




Establishment and validation of a risk prediction model for pulmonary embolism in severe burn patients
-
摘要:
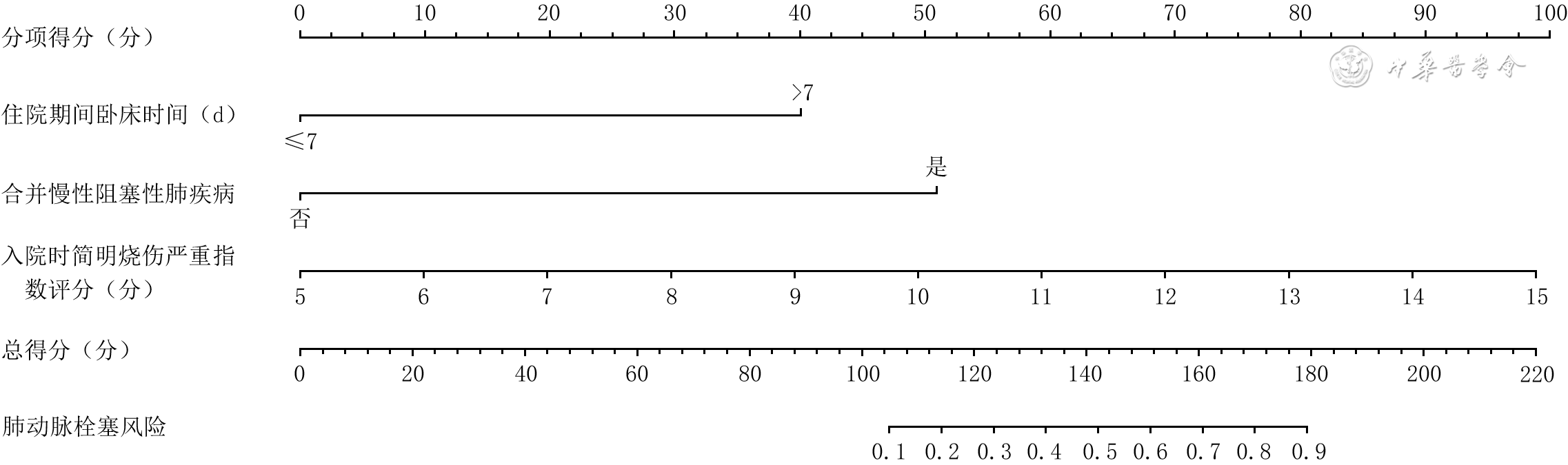
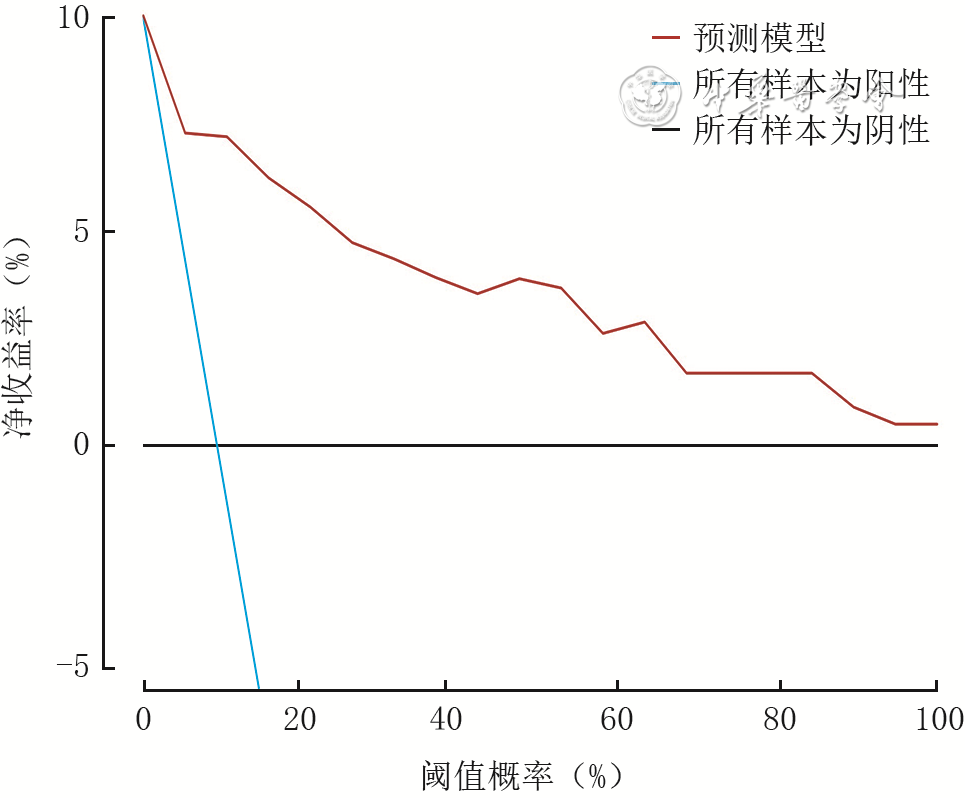
目的 筛选严重烧伤患者并发肺动脉栓塞的危险因素,据此构建风险预测模型并进行验证。 方法 该研究为回顾性病例系列研究。收集2020年3月—2023年3月武汉市第三医院烧伤科收治的符合入选标准的267例严重烧伤患者的临床资料,其中男159例、女108例,年龄18~82岁。根据是否并发肺动脉栓塞将患者分为肺动脉栓塞组(26例)与非肺动脉栓塞组(241例),收集并比较2组患者性别、年龄、体重指数、治疗期间卧床时间、烧伤原因、入院时白蛋白水平、合并慢性阻塞性肺疾病(COPD)情况、合并糖尿病情况、合并高血压情况、合并吸入性损伤情况和入院时简明烧伤严重指数(ABSI)评分。对组间比较差异有统计学意义的指标进行单因素和多因素logistic回归分析,筛选267例严重烧伤患者并发肺动脉栓塞的独立危险因素,并据此构建列线图预测模型。通过受试者操作特征(ROC)曲线评估预测模型的性能,采用校准曲线和临床决策曲线分析法对预测模型进行验证。 结果 肺动脉栓塞组患者中>60岁、治疗期间卧床时间>7 d、合并COPD、合并糖尿病患者比例(χ2值分别为7.75、29.15、29.86、5.94),入院时ABSI评分(t=6.01)均明显高于非肺动脉栓塞组(P<0.05)。2组患者其余资料比较,差异均无统计学意义(P>0.05)。单因素logistic回归分析显示,年龄、治疗期间卧床时间、合并COPD、合并糖尿病、入院时ABSI评分均为严重烧伤患者并发肺动脉栓塞的危险因素(比值比分别为3.40、14.87、17.78、2.80、1.88,95%置信区间分别为1.38~8.39、4.34~50.98、4.63~68.22、1.19~6.58、1.47~2.41,P<0.05)。多因素logistic回归分析显示,治疗期间卧床时间>7 d、合并COPD、入院时ABSI评分高均为严重烧伤患者并发肺动脉栓塞的独立危险因素(比值比分别为11.02、30.82、1.86,95%置信区间分别为2.76~43.98、3.55~267.33、1.38~2.50,P<0.05)。根据前述3个独立危险因素构建严重烧伤患者并发肺动脉栓塞风险列线图预测模型。预测模型的ROC曲线显示,ROC曲线下面积为0.91(95%置信区间为0.82~0.99),取最佳阈值25%时,预测模型的敏感度为84.6%、特异度为93.4%;校准曲线显示,预测模型校准曲线在理想曲线附近,Cox回归的一致性指数为0.80(95%置信区间为0.74~0.87);临床决策曲线显示,该模型的阈值概率范围为1%~98%,其净收益率>0。 结论 严重烧伤患者并发肺动脉栓塞的独立危险因素包括治疗期间卧床时间>7 d、合并COPD、入院时ABSI评分高,据此构建的列线图预测模型对严重烧伤患者并发肺动脉栓塞具有较佳的预测价值。 Abstract:Objective To screen the risk factors for pulmonary embolism in severe burn patients, based on which, a risk prediction model was established and validated. Methods This study was a retrospective case series study. The clinical data of 267 severe burn patients who met the inclusion criteria and were admitted to the Department of Burns of Wuhan Third Hospital from March 2020 to March 2023 were collected, including 159 males and 108 females, aged 18-82 years. The patients were divided into pulmonary embolism group (26 cases) and non-pulmonary embolism group (241 cases) according to whether they were complicated with pulmonary embolism. The following data of patients in the 2 groups were collected and compared, including gender, age, body mass index, bedtime during treatment, cause of burn, albumin level on admission, combination of chronic obstructive pulmonary disease (COPD), combination of diabetes mellitus, combination of hypertension, combination of inhalation injury, and the abbreviated burn severity index (ABSI) on admission. The indicators with statistically significant differences between the two groups were conducted with univariate and multivariate logistic regression analyses to identify the independent risk factors for pulmonary embolism in 267 severe burn patients. Based on these findings, a nomogram prediction model was established. The performance of the prediction model was evaluated by the receiver operating characteristic (ROC) curve, while its validation was conducted through calibration curve and clinical decision curve analysis. Results The proportions of beyond 60 years old, bedtime over 7 days during treatment, combination of COPD, and combination of diabetes mellitus (with χ2 values of 7.75, 29.15, 29.86, and 5.94, respectively), and ABSI score on admission (t=6.01) of patients in pulmonary embolism group were significantly higher than those in non-pulmonary embolism group (P<0.05). There were no statistically significant differences in the other indicators between the two groups of patients (P>0.05). The univariate logistic regression analysis showed that age, bedtime during treatment, combination of COPD, combination of diabetes mellitus, and ABSI score on admission were the risk factors for pulmonary embolism in severe burn patients (with odds ratios of 3.40, 14.87, 17.78, 2.80, and 1.88, respectively, 95% confidence intervals of 1.38-8.39, 4.34-50.98, 4.63-68.22, 1.19-6.58, and 1.47-2.41, respectively, P<0.05). The multivariate logistic regression analysis showed that bedtime over 7 days during treatment, combination of COPD, and high ABSI score on admission were the independent risk factors for pulmonary embolism in severe burn patients (with odds ratios of 11.02, 30.82, and 1.86, respectively, 95% confidence intervals of 2.76-43.98, 3.55-267.33, and 1.38-2.50, respectively, P<0.05). Based on the three aforementioned independent risk factors, a nomogram prediction model for the risk of pulmonary embolism in severe burn patients was established. The ROC curve of prediction model showed that the area under the ROC curve was 0.91 (with 95% confidence interval of 0.82-0.99). When the optimal cut-off value of 25% was taken, the sensitivity and specificity of prediction model was 84.6% and 93.4%, respectively. The calibration curve showed that the calibration curve of prediction model was around the ideal curve, with a consistency index of 0.80 in Cox regression (with 95% confidence interval of 0.74-0.87). The clinical decision curve showed that the threshold probability value of the prediction model was in the range of 1% to 98%, with net return rate over 0. Conclusions The independent risk factors for pulmonary embolism in severe burn patients include bedtime over 7 days during treatment, combination of COPD, and high ABSI score on admission. The nomogram prediction model established based on this has good predictive value for complicated pulmonary embolism in severe burn patients. -
Key words:
- Burns /
- Risk factors /
- Nomograms /
- Pulmonary embolism
-
参考文献
(61) [1] BurgessM, ValderaF, VaronD, et al. The immune and regenerative response to burn injury[J]. Cells, 2022,11(19):3073. DOI: 10.3390/cells11193073. [2] 马琪敏,汤文彬,李孝建,等.危重烧伤老年患者早期临床特征的多中心回顾分析及预后的危险因素分析[J].中华烧伤与创面修复杂志,2024,40(3):249-257.DOI: 10.3760/cma.j.cn501225-20230808-00042. [3] FranckCL, SenegagliaAC, LeiteLMB, et al. Influence of adipose tissue-derived stem cells on the burn wound healing process[J]. Stem Cells Int, 2019,2019:2340725. DOI: 10.1155/2019/2340725. [4] Radzikowska-BüchnerE, ŁopuszyńskaI, FliegerW, et al. An overview of recent developments in the management of burn injuries[J]. Int J Mol Sci, 2023, 24(22): 16357. DOI: 10.3390/ijms242216357. [5] SangitaC,GarimaG,JayanthiY,et al.Histological indicators of cutaneous lesions caused by electrocution, flame burn and impact abrasion[J].Med Sci Law,2018,58(4):216-221.DOI: 10.1177/0025802418776116. [6] FalsterC,HellfritzschM,GaistTA,et al.Comparison of international guideline recommendations for the diagnosis of pulmonary embolism[J].Lancet Haematol,2023,10(11):e922-e935.DOI: 10.1016/S2352-3026(23)00181-3. [7] ChenX,LiuX,LiuJ,et al.Pulmonary embolism secondary to deep venous thrombosis: a retrospective and observational study for clinical characteristics and risk stratification[J].Phlebology,2021,36(8):627-635.DOI: 10.1177/0268355521990964. [8] HuSS,Writing Committee of the Report on Cardiovascular Health and Diseases in China.Pulmonary embolism and deep venous thrombosis in China[J].J Geriatr Cardiol,2024,21(8):775-778.DOI: 10.26599/1671-5411.2024.08.007. [9] NaumAG,JariI,MoisiiL,et al.Imaging and biomarkers: the assesment of pulmonary embolism risk and early mortality[J].Medicina (Kaunas),2024,60(9):1489.DOI: 10.3390/medicina60091489. [10] SebastianR,GhanemO,DiRomaF,et al.Pulmonary embolism in burns, is there an evidence based prophylactic recommendation? Case report and review of literature[J].Burns,2015,41(2):e4-7.DOI: 10.1016/j.burns.2014.06.018. [11] CastanonL, BhogadiSK, AnandT, et al. The association between the timing of initiation of pharmacologic venous thromboembolism prophylaxis with outcomes in burns patients[J]. J Burn Care Res, 2023, 44(6): 1311-1315. DOI: 10.1093/jbcr/irad074. [12] MohammedAQI, BermanL, StaroselskyM, et al. Clinical presentation and risk stratification of pulmonary embolism[J]. Int J Angiol, 2024,33(2):82-88. DOI: 10.1055/s-0044-1786878. [13] KobayashiT, PuglieseS, SethiSS, et al. Contemporary management and outcomes of patients with high-risk pulmonary embolism[J]. J Am Coll Cardiol, 2024, 83(1): 35-43. DOI: 10.1016/j.jacc.2023.10.026. [14] VrettouCS,DimaE,SigalaI.Pulmonary embolism in critically ill patients-prevention, diagnosis, and management[J].Diagnostics (Basel),2024,14(19):2208.DOI: 10.3390/diagnostics14192208. [15] 中华医学会呼吸病学分会肺栓塞与肺血管病学组,中国医师协会呼吸医师分会肺栓塞与肺血管病工作委员会,全国肺栓塞与肺血管病防治协作组.肺血栓栓塞症诊治与预防指南[J].中华医学杂志,2018,98(14):1060-1087.DOI: 10.3760/cma.j.issn.0376-2491.2018.14.007. [16] KhanAY, WaheedF, RehanM, et al. Hematological trends in severe burn patients: a comprehensive study for prognosis and clinical insights[J]. J Burn Care Res, 2024,45(5):1315-1320. DOI: 10.1093/jbcr/irae057. [17] HuY,MaoQ,YeS,et al.Blast-burn combined injury followed by immediate seawater immersion induces hemodynamic changes and metabolic acidosis: an experimental study in a canine model[J].Clin Lab,2016,62(7):1193-1199.DOI: 10.7754/Clin.Lab.2015.150929. [18] KayaAT,AkmanB.Relationship of the novel scoring system for lower extremity venous thrombosis with pulmonary embolism[J].Acad Radiol,2024,31(9):3811-3824.DOI: 10.1016/j.acra.2024.03.010. [19] HuangS,MaQ,LiaoX,et al.Identification of early coagulation changes associated with survival outcomes post severe burns from multiple perspectives[J].Sci Rep,2024,14(1):10457.DOI: 10.1038/s41598-024-61194-0. [20] KrugerE, KowalS, BilirSP, et al. Relationship between patient characteristics and number of procedures as well as length of stay for patients surviving severe burn injuries: analysis of the American Burn Association National Burn Repository[J]. J Burn Care Res, 2020,41(5):1037-1044. DOI: 10.1093/jbcr/iraa040. [21] Alcalá-CerrilloM,González-SánchezJ,González-BernalJJ,et al.Retrospective study of the epidemiological-clinical characteristics of burns treated in a hospital emergency service (2018-2022)[J].Nurs Rep,2024,14(3):1987-1997.DOI: 10.3390/nursrep14030148. [22] DuffettL. Deep venous thrombosis[J]. Ann Intern Med, 2022, 175(9): ITC129-ITC144. DOI: 10.7326/AITC202209200. [23] FeathersJR,RichardsonG,CornierA,et al.The use of Oxandrolone in the management of severe burns: a multi-service survey of burns centres and units across the United Kingdom[J].Cureus,2024,16(3):e57167.DOI: 10.7759/cureus.57167. [24] Ter MeulenEW,PoleyMJ,Van DijkM,et al.The hospital costs associated with acute paediatric burn injuries[J].S Afr Med J,2016,106(11):1120-1124.DOI: 10.7196/SAMJ.2016.v106i11.11202. [25] LiuHY, WuYJ, HuangSC, et al.Experiences with pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension at multiple centers in Taiwan[J]. J Formos Med Assoc, 2022, 121(3):604-612. DOI: 10.1016/j.jfma.2021.07.023. [26] BruntonN,McBaneR,CasanegraAI,et al.Risk stratification and management of intermediate-risk acute pulmonary embolism[J].J Clin Med,2024,13(1):257.DOI: 10.3390/jcm13010257. [27] 吕琴,何雅,高慎敏.肺栓塞患者合并阻塞性睡眠呼吸暂停发病率及危险因素Meta分析[J].四川医学,2023,44(4):349-355.DOI: 10.16252/j.cnki.issn1004-0501-2023.04.003. [28] SökücüSN,SatıcıC,Tokgöz AkyılF,et al.The impact of deep venous thrombosis on 90 day mortality in chronic obstructive pulmonary disease patients presenting with pulmonary embolism[J].Respir Med Res,2024,85:101090.DOI: 10.1016/j.resmer.2024.101090. [29] CastellanaG,IntigliettaP,DragonieriS,et al.Incidence of deep venous thrombosis in patients with both pulmonary embolism and COPD[J].Acta Biomed,2021,92(3):e2021210.DOI: 10.23750/abm.v92i3.11258. [30] AhmedI, KhanK, AkhterN, et al.Frequency of asymptomatic deep vein thrombosis in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease (COPD)[J]. Cureus, 2024,16(9):e69858. DOI: 10.7759/cureus.69858. [31] 蒋秋玲,袁媛,郑婧.胸部恶性肿瘤胸腔镜术后肺栓塞发生的危险因素与治疗效果分析[J].实用癌症杂志,2022,37(10):1646-1648,1652.DOI: 10.3969/j.issn.1001-5930.2022.10.021. [32] CouturaudF, BertolettiL, PastreJ, et al. Prevalence of pulmonary embolism among patients with COPD hospitalized with acutely worsening respiratory symptoms[J]. JAMA, 2021, 325(1): 59-68. DOI: 10.1001/jama.2020.23567. [33] YuHY, BaiYP, SongXC, et al. Factors associated with acute pulmonary embolism in patients with hypoxia after off-pump coronary artery bypass grafting: a case-control study[J]. J Multidiscip Healthc, 2024,17:573-583. DOI: 10.2147/JMDH.S447534. [34] TangS,MeiZ,HuangD,et al.Comparative analysis of hemoglobin, potassium, sodium, and glucose in arterial blood gas and venous blood of patients with COPD[J].Sci Rep,2024,14(1):5194.DOI: 10.1038/s41598-024-55992-9. [35] LiuS,ZhangH,ZhuP,et al.Predictive role of red blood cell distribution width and hemoglobin-to-red blood cell distribution width ratio for mortality in patients with COPD: evidence from NHANES 1999-2018[J].BMC Pulm Med,2024,24(1):413.DOI: 10.1186/s12890-024-03229-w. [36] HultcrantzM,ModlitbaA,VasanSK,et al.Hemoglobin concentration and risk of arterial and venous thrombosis in 1.5 million Swedish and Danish blood donors[J].Thromb Res,2020,186:86-92.DOI: 10.1016/j.thromres.2019.12.011. [37] 刘艳洁,余瑞雪,王莉,等.慢性阻塞性肺疾病患者住院期间发生肺栓塞的危险因素分析[J].血管与腔内血管外科杂志,2023,9(7):881-884.DOI: 10.19418/j.cnki.issn2096-0646.2023.07.24. [38] ZhouR,ZhangJ,ZhangW,et al.Clinical efficacy and safety of Panax notoginseng saponins in treating chronic obstructive pulmonary disease with blood hypercoagulability: a meta-analysis of randomized controlled trials[J].Phytomedicine,2024,125:155244.DOI: 10.1016/j.phymed.2023.155244. [39] LiuX, JiaoX, GongX, et al. Prevalence, risk factor and clinical characteristics of venous thrombus embolism in patients with acute exacerbation of COPD: a prospective multicenter study[J]. Int J Chron Obstruct Pulmon Dis, 2023,18: 907-917. DOI: 10.2147/COPD.S410954. [40] JiménezD, AgustíA, TaberneroE, et al. Effect of a pulmonary embolism diagnostic strategy on clinical outcomes in patients hospitalized for COPD exacerbation: a randomized clinical trial[J]. JAMA, 2021, 326(13): 1277-1285. DOI: 10.1001/jama.2021.14846. [41] LiR,ZengJ,SunD,et al.The challenges of identifying pulmonary embolism in patients hospitalized for exacerbations of COPD[J/OL].Respir Med Res,2024,86:101122(2024-06-22)[2024-11-20].https://pubmed.ncbi.nlm.nih.gov/38972110/.DOI:10.1016/j.resmer.2024.101122.[published online ahead of print]. [42] de Miguel-DíezJ,JiZ.Exploring predictors of pulmonary embolism in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease[J].Eur J Intern Med,2024:S0953-6205(24)00452-00457.DOI: 10.1016/j.ejim.2024.11.003. [43] LiJ,XiongY,LiS,et al.Prevalence and risk factors of pulmonary embolism in COPD patients complicated with secondary polycythemia[J].Int J Chron Obstruct Pulmon Dis,2024,19:2371-2385.DOI: 10.2147/COPD.S481905. [44] DowlingAR,LukeCE,CaiQ,et al.Modulation of interleukin-6 and its effect on late vein wall injury in a stasis mouse model of deep vein thrombosis[J].JVS Vasc Sci,2022,3:246-255.DOI: 10.1016/j.jvssci.2022.04.001. [45] NajemMY,RysRN,LauranceS,et al.Extracellular RNA induces neutrophil recruitment via toll-like receptor 3 during venous thrombosis after vascular injury[J].J Am Heart Assoc,2024,13(15):e034492.DOI: 10.1161/JAHA.124.034492. [46] Bordeanu-DiaconescuEM, Grosu-BulardaA, FrunzaA, et al. Venous thromboembolism in burn patients: a 5-year retrospective study[J]. Medicina (Kaunas), 2024, 60(2): 258. DOI: 10.3390/medicina60020258. [47] HuY,OuS,FengQ,et al.Incidence and predictors of perioperative atrial fibrillation in burn intensive care unit patients following burn surgery[J].Burns,2022,48(5):1092-1096.DOI: 10.1016/j.burns.2022.04.012. [48] ZhouX,ZhangL,CaiJ,et al.Application areas of intermittent pneumatic compression in the prevention of deep vein thrombosis during dixon surgery: a randomized, controlled trial[J].Clin Ther,2023,45(10):977-982.DOI: 10.1016/j.clinthera.2023.07.022. [49] GuzelA,CanbazS.A retrospective assessment of venous recanalization outcomes for oral anticoagulant treatment in deep vein thrombosis[J].Vascular,2024:17085381241236931.DOI: 10.1177/17085381241236931. [50] TongM,ZhangS,MaP,et al.Efficacy analysis of intermittent pneumatic compression combined with hyperthermia at different temperatures for prevention of deep vein thrombosis after simulated orthopaedic surgery in male rabbits[J].Am J Transl Res,2024,16(10):5337-5346.DOI: 10.62347/OXES9217. [51] BrownC,TokessyL,DellucA,et al.Risk of developing post thrombotic syndrome after deep vein thrombosis with different anticoagulant regimens: a systematic review and pooled analysis[J].Thromb Res,2024,240:109057.DOI: 10.1016/j.thromres.2024.109057. [52] HardtK, WapplerF, SakkaSG. Uncertain acute hemodynamic instability after severe burn injury: an (un-)usual complication[J]. Anasthesiol Intensivmed Notfallmed Schmerzther, 2020,55(3):190-199. DOI: 10.1055/a-1014-9098. [53] DeeterL, SeatonM, CarrougherGJ, et al. Hospital-acquired complications alter quality of life in adult burn survivors: report from a burn model system[J]. Burns, 2019,45(1):42-47. DOI: 10.1016/j.burns.2018.10.010. [54] 孙淑英,文大林,陈国昇,等.严重多发伤患者脓毒症发生的相关危险因素及其预警效能分析[J].中华创伤杂志,2023,39(5):443-449.DOI: 10.3760/cma.j.cn501098-20230201-00055. [55] LiuA, MinasianRA, ManiagoE, et al. Venous thromboembolism chemoprophylaxis in burn patients: a literature review and single-institution experience[J]. J Burn Care Res, 2021, 42(1): 18-22. DOI: 10.1093/jbcr/iraa143. [56] SchallerC,PetitpierreA,von FeltenS,et al.Thromboembolic events in burn patients: an analysis of risk factors and different anticoagulants[J].Burns,2024,50(3):569-577.DOI: 10.1016/j.burns.2023.12.014. [57] FosterKN,ChunduKR,LalS,et al.Invasive Aspergillus infection leading to vascular thrombosis and amputation in a severely burned child[J].J Burn Care Res,2017,38(1):e464-e468.DOI: 10.1097/BCR.0000000000000366. [58] KimballA,GibsonE,QuinnL,et al.Thrombosis incidence in major paediatric burns[J].ANZ J Surg,2023,93(11):2721-2726.DOI: 10.1111/ans.18664. [59] MurphyKD,LeeJO,HerndonDN.Current pharmacotherapy for the treatment of severe burns[J].Expert Opin Pharmacother,2003,4(3):369-384.DOI: 10.1517/14656566.4.3.369. [60] StantonE, YenikomshianHA, GillenwaterJ. 754 Venous Thromboembolism incidence and risk factors in burn patients[J]. J Burn Care Res. 2024,45(Suppl 1):S230. DOI: 10.1093/jbcr/irae036.296. [61] StantonEW, ManasyanA, ThompsonCM,et al. Venous thromboembolism incidence, risk factors, and prophylaxis in burn patients: a national trauma database study[J/OL]. J Burn Care Res, 2024:irae171(2024-09-11)[2024-12-10]. https://academic.oup.com/jbcr/advance-article/doi/10.1093/jbcr/irae171/7755309.DOI: 10.1093/jbcr/irae171. published online ahead of print. -
Table 1. 2组严重烧伤患者临床资料比较
组别 例数 性别(例) 年龄(例) 体重指数(例) 治疗期间卧床时间(例) 入院时白蛋白水平(例) 合并COPD(例) 男 女 >60岁 ≤60岁 ≥24 kg/m2 <24 kg/m2 >7 d ≤7 d >35 g/L ≤35 g/L 是 否 肺动脉栓塞组 26 13 13 19 7 14 12 23 3 16 10 6 20 非肺动脉栓塞组 241 146 95 107 134 170 71 82 159 176 65 4 237 统计量值 χ2=1.09 χ2=7.75 χ2=3.05 χ2=29.15 χ2=1.53 χ2=29.86 P值 0.296 0.005 0.081 <0.001 0.216 <0.001 注:COPD为慢性阻塞性肺疾病,ABSI为简明烧伤严重指数  下载: 导出CSV
下载: 导出CSV
Table 2. 267例严重烧伤患者并发肺动脉栓塞的单因素和多因素logistic回归分析结果
自变量 单因素 多因素 回归系数 标准误 比值比 95%置信区间 P值 回归系数 标准误 比值比 95%置信区间 P值 年龄(岁) 1.22 0.46 3.40 1.38~8.39 P值 0.94 0.61 2.56 0.78~8.45 0.123 治疗期间卧床时间(>7 d) 2.70 0.63 14.87 4.34~50.98 0.008 2.40 0.71 11.02 2.76~43.98 0.001 合并COPD 2.88 0.69 17.78 4.63~68.22 <0.001 3.43 1.10 30.82 3.55~267.33 0.002 合并糖尿病 1.03 0.44 2.80 1.19~6.58 <0.001 0.68 0.63 1.97 0.58~6.69 0.279 入院时ABSI评分(10.7~14.9分) 0.63 0.13 1.88 1.47~2.41 <0.001 0.62 0.15 1.86 1.38~2.50 <0.001 注:COPD为慢性阻塞性肺疾病,ABSI为简明烧伤严重指数
下载: 导出CSV
-

 下载:
下载:




图(5) / 表(2)
计量
- 文章访问数: 4579
- HTML全文浏览量: 901
- PDF下载量: 40
- 被引次数: 0
