




Clinical application effects of the "novel three-longitude and five-transverse method" for perforator localization of anterolateral thigh chimeric flaps
-
摘要:
目的 探讨“新型三纵五横法”在股前外侧嵌合皮瓣穿支定位中的临床应用效果。 方法 该研究为回顾性病例系列研究。2021年6月—2023年6月,遵义医科大学附属医院收治15例符合入选标准的肢体毁损性创面患者,创面位于上肢者5例、下肢者10例,清创后创面面积为12 cm×5 cm~22 cm×7 cm。采用“新型三纵五横法”,以髂前上棘为P点、髌骨外上缘为A点、股骨外上髁为B点,分别将P点与A、B点连接,形成PA、PB线,连接P点与A、B点连线的中点(C点),得到PC线;从PA线中点引一垂线为E线,将E线向近端平移5 cm为D线,向远端分别平移5、10、15 cm为F、G、H线;PA和PB线分别与D、E、F、G、H线相交,形成Ⅰ、Ⅱ、Ⅲ、Ⅳ区。以PC线为皮瓣轴线,在此区域内设计并切取股前外侧嵌合皮瓣修复创面,皮瓣切取面积为13.0 cm×6.0 cm~23.0 cm×8.0 cm。将供区创面行减张缝合。术中记录观察到的各区域内穿支数量、来源及穿支入皮点至PC线的垂直距离。术后观察皮瓣成活情况。随访时观察皮瓣色泽、质地、外形及并发症情况,供区瘢痕增生、肌疝发生情况。 结果 术中共观察到75条穿支,其中18条穿支位于Ⅰ区(3条来源于旋股外侧动脉斜支、15条来源于旋股外侧动脉降支),17条穿支位于Ⅱ区(均来源于旋股外侧动脉降支),21条穿支位于Ⅲ区(均来源于旋股外侧动脉降支),19条穿支位于Ⅳ区(12条来源于旋股外侧动脉降支、7条来源于大腿下段周边血管)。24条穿支入皮点位于PC线上,51条穿支入皮点位于PC线旁,其至PC线的垂直距离均<1.0 cm。术后1例患者皮瓣远端出现淤紫,2例患者皮瓣边缘少量渗液,均经换药后愈合;其余患者皮瓣顺利成活。术后6~40个月随访时,皮瓣色泽、质地、外形均良好,无并发症发生,供区瘢痕增生不明显,无肌疝发生。 结论 “新型三纵五横法”可有效定位股前外侧嵌合皮瓣穿支,方法简单、可靠,基于该方法设计与切取的股前外侧嵌合皮瓣修复肢体毁损性创面的临床效果良好,值得推广。 Abstract:Objective To evaluate the clinical application effects of the "novel three-longitude and five-transverse method" for perforator localization in anterolateral thigh chimeric flaps. Methods This study was a retrospective study of case series. From June 2021 to June 2023, 15 patients with destructive limb wounds who met the inclusion criteria were admitted to the Affiliated Hospital of Zunyi Medical University. The wounds were located on the upper limbs in 5 cases and the lower limbs in 10 cases, with a post-debridement area ranging from 12 cm×5 cm to 22 cm×7 cm. The "novel three-longitude and five-transverse method" was employed. The anterior superior iliac spine was defined as Point P, the superolateral border of patella was defined as Point A, and the lateral femoral epicondyle was defined as Point B. Point P was connected with Points A and B to form Lines PA and PB. The Point P was connected to the midpoint of the line connecting Points A and B (Point C) to form Line PC. A perpendicular line was drawn from the midpoint of Line PA as Line E. Line E was translated 5 cm proximally to form Line D, while Lines F, G, and H were drawn 5, 10, and 15 cm distally, respectively. The intersections of Lines PA and PB with Lines D, E, F, G, and H were defined as Zones Ⅰ, Ⅱ, Ⅲ, and Ⅳ, respectively. Using Line PC as the flap axis, anterolateral thigh chimeric flaps were designed and harvested within the areas to repair the wounds. The area of harvested flap ranged from 13.0 cm×6.0 cm to 23.0 cm×8.0 cm. The donor site wounds were sutured with tension reduction. During surgery, the number and origin of perforators observed in each zone, as well as the vertical distance from the skin entry point of the perforator to Line PC were recorded. After surgery, flap survival was observed. During follow-up, the color, texture, appearance, and occurrence of complications of flaps, as well as the occurrence of hyperplastic scar formation and muscle herniation in donor sites were observed. Results During surgery, a total of 75 perforators was identified. Of those perforators, 18 were located in Zone Ⅰ (three originating from the oblique branch of lateral circumflex femoral artery and 15 originating from the descending branch of lateral circumflex femoral artery), 17 were located in Zone Ⅱ (all originating from the descending branch of lateral circumflex femoral artery), 21 were located in Zone Ⅲ (all originating from the descending branch of lateral circumflex femoral artery), and 19 were located in Zone Ⅳ (12 originating from the descending branch of lateral circumflex femoral artery and 7 originating from the peripheral vessels in distal thigh). The skin entry points of 24 perforators were located directly on Line PC, while the skin entry points of the other 51 perforators were located adjacent to it, with the vertical distances to Line PC all less than 1.0 cm. After surgery, one patient developed distal flap bruising, and two patients had minor exudation at the flap margin, which all healed after dressing changes. The flaps in the remaining patients survived smoothly. During the follow-up period of 6 to 40 months, all flaps demonstrated favorable color, texture, and appearance, with no complications observed; the scars in donor sites were mild, with no muscle herniation. Conclusions The "novel three-longitude and five-transverse method" can effectively locate anterolateral thigh chimeric flap perforators. The method is simple and reliable. The anterolateral thigh chimeric flaps designed and harvested based on this method have good clinical effect in repairing destructive limb wounds, which is worthy of promotion. -
参考文献
(40) [1] 杨亮,周荣,巨积辉,等.游离双侧股前外侧内增压型串联皮瓣修复足踝部大面积创面的临床疗效[J].中华烧伤与创面修复杂志,2025,41(1):61-69.DOI: 10.3760/cma.j.cn501225-20240508-00164. [2] 周耀,唐林峰,杨林,等.以旋股外侧动脉斜支和降支为蒂的股前外侧穿支皮瓣修复四肢创面效果的对比[J].中华显微外科杂志,2025,48(4):373-381.DOI: 10.3760/cma.j.cn441206-20241119-00251. [3] 韩飞,张万福,佟琳,等.阔筋膜-股前外侧皮瓣复合移植修复颌面部根治性肿瘤切除术后复杂缺损的临床效果[J].中华烧伤与创面修复杂志,2025,41(5):440-446.DOI: 10.3760/cma.j.cn501225-20240801-00290. [4] AliRS,Bluebond-LangnerR,RodriguezED,et al.The versatility of the anterolateral thigh flap[J].Plast Reconstr Surg,2009,124(6Suppl):Se395-Se407.DOI: 10.1097/PRS.0b013e3181bcf05c. [5] ChaHG,HurJ,AhnC,et al.Ultrathin anterolateral thigh free flap: an adipocutaneous flap with the most superficial elevation plane[J].Plast Reconstr Surg,2023,152(4):718e-723e.DOI: 10.1097/PRS.0000000000010295. [6] MelecaJB, KerrRP, PrendesBL, et al. Anterolateral thigh fascia lata rescue flap: a new weapon in the battle against osteoradionecrosis[J].Laryngoscope, 2021, 131(12): 2688-2693. DOI: 10.1002/lary.29709. [7] 徐永清,唐举玉,刘元波,等.股前外侧皮瓣穿支解剖学特征与定位方法的专家共识(2024版)[J].中国临床解剖学杂志,2024,42(5):489-499.DOI: 10.13418/j.issn.1001-165x.2024.5.01. [8] IllgC, KraussS, LauerH, et al. Precision of dynamic infrared thermography in anterolateral thigh flap planning: identification of the perforator fascia passage[J]. J Reconstr Microsurg, 2023, 39(6): 413-418. DOI: 10.1055/s-0042-1758183. [9] ViscontiG, BianchiA, HayashiA, et al. Designing an anterolateral thigh flap using ultrasound[J]. J Reconstr Microsurg, 2022, 38(3): 206-216. DOI: 10.1055/s-0041-1740126. [10] HuY, WangY, CaoS, et al. Customizing anterolateral thigh flap with magnetic resonance angiography differential subsampling with cartesian ordering imaging for individualized reconstruction of extremity defects[J]. J Surg Res, 2023, 283: 733-742. DOI: 10.1016/j.jss.2022.11.036. [11] KimS,LeeHR,YunJH,et al.Preoperative perforator localization in anterolateral thigh free flap using acoustic Doppler and computed tomography angiography[J].Laryngoscope Investig Otolaryngol,2022,7(6):1790-1797.DOI: 10.1002/lio2.958. [12] YuXX,YangSF,JiCS,et al.A novel computed tomography angiography technique: guided preoperative localization and design of anterolateral thigh perforator flap[J].Insights Imaging,2022,13(1):190.DOI: 10.1186/s13244-022-01318-0. [13] 李贤海,周建东,郑杰,等.红外热成像结合高频彩色多普勒超声定位浅筋膜穿支在超薄股前外侧皮瓣切取中的应用[J].中华显微外科杂志,2024,47(6):635-640.DOI: 10.3760/cma.j.cn441206-20240205-00041. [14] 张宇轩,许亚军,周建东,等.宽频线阵容积探头引导下三维超声技术在股前外侧穿支皮瓣术前穿支定位中的应用[J].中华显微外科杂志,2024,47(1):17-21.DOI: 10.3760/cma.j.cn441206-20230815-00015. [15] 周飞亚,张弦,蔡乐益,等.精准定位的微型股前外侧穿支皮瓣修复手指中等面积皮肤软组织缺损的效果[J].中华烧伤与创面修复杂志,2024,40(2):165-171.DOI: 10.3760/cma.j.cn501225-20231030-00150. [16] 董帅,王石,滕志成,等.吲哚菁绿血管造影联合彩色多普勒超声在股前外侧穿支皮瓣穿支定位中的临床应用效果[J].中华烧伤与创面修复杂志,2025,41(11):1091-1100.DOI: 10.3760/cma.j.cn501225-20240629-00254. [17] XuDC,ZhongSZ,KongJM,et al.Applied anatomy of the anterolateral femoral flap[J].Plast Reconstr Surg,1988,82(2):305-310. [18] YuP,YoussefA.Efficacy of the handheld Doppler in preoperative identification of the cutaneous perforators in the anterolateral thigh flap[J].Plast Reconstr Surg,2006,118(4):928-933.DOI: 10.1097/01.prs.0000232216.34854.63. [19] DengC, ChangS, WeiZ, et al. Alternative design for anterolateral thigh multi-paddled flaps: the 3-5 system[J]. Med Sci Monit, 2018, 24: 9102-9109. DOI: 10.12659/MSM.911883. [20] 常树森,魏在荣,金文虎,等.股前外侧皮瓣三纵五横法设计方案的临床研究[J].中华整形外科杂志,2019,35(6):571-576.DOI: 10.3760/cma.j.issn.1009-4598.2019.06.011. [21] 胡涛涛,常树森,魏在荣,等.改良三纵五横法在股前外侧穿支皮瓣修复术前穿支定位中的应用研究[J].中国修复重建外科杂志,2021,35(8):1027-1032.DOI: 10.7507/1002-1892.202103074. [22] 常树森,莫小金,魏在荣,等. 遵义缝合法在股前外侧皮瓣供区缝合中的应用研究[J]. 中国修复重建外科杂志,2021,35(4):477-482. DOI: 10.7507/1002-1892.202008101. [23] 魏在荣,王达利,黄广涛.毁损性创面的治疗进展[J/OL].中华损伤与修复杂志(电子版),2019,14(2):85-90[2024-05-20]. https://rs.yiigle.com/cmaid/1129420.DOI: 10.3877/cma.j.issn.1673-9450.2019.02.002. [24] 胡大海,张月.毁损性创面修复重建技术及策略探索[J].中华烧伤与创面修复杂志,2024,40(9):812-817.DOI: 10.3760/cma.j.cn501225-20240807-00296. [25] MarttilaE, SalliM, MesimäkiK, et al. The combined anterolateral thigh-partial iliac crest minihybrid free flap for mandibular reconstruction[J]. Microsurgery, 2022, 42(4): 312-318. DOI: 10.1002/micr.30854. [26] DI SummaPG, WatfaW, CampisiC, et al. Free versus pedicled anterolateral thigh flap for abdominal wall reconstruction[J]. Anticancer Res, 2019, 39(12): 6759-6768. DOI: 10.21873/anticanres.13891. [27] SơnTT, NghĩaPT, DungPTV, et al. Facial reconstruction with thinned anterolateral thigh free flap[J]. BMC Surg, 2024, 24(1): 296. DOI: 10.1186/s12893-024-02587-w. [28] YangZ, XuC, ZhuY, et al. Flow-through free anterolateral thigh flap in reconstruction of severe limb injury[J]. Ann Plast Surg, 2020, 84(5S Suppl 3): S165-S170. DOI: 10.1097/SAP.0000000000002372. [29] 吴育煜,胡朝波,陈绵川,等.股前内侧穿支内增压技术在股前外侧穿支皮瓣修复大面积缺损中的应用[J].组织工程与重建外科杂志,2023,19(2):141-145.DOI: 10.3969/j.issn.1673-0364.2023.02.007. [30] 赵铭,李涛.联体形式的股前外侧穿支皮瓣修复特殊类型创面的临床应用[J].中华显微外科杂志,2018,41(2):181-184.DOI: 10.3760/cma.j.issn.1001-2036.2018.02.022. [31] 巨积辉,李雷,徐磊,等.双血供来源的超长胸脐联体穿支皮瓣修复前臂大面积皮肤缺损[J].中华显微外科杂志,2018,41(2):137-141.DOI: 10.3760/cma.j.issn.1001-2036.2018.02.009. [32] 杨锐,高伟航,张子阳,等.静脉超引流技术在逆行旋股外侧动脉降支穿支皮瓣修复膝关节软组织缺损中的应用效果[J].中华创伤杂志,2025,41(4):387-390.DOI: 10.3760/cma.j.cn501098-20241127-00672. [33] MatsuiC,EscandónJM,MohammadA,et al.Clinical applications of the chimeric anterolateral thigh (ALT) flap in head and neck reconstruction[J].Acta Chir Belg,2023,123(5):473-480.DOI: 10.1080/00015458.2022.2073016. [34] WangKC, HungKS, ChangTY, et al. Temporary ectopic implantation of an amputated leg using the distal runoff vessel of the anterolateral thigh flap followed by subsequent prefabricated chimeric replantation[J]. Ann Plast Surg, 2019, 82(1): 71-75. DOI: 10.1097/SAP.0000000000001630. [35] ChenX, ZhangC, ChengL, et al. Survival and versatility of the flow-through lateral-thigh free flap in severe electrical injuries to the wrist[J]. Ann Plast Surg, 2020, 85(6): 612-617. DOI: 10.1097/SAP.0000000000002355. [36] 尹善青,竺枫,黄耀鹏,等.修薄的股前外侧穿支皮瓣联合分指及指蹼成形术序贯治疗全手脱套毁损性创面的效果[J].中华烧伤与创面修复杂志,2024,40(11):1052-1058.DOI: 10.3760/cma.j.cn501225-20240723-00275. [37] HsiehF, LeowOQY, CheongCF, et al. Musculoseptocutaneous perforator of anterolateral thigh flap: a clinical study[J]. Plast Reconstr Surg, 2021, 147(1): 103e-110e. DOI: 10.1097/PRS.0000000000007471. [38] 孙浩然,欧阳阳钢,刘璐,等.接合神经的游离股前外侧穿支皮瓣修复前足缺损的疗效[J].实用手外科杂志,2024,38(4):435-438.DOI: 10.3969/j.issn.1671-2722.2024.04.003. [39] 陈占斌,曹广超,杨龙,等.带阔筋膜游离股前外侧皮瓣修复伴肌腱缺损的创面[J].实用手外科杂志,2021,35(3):320-323.DOI: 10.3969/j.issn.1671-2722.2021.03.015. [40] GraboyesEM,HornigJD.Evolution of the anterolateral thigh free flap[J].Curr Opin Otolaryngol Head Neck Surg,2017,25(5):416-421.DOI: 10.1097/MOO.0000000000000394. -

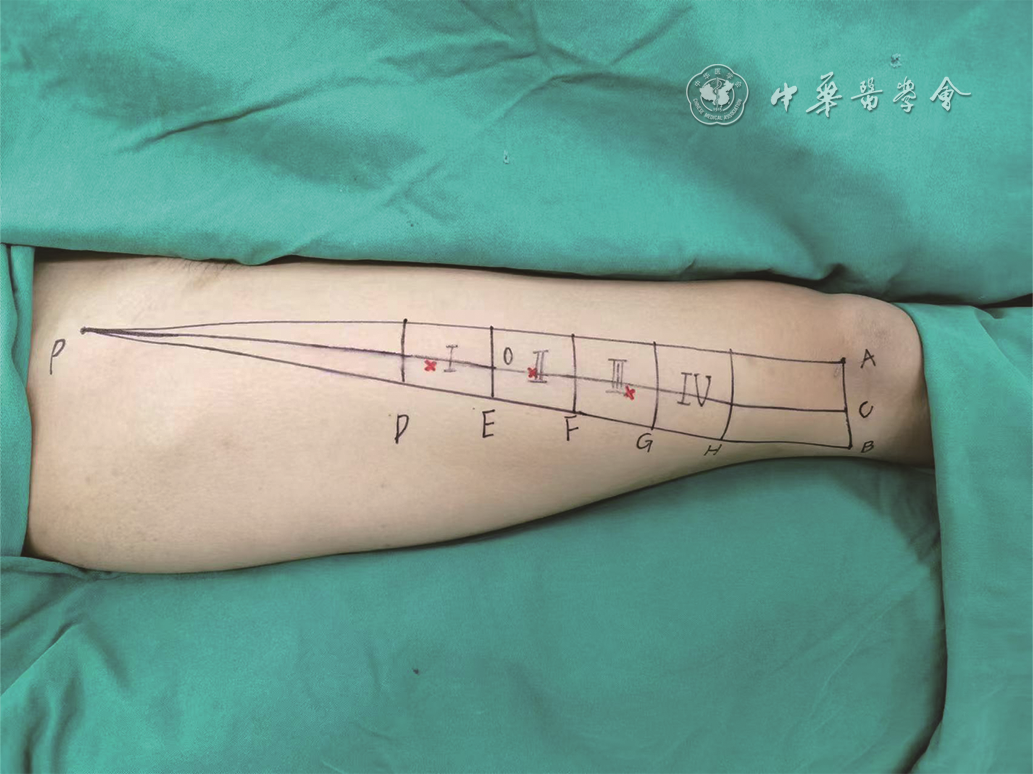
图 1 采用“新型三纵五横法”定位一例左下肢毁损性创面患者的股前外侧嵌合皮瓣穿支
注:P点为髂前上棘,A点为髌骨外上缘,B点为股骨外上髁,C点为A、B点连线的中点,O点为PA线中点;PA线为髂前上棘与髌骨外上缘的连线,PB线为髂前上棘与股骨外上髁的连线,PC线为髂前上棘与C点的连线,E线为过O点垂直于PA线的线,D线为E线向近端平移5 cm所得,F、G、H线分别为E线向远端平移5、10、15 cm所得,PA和PB线分别与D、E、F、G、H线相交,形成4个梯形区域即Ⅰ、Ⅱ、Ⅲ、Ⅳ区;图中各区域内红叉为术前多普勒超声探测到的穿支入皮点

图 2 应用“新型三纵五横法”设计携带阔筋膜的游离股前外侧嵌合皮瓣修复例1患者右手毁损性创面的效果。2A.清创后,见右手掌皮肤软组织缺损,桡侧3指及掌部组织缺失,环指指深屈肌腱部分缺损,小指中远节坏死;2B.采用“新型三纵五横法”设计携带阔筋膜的游离股前外侧嵌合皮瓣;2C.术中切取皮瓣时可见携带的阔筋膜;2D.完整切取的皮瓣;2E、2F.分别为皮瓣游离移植术后即刻右手掌侧、桡侧外观;2G、2H.分别为术后1年随访时右手掌侧、尺侧外观

图 3 应用“新型三纵五横法”设计携带肌瓣的游离股前外侧嵌合皮瓣修复例2患者左下肢毁损性创面。3A.清创后,见左小腿前侧大面积皮肤缺损,胫骨外露伴骨质缺损,深部可见死腔形成;3B.清创后见左小腿内侧大面积皮肤缺损,胫骨外露伴骨质缺损;3C.采用“新型三纵五横法”设计携带肌瓣的游离股前外侧嵌合皮瓣;3D.术中切取皮瓣时可见携带的肌瓣;3E.完整切取的皮瓣;3F.将皮瓣分为两叶,转移覆盖创面后即刻外观;3G、3H.分别为术后1年随访时小腿内侧、外侧皮瓣外观
Table 1. 15例肢体毁损性创面患者各区域内股前外侧嵌合皮瓣穿支情况
区域 数量(条) 来源(条) 穿支入皮点至PC线的垂直距离(cm) 旋股外侧动脉斜支 旋股外侧动脉降支 大腿下段周边血管 Ⅰ区 18 3 15 0 0~0.6 Ⅱ区 17 0 17 0 0~0.8 Ⅲ区 21 0 21 0 0~1.0 Ⅳ区 19 0 12 7 0~1.0 合计 75 3 65 7 — 注:PC线为髂前上棘与髌骨外上缘和股骨外上髁连线中点的连线;“—”表示无此项  下载: 导出CSV
下载: 导出CSV
-
 吴祥奎 3月9日.mp4
吴祥奎 3月9日.mp4

-

 下载:
下载:






计量
- 文章访问数: 673
- HTML全文浏览量: 293
- PDF下载量: 39
- 被引次数: 0
