar removal+dressing change group 2 and dressing change alone group 2 were recorded. The incidences of wound infection, sepsis, fever, and fever after 5 days of burns in children of eschar removal+dressing change group and dressing change alone group during wound healing. Results Compared with those in dressing change alone group, the healing time and intervention healing time were significantly shortened, and the times of operation/dressing change and times of intervention operation/dressing change were significantly reduced in children with deep partial-thickness burn wounds in eschar removal+dressing change group (with Z values of -11.00, -11.33, -12.64, and -11.65, respectively, P<0.05). Compared with those in dressing change alone group 1, the healing time and intervention healing time were significantly shortened, and the times of operation/dressing change and times of intervention operation/dressing change were significantly reduced in children with deep partial-thickness burn wounds in eschar removal+dressing change group 1 (with Z values of 6.57, 6.46, 8.04, and 6.57, respectively, P<0.05). At the last follow-up, the mVSS score of the most severe scar hyperplasia area of healed deep partial-thickness burn wounds of 54 children in eschar removal+dressing change group was 4.00 (3.00,5.00), which was significantly lower than 6.50 (5.00,7.00) of 48 children in dressing change alone group ( Z =-4.67, P<0.05).Compared with those in dressing change alone group, the healing time was significantly shortened, and times of operation/dressing change was significantly reduced in all burn wounds in eschar removal+dressing change group (with Z values of -5.20 and -6.34, respectively, P<0.05). Compared with those in dressing change alone group 2, the healing time was significantly shortened, and times of operation/dressing change was significantly reduced in full-thickness burn wounds in eschar removal+dressing change group 2 (with Z values of -5.22 and -5.73, respectively, P<0.05). During wound healing, the probabilities of fever and fever after 5 days of burns in children of eschar removal+dressing change group were significantly lower than those in dressing change alone group (with χ 2 values of 4.13 and 3.91, respectively, P<0.05); only 1 child in dressing change alone group developed sepsis, and there was no statistically significant difference in the wound infection rate of children in the two groups ( P>0.05). Conclusions For children with deep burns, early surgery, and early skin grafting or elective autologous skin grafting as needed, have better short-term and long-term effects than those without early surgery. -
Key words:
- Burns /
- Child /
- Debridement /
- Deep partial-thickness burns /
- Full-thickness burns /
- Eschar removal /
- Acellular dermal matrix
-
参考文献
(32) [1] BurdA,YuenC.A global study of hospitalized paediatric burn patients[J].Burns,2005,31(4):432-438.DOI: 10.1016/j.burns.2005.02.016. [2] HanD,WeiY,LiY,et al.Epidemiological and clinical characteristics of 5,569 pediatric burns in central China from 2013 to 2019[J].Front Public Health,2022,10:751615.DOI: 10.3389/fpubh.2022.751615. [3] YangJ,TianG,LiuJ,et al.Epidemiology and clinical characteristics of burns in mainland China from 2009 to 2018[J/OL].Burns Trauma,2022,10:tkac039[2023-07-20]. https://pubmed.ncbi.nlm.nih.gov/36196302/.DOI: 10.1093/burnst/tkac039. [4] 张成, 彭源, 罗小强, 等. 3 067例住院烧伤患儿流行病学调查及其感染的病原学特征分析[J]. 中华烧伤杂志, 2021, 37(6):538-545. DOI: 10.3760/cma.j.cn501120-20210201-00044. [5] KaźmierskiM,MańkowskiP,JankowskiA,et al.Comparison of the results of operative and conservative treatment of deep dermal partial-thickness scalds in children[J].Eur J Pediatr Surg,2007,17(5):354-361.DOI: 10.1055/s-2006-924646. [6] 中华医学会烧伤外科学分会.儿童深Ⅱ度烧伤创面处理专家共识(2023版)[J].中华烧伤与创面修复杂志,2023,39(10):901-910.DOI: 10.3760/cma.j.cn501225-20230730-00026. [7] 宋国栋,石文,高聪,等.大面积深度烧伤的早期切除与皮肤移植[J/CD].中华损伤与修复杂志(电子版),2017,12(1):56-60.DOI: 10.3877/cma.j.issn.1673-9450.2017.07.010. [8] BrownsonEG, GibranNS. Evaluation of the burn wound: management decisions[M]//Herndon DN. Total burn care. 5th ed. Philadelphia: Elsevier, 2018:87-92. [9] IsmailalyME, DannounM, JimenezCJ, et al. Operative wound management[M]//Herndon DN. Total burn care. 5th ed. Philadelphia: Elsevier, 2018:114-130. [10] SongG,JiaJ,MaY,et al.Experience and efficacy of surgery for retaining viable subcutaneous tissue in extensive full-thickness burns[J].Burns,2016,42(1):71-80.DOI: 10.1016/j.burns.2015.06.012. [11] 宋国栋,贾军,马印东,等.削痂皮下组织创面植皮术治疗大面积Ⅲ度烧伤患者的效果[J].中华医学杂志,2014,(44):3492-3496.DOI: 10.3760/cma.j.issn.0376-2491.2014.44.010. [12] 中华医学会烧伤外科学分会,海峡两岸医药卫生交流协会暨烧创伤组织修复专委会.Ⅱ度烧伤创面治疗专家共识(2024版)Ⅱ:手术治疗和感染防治[J].中华烧伤与创面修复杂志,2024,40(2):101-118.DOI: 10.3760/cma.j.cn501225-20240112-00015. [13] KaganRJ,PeckMD,AhrenholzDH,et al.Surgical management of the burn wound and use of skin substitutes: an expert panel white paper[J].J Burn Care Res,2013,34(2):e60-79.DOI: 10.1097/BCR.0b013e31827039a6. [14] 宋国栋,高聪,石文,等.灾害性群体烧伤早期救治的现状及思考[J].中华医学杂志,2017,97(6):401-405.DOI: 10.3760/cma.j.issn.0376-2491.2017.06.001. [15] GreenhalghDG.Management of burns[J].N Engl J Med,2019,380(24):2349-2359.DOI: 10.1056/NEJMra1807442. [16] 李峰,迟云飞,胡泉,等.伤后早期微创削痂治疗小儿躯干及四肢深Ⅱ度烧伤创面的效果[J].中华烧伤杂志,2018,34(10):714-718.DOI: 10.3760/cma.j.issn.1009-2587.2018.10.012. [17] 李利根.防治深Ⅱ度烧伤创面早期加深的研究进展[J/CD].中华临床医师杂志(电子版),2012,6(18):5397-5400.DOI: 10.3877/cma.j.issn.1674-0785.2012.18.003. [18] 赖青鸿,张友来,辛国华.烧伤早期创面加深机制与防治措施的研究进展[J].中华烧伤杂志,2019,35(3):229-232.DOI: 10.3760/cma.j.issn.1009-2587.2019.03.014. [19] BaryzaMJ,BaryzaGA.The Vancouver Scar Scale: an administration tool and its interrater reliability[J].J Burn Care Rehabil,1995,16(5):535-538.DOI: 10.1097/00004630-199509000-00013. [20] HoranTC,AndrusM,DudeckMA.CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting[J].Am J Infect Control,2008,36(5):309-332.DOI: 10.1016/j.ajic.2008.03.002. [21] 姚咏明,张卉,童亚林.深化对烧伤脓毒症诊断体系与治疗策略的认识[J].中华烧伤杂志,2021,37(5):404-409.DOI: 10.3760/cma.j.cn501120-20200703-00337. [22] SeymourCW,LiuVX,IwashynaTJ,et al.Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3)[J].JAMA,2016,315(8):762-774.DOI: 10.1001/jama.2016.0288. [23] ČapekKD,CulnanDM,DesaiMH,et al.Fifty years of burn care at Shriners hospitals for children, Galveston[J].Ann Plast Surg,2018,80(3 Suppl 2):S90-94.DOI: 10.1097/SAP.0000000000001376. [24] 李梦芸,毛远桂,郭光华,等.水动力清创系统在各类烧伤创面清创手术中的应用[J].中华烧伤杂志,2016,32(9):574-576.DOI: 10.3760/cma.j.issn.1009-2587.2016.09.014. [25] LegemateCM,KwaK,GoeiH,et al.Hydrosurgical and conventional debridement of burns: randomized clinical trial[J].Br J Surg,2022,109(4):332-339.DOI: 10.1093/bjs/znab470. [26] 辛乃军,韩梅,宋国栋.手部深度烧伤的临床评估与早期治疗[J/CD].中华损伤与修复杂志(电子版),2020,15(3):223-226.DOI: 10.3877/cma.j.issn.1673-9450.2020.03.015. [27] JeschkeMG,HerndonDN.Burns in children: standard and new treatments[J].Lancet,2014,383(9923):1168-1178.DOI: 10.1016/S0140-6736(13)61093-4. [28] MatsumuraH,EngravLH,GibranNS,et al.Cones of skin occur where hypertrophic scar occurs[J].Wound Repair Regen,2001,9(4):269-277.DOI: 10.1046/j.1524-475x.2001.00269.x. [29] ChiY,YinH,ChenX,et al.Effect of precise partial scab removal on the repair of deep partial-thickness burn wounds in children: a retrospective study[J].Transl Pediatr,2021,10(11):3014-3022.DOI: 10.21037/tp-21-500. [30] 贾晓明.异种(体)生物材料与创面修复[J/CD].中华损伤与修复杂志(电子版),2020,15(5):341-346.DOI: 10.3877/cma.j.issn.1673-9450.2020.05.003. [31] CubisonTC,PapeSA,ParkhouseN.Evidence for the link between healing time and the development of hypertrophic scars (HTS) in paediatric burns due to scald injury[J].Burns,2006,32(8):992-999.DOI: 10.1016/j.burns.2006.02.007. [32] LvK, XiaZ, Chinese consensus panel on the prevention and treatment of scars. Chinese expert consensus on clinical prevention and treatment of scar[J/OL]. Burns Trauma, 2018,6:27[2023-07-20]. https://pubmed.ncbi.nlm.nih.gov/30263894/. DOI: 10.1186/s41038-018-0129-9. -

1 早期清创保守去痂后外覆脱细胞真皮基质(ADM)联合常规换药治疗例1患儿颈和腰背部深Ⅱ度烫伤创面的效果。1A.伤后3 d术前创面;1B.伤后3 d清创保守去痂后创面;1C.创面经图1B处理后外覆ADM;1D.术后7 d,创面周围区域ADM分离修剪后,可见ADM与创面中央区域贴附紧密、部分较浅创面已上皮化;1E.术后11 d,部分ADM仍与创基贴附密切,大部分创面愈合;1F.术后26 d,愈合创面呈红色,局部有表皮擦伤和斑片状轻微增生;1G.伤后3个月,愈合创面整体色素沉着减退,有粟粒样和斑片状瘢痕;1H.伤后7个月,瘢痕呈混合色素沉着但大体接近周围肤色,局部有斑片状平软瘢痕

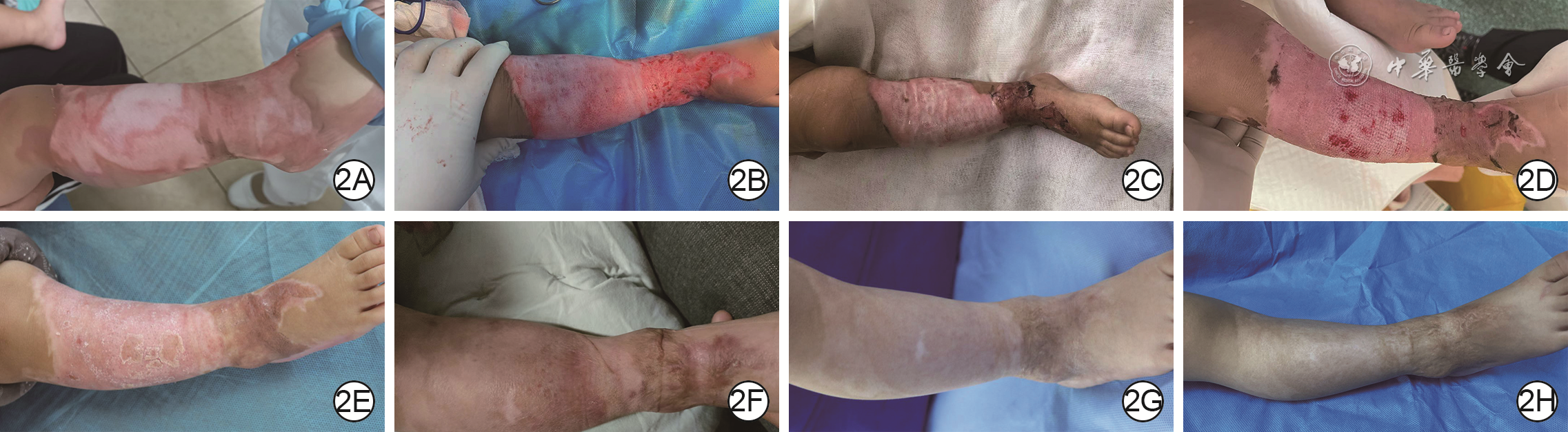
2 早期清创保守去痂后外覆脱细胞真皮基质(ADM)+中厚自体皮移植联合常规换药治疗例2患儿右小腿和右踝部深度烫伤创面的效果。2A.伤后3 d创面外观;2B.伤后5 d,行保守去痂(右小腿)和削痂(右踝)后创面外观;2C.术后5 d去除ADM后创面与植皮创面情况;2D.术后11 d,大部分创面愈合;2E.术后30 d,愈合创面脱屑,植皮区域瘢痕轻微增生;2F.伤后4个月,部分愈合创面发红,局灶性瘢痕增生;2G.伤后7个月,小腿部色素沉者减退,有斑片状平软瘢痕,踝部植皮轻微挛缩;2H.伤后12个月,小腿创面颜色与周围皮肤接近,踝部植皮柔软
表1 去痂+换药组与单纯换药组住院深度烧伤患儿临床资料比较
表1. Comparison of clinical data of hospitalized children with deep burns in eschar removal+dressing change group and dressing change alone group
组别 例数 性别(例) 年龄[岁, M( Q 1, Q 3)] 伤后入院时间[h, M( Q 1, Q 3)] 烧伤总面积[%TBSA, M( Q 1, Q 3)] 深Ⅱ度烧伤面积[%TBSA, M( Q 1, Q 3)] Ⅲ度烧伤面积1[%TBSA, M( Q 1, Q 3)] Ⅲ度烧伤面积2[%TBSA, M( Q 1, Q 3)] 男 女 去痂+换药组 134 77 57 1(1,2) 3.00(2.00,17.00) 15.0(10.0,20.0) 8.0(6.0,10.0) 0.5(0,1.0) a 0(0,1.0) b 单纯换药组 144 90 54 1(1,2) 2.25(1.00,9.00) 13.5(10.0,17.8) 7.0(6.0,10.0) 0(0,1.0) 0(0,1.0) 统计量值 χ 2=0.73 Z=-0.31 Z=-1.00 Z=-1.62 Z=-0.92 Z=-3.26 Z=-0.50 P值 0.391 0.756 0.319 0.105 0.355 0.001 0.619 注:去痂+换药指行早期清创保守去痂后外覆脱细胞真皮基质+常规换药治疗,单纯换药指仅行常规换药治疗;TBSA为体表总面积; a指去痂+换药组中83例Ⅲ度烧伤患儿Ⅲ度烧伤面积, b指去痂+换药组中57例未行早期自体皮移植手术的Ⅲ度烧伤患儿Ⅲ度烧伤面积;单纯换药组共68例患儿有Ⅲ度烧伤;2组所有患儿都有深Ⅱ度烧伤  下载: 导出CSV
下载: 导出CSV
表2 去痂+换药1组与单纯换药1组住院深度烧伤患儿临床资料比较
表2. Comparison of clinical data of hospitalized children with deep burns in eschar removal+dressing change group 1 and dressing change alone group 1
组别 例数 性别(例) 年龄[岁, M( Q 1, Q 3)] 伤后入院时间[h, M( Q 1, Q 3)] 烧伤总面积[%TBSA, M( Q 1, Q 3)] 深Ⅱ度烧伤面积[%TBSA, M( Q 1, Q 3)] 男 女 去痂+换药1组 51 26 25 1(1,2) 3.00(2.00,17.00) 15.0(10.0,20.0) 8.0(5.0,11.0) 单纯换药1组 76 51 25 1(1,3) 2.25(1.00,22.00) 10.5(10.0,15.0) 7.0(6.0,8.0) 统计量值 χ 2 =3.32 Z=0.23 Z=-0.78 Z=-1.10 Z=-1.00 P值 0.068 0.821 0.437 0.057 0.319 注:去痂+换药1组患儿为行早期清创保守去痂后外覆脱细胞真皮基质+常规换药治疗且无Ⅲ度烧伤的患儿,单纯换药1组患儿为仅行常规换药治疗且无Ⅲ度烧伤的患儿;TBSA指体表总面积
下载: 导出CSV
表3 去痂+换药2组与单纯换药2组住院深度烧伤患儿临床资料比较
表3. Comparison of clinical data of hospitalized children with deep burns in eschar removal+dressing change group 2 and dressing change alone group 2
组别 例数 性别(例) 年龄[岁, M( Q 1, Q 3)] 伤后入院时间[h, M( Q 1, Q 3)] 烧伤总面积[%TBSA, M( Q 1, Q 3)] 深Ⅱ度烧伤面积[%TBSA, M( Q 1, Q 3)] Ⅲ度烧伤面积[%TBSA, M( Q 1, Q 3)] 择期自体皮移植[例(%)] 男 女 去痂+换药2组 57 37 20 1(1,2) 3.00(1.25,10.50) 15.0(10.0,20.0) 8.0(6.0,10.0) 1.0(0.5,1.0) 11(19.30) 单纯换药2组 68 39 29 1(1,2) 2.50(1.00,5.75) 15.0(12.0,20.0) 8.0(6.0,10.8) 1.0(0.5,1.0) 14(20.59) 统计量值 χ 2=0.74 Z=-0.64 Z=-0.41 Z=-0.25 Z=-0.27 Z=-0.62 χ 2=0.03 P值 0.389 0.523 0.681 0.806 0.784 0.537 0.857 注:去痂+换药2组患儿为行早期清创保守去痂后外覆脱细胞真皮基质+常规换药治疗且存在Ⅲ度烧伤但未行早期自体皮移植的患儿,单纯换药2组患儿为仅行常规换药治疗且存在Ⅲ度烧伤的患儿;TBSA为体表总面积
下载: 导出CSV
表4 4组住院烧伤患儿深Ⅱ度烧伤创面愈合及干预指标比较[ M( Q 1, Q 3)]
表4. Comparison of healing and intervention indexes of deep partial-thickness burn wounds of hospitalized children with burns in the four groups
组别 例数 愈合时间(d) 干预愈合时间(d) 手术/换药次数 a 干预手术/换药次数 a 去痂+换药组 134 18.00(17.00,19.00) 13.00(12.00,14.00) 5(5,6) 4(4,4) 单纯换药组 144 22.00(20.25,24.00) 17.00(16.00,19.75) 7(7,8) 6(5,6) 去痂+换药1组 51 18.00(17.00,19.00) 13.00(12.00,15.00) 5(5,6) 4(4,4) 单纯换药1组 76 21.00(19.00,24.00) 17.00(14.25,19.00) 7(6,8) 5(5,6) Z 1值 -11.00 -11.33 -12.64 -11.65 P 1值 <0.001 <0.001 <0.001 <0.001 Z 2值 6.57 6.46 8.04 6.57 P 2值 <0.001 <0.001 <0.001 <0.001 注:去痂+换药组患儿为行早期清创保守去痂后外覆脱细胞真皮基质(ADM)+常规换药治疗的患儿,单纯换药组患儿为仅行常规换药治疗的患儿,去痂+换药1组患儿为行早期清创保守去痂后外覆ADM+常规换药治疗且无Ⅲ度烧伤的患儿,单纯换药1组患儿为仅行常规换药治疗且无Ⅲ度烧伤的患儿; a其中的手术指早期清创保守去痂后外覆ADM和择期自体皮移植手术; Z 1值、 P 1值为去痂+换药组与单纯换药组各指标比较所得, Z 2值、 P 2值为去痂+换药1组与单纯换药1组各指标比较所得
下载: 导出CSV
-
 梁艳.mp4
梁艳.mp4

-

 下载:
下载:





计量
- 文章访问数: 9287
- HTML全文浏览量: 1317
- PDF下载量: 66
- 被引次数: 0
