




Application efficacy of lymph pads in complete decongestive therapy after lymphatico-venous anastomosis combined with liposuction in patients with lower limb lymphedema
-
摘要:
目的 评估淋巴垫在下肢淋巴水肿患者行淋巴管-静脉吻合术(LVA)联合脂肪抽吸术后综合消肿治疗中应用的效果。 方法 该研究为历史对照研究。将2021年6月—2023年1月在西安交通大学附属西安市中心医院烧伤整形美容外科(以下简称本科室)行LVA联合脂肪抽吸术后行综合消肿治疗中未使用淋巴垫的23例患者作为对照组,其中男2例、女21例,年龄(58±10)岁;将2023年2月—2024年1月在本科室行LVA联合脂肪抽吸术后行综合消肿治疗中使用淋巴垫的23例患者作为淋巴垫组,其中男3例、女20例,年龄(59±11)岁。治疗前及治疗6、12个月,测量2组患者患肢足背、踝关节、膝关节上缘周径,记录下肢淋巴水肿功能、残疾与健康问卷(Lymph-ICF-LL)总得分及其中的下肢功能得分。 结果 淋巴垫组患者治疗6、12个月的患肢足背、踝关节、膝关节上缘周径分别为(22.9±1.7)、(26±3)、(44±8)cm和(20.7±1.7)、(25±3)、(42±6)cm,均明显小于对照组的(24.3±2.3)、(29±4)、(49±10)cm和(23.9±2.2)、(29±4)、(48±12)cm(t值分别为2.18、2.29、2.09和5.84、3.92、2.31,P < 0.05),组间均数差值(95%置信区间)分别为1.3(0.1~2.5)、2(0~4)、5(0~10)cm和3.3(2.2~4.5)、4(2~6)、6(1~12)cm。2组患者治疗前及治疗6、12个月的患肢Lymph-ICF-LL总得分比较,差异均无统计学意义(P > 0.05)。淋巴垫组患者治疗6、12个月的患肢Lymph-ICF-LL中下肢功能得分均明显低于对照组(t值分别为2.24、2.44,P < 0.05),组间均数差值(95%置信区间)分别为5(1~9)、5(1~9)cm。 结论 在行LVA联合脂肪抽吸术后行综合消肿治疗中应用淋巴垫可以缩小下肢淋巴水肿患者足背、踝关节、膝关节周径,同时改善患者的下肢功能。 Abstract:Objective To evaluate the application efficacy of lymph pads in complete decongestive therapy after lymphatico-venous anastomosis (LVA) combined with liposuction in patients with lower limb lymphedema. Methods This study was a historical control study. From June 2021 to January 2023, a total of 23 patients who underwent LVA combined with liposuction and then complete decongestive therapy without application of lymph pads at the Department of Burn, Plastic and Cosmetic Surgery of Xi'an Central Hospital of Xi'an Jiaotong University (hereinafter referred to as our department) were included as control group. There were 2 males and 21 females in this group, with the age of 58±10 years. From February 2023 to January 2024, another 23 patients who underwent LVA combined with liposuction and then complete decongestive therapy with additional application of lymph pads at our department were included as lymph pad group. There were 3 males and 20 females in this group, with the age of 59±11 years. Before treatment and at 6 and 12 months of treatment, the circumferences of the dorsum of the foot, ankle joint, and upper edge of the knee joint of the affected limbs were measured, and the total score of lymphedema functioning, disability and health questionnaire for lower limb lymphedema (Lymph-ICF-LL) and score of lower limb function in Lymph-ICF-LL were recorded in patients in the two groups. Results At 6 and 12 months of treatment, the circumferences of the dorsum of the foot, ankle joint, and upper edge of the knee joint in patients in lymph pad group were (22.9±1.7), (26±3), (44±8) cm and (20.7±1.7), (25±3), (42±6) cm, respectively, which were significantly smaller than (24.3±2.3), (29±4), (49±10) cm and (23.9±2.2), (29±4), (48±12) cm in control group (with t values of 2.18, 2.29, 2.09, and 5.84, 3.92, 2.31, respectively, P < 0.05), and the mean differences (95% confidence intervals) between the two groups were 1.3 (0.1 to 2.5), 2 (0 to 4), 5 (0 to 10) cm and 3.3 (2.2 to 4.5), 4 (2 to 6), 6 (1 to 12) cm, respectively. There were no statistically significant differences in the total Lymph-ICF-LL scores of the affected limbs between the two groups of patients before treatment and at 6 and 12 months of treatment (P > 0.05). At 6 and 12 months of treatment, the lower limb function scores in Lymph-ICF-LL of the affected limbs in lymph pad group of patients were significantly lower than those in control group (with t values of 2.24 and 2.44, respectively, P < 0.05), and the mean differences (95% confidence intervals) between the two groups were 5 (1 to 9) and 5 (1 to 9) cm, respectively. Conclusions During complete decongestive therapy following LVA combined with liposuction, the application of lymph pads can significantly reduce the circumference of the dorsum of the foot, ankle joint, and knee joint in patients with lower limb lymphedema, and also improve their lower limb function. 本文亮点对淋巴垫在下肢淋巴水肿患者行淋巴管-静脉吻合术联合脂肪抽吸术后综合消肿治疗中的临床效果进行系统评估,证实淋巴垫治疗能够显著缩小足背、踝关节及膝关节的周径,同时改善患者的下肢功能。 -
参考文献
(41) [1] Hock LA, Nürnberger T, Koban KC, et al. Quality of life in lymphedema patients treated by microsurgical lymphatic vessel transplantation-a long-term follow-up[J]. Life (Basel), 2024, 14(8): 957. DOI: 10.3390/life14080957. [2] Akita S, Yoshida K, Omura M, et al. Noninvasive, objective evaluation of lower extremity lymphedema severity using shear wave elastography: a preliminary study[J]. J Plast Reconstr Aesthet Surg, 2021, 74(12): 3377-3385. DOI: 10.1016/j.bjps.2021.05.013. [3] Tedeschi R. Biomechanical alterations in lower limb lymphedema: implications for walking ability and rehabilitation[J]. Phlebology, 2023, 38(8): 496-502. DOI: 10.1177/02683555231188236. [4] Dessources K, Aviki E, Leitao MM Jr. Lower extremity lymphedema in patients with gynecologic malignancies[J]. Int J Gynecol Cancer, 2020, 30(2): 252-260. DOI: 10.1136/ijgc-2019-001032. [5] Letellier ME, Ibrahim M, Towers A, et al. Incidence of lymphedema related to various cancers[J]. Med Oncol, 2024, 41(10): 245. DOI: 10.1007/s12032-024-02441-2. [6] Wong M, Eaton PK, Zanichelli C, et al. The prevalence of undiagnosed postoperative lower limb lymphedema among gynecological oncology patients[J]. Eur J Surg Oncol, 2022, 48(5): 1167-1172. DOI: 10.1016/j.ejso.2021.12.464. [7] Şahinoğlu E, Ergin G, Karadibak D. The efficacy of change in limb volume on functional mobility, health-related quality of life, social appearance anxiety, and depression in patients with lower extremity lymphedema[J]. Phlebology, 2022, 37(3): 200-205. DOI: 10.1177/02683555211061011. [8] Bobrek K, Nabavizadeh R, Nabavizadeh B, et al. How to care and minimize the sequelae of lower extremity lymphedema [J]. Semin Oncol Nurs, 2022, 38(3): 151270. DOI: 10.1016/j.soncn.2022.151270. [9] Son JH, Min JH, Kim IH, et al. The clinical usefulness of ultrasonographic measurement technique in patients with lower extremity lymphedema[J]. Lymphat Res Biol, 2023, 21(1): 20-27. DOI: 10.1089/lrb.2021.0089. [10] Nuwayhid R, Langer S, von Dercks N. Cost comparison of conservative vs. surgical treatment of chronic lymphedema [J]. Chirurgie (Heidelb), 2025, 96(1): 41-47. DOI: 10.1007/s00104-024-02123-9. [11] Yoshida S, Koshima I, Imai H, et al. Effect of postoperative compression therapy on the success of liposuction in patients with advanced lower limb lymphedema[J]. J Clin Med, 2021, 10(21): 4852. DOI: 10.3390/jcm10214852. [12] Karlsson T, Hoffner M, Ohlin K, et al. Complete reduction of leg lymphedema after liposuction: a 5-year prospective study in 67 patients without recurrence[J]. Plast Reconstr Surg Glob Open, 2023, 11(12): e5429. DOI: 10.1097/GOX.0000000000005429. [13] Torgbenu E, Luckett T, Buhagiar MA, et al. Guidelines relevant to diagnosis, assessment, and management of lymphedema: a systematic review[J]. Adv Wound Care (New Rochelle), 2023, 12(1): 15-27. DOI: 10.1089/wound.2021.0149. [14] Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology[J]. Lymphology, 2020, 53(1): 3-19. [15] Devoogdt N, De Groef A, Hendrickx A, et al. Lymphoedema functioning, disability and health questionnaire for lower limb lymphoedema (Lymph-ICF-LL): reliability and validity [J]. Phys Ther, 2014, 94(5): 705-721. DOI: 10.2522/ptj.20130285. [16] Lu C, Li GL, Deng DH, et al. Transcutaneous electrical acupoint stimulation combined with warm acupuncture for breast cancer related upper limb lymphedema: a retrospective cohort study[J]. Chin J Integr Med, 2023, 29(6): 534-539. DOI: 10.1007/s11655-022-3684-7. [17] Karlsson T, Karlsson M, Ohlin K, et al. Liposuction of breast cancer-related arm lymphedema reduces fat and muscle hypertrophy[J]. Lymphat Res Biol, 2022, 20(1): 53-63. DOI: 10.1089/lrb.2020.0120. [18] Onoda S, Satake T, Hamada E. Super-microsurgery technique for lymphaticovenular anastomosis[J]. J Vasc Surg Venous Lymphat Disord, 2023, 11(1): 177-181. DOI: 10.1016/j.jvsv.2022.08.008. [19] Cheng MH, Tee R, Chen C, et al. Simultaneous ipsilateral vascularized lymph node transplantation and contralateral lymphovenous anastomosis in bilateral extremity lymphedema with different severities[J]. Ann Surg Oncol, 2020, 27(13): 5267-5276. DOI: 10.1245/s10434-020-08720-2. [20] 陈佳佳, 高敏哲, 汪立, 等. 妇科相关肿瘤术后下肢淋巴水肿合并会阴部水肿的综合治疗初探[J]. 组织工程与重建外科杂志, 2022, 18(3): 242-246. DOI: 10.3969/j.issn.1673-0364.2022.03.008. [21] Dionyssiou D, Sarafis A, Tsimponis A, et al. Long-term outcomes of lymph node transfer in secondary lymphedema and its correlation with flap characteristics[J]. Cancers (Basel), 2021, 13(24): 6198. DOI: 10.3390/cancers13246198. [22] Shimbo K, Kawamoto H, Koshima I. Conservative treatment versus lymphaticovenular anastomosis for early-stage lower extremity lymphedema[J]. J Vasc Surg Venous Lymphat Disord, 2023, 11(6): 1231-1240. DOI: 10.1016/j.jvsv.2023.06.013. [23] Mihara M, Hara H, Furniss D, et al. Lymphaticovenular anastomosis to prevent cellulitis associated with lymphoedema[J]. Br J Surg, 2014, 101(11): 1391-1396. DOI: 10.1002/bjs.9588. [24] Caretto AA, Stefanizzi G, Garganese G, et al. Treatment of early-stage gynecological cancer-related lower limb lymphedema by lymphaticovenular anastomosis-the triple incision approach[J]. Medicina (Kaunas), 2022, 58(5): 631. DOI: 10.3390/medicina58050631. [25] 刘长瑞, 王鹤君, 王营营, 等. 超显微外科淋巴管静脉吻合术在肢体淋巴水肿中的应用[J]. 组织工程与重建外科杂志, 2025, 21(1): 77-82. DOI: 10.3969/j.issn.1673-0364.2025.01.014. [26] Karlsson T, Hoffner M, Brorson H. Liposuction and controlled compression therapy reduce the erysipelas incidence in primary and secondary lymphedema[J]. Plast Reconstr Surg Glob Open, 2022, 10(5): e4314. DOI: 10.1097/GOX.0000000000004314. [27] Hoffner M, Peterson P, Månsson S, et al. Lymphedema leads to fat deposition in muscle and decreased muscle/water volume after liposuction: a magnetic resonance imaging study[J]. Lymphat Res Biol, 2018, 16(2): 174-181. DOI: 10.1089/lrb.2017.0042. [28] 郝昆, 孙宇光, 王仁贵, 等. 抽吸减容术治疗乳腺癌术后上肢淋巴水肿[J]. 组织工程与重建外科杂志, 2024, 20(1): 69-74, 82. DOI: 10.3969/j.issn.1673-0364.2024.01.005. [29] Brazio PS, Nguyen DH. Combined liposuction and physiologic treatment achieves durable limb volume normalization in class Ⅱ-Ⅲ lymphedema: a treatment algorithm to optimize outcomes[J]. Ann Plast Surg, 2021, 86(5S Suppl 3): S384-389. DOI: 10.1097/SAP.0000000000002695. [30] Gabriele G, Nigri A, Chisci G, et al. Combination of supramicrosurgical lymphatico-venular anastomosis (sLVA) and lymph-sparing liposuction in treating cancer-related lymphedema: rationale for a regional one-stage approach[J]. J Clin Med, 2024, 13(10): 2872. DOI: 10.3390/jcm13102872. [31] Zhou X, Ma G, Qi X, et al. Application of complete decongestive therapy after lymphaticovenular anastomosis of the lower limb combined with liposuction-a retrospective study research[J]. Phlebology, 2024, 39(1): 49-57. DOI: 10.1177/02683555231209056. [32] Brémond-Gignac D, Copin H, Kohler C, et al. The lateral inframalleolar fat pad: a poorly recognized anatomical structure[J]. Surg Radiol Anat, 2001, 23(5): 325-329. DOI: 10.1007/s00276-001-0325-2. [33] Yao B, Samuel LT, Acuña AJ, et al. Infrapatellar fat pad resection or preservation during total knee arthroplasty: a systematic review[J]. J Knee Surg, 2021, 34(4): 415-421. DOI: 10.1055/s-0039-1696692. [34] Arai KY, Sugimoto M, Ito K, et al. Repeated folding stress-induced morphological changes in the dermal equivalent[J]. Skin Res Technol, 2014, 20(4): 399-408. DOI: 10.1111/srt.12131. [35] Lee SO, Kim IK. Molecular pathophysiology of secondary lymphedema[J]. Front Cell Dev Biol, 2024, 12: 1363811. DOI: 10.3389/fcell.2024.1363811. [36] Ren Y, Kebede MA, Ogunleye AA, et al. Burden of lymphedema in long-term breast cancer survivors by race and age[J]. Cancer, 2022, 128(23): 4119-4128. DOI: 10.1002/cncr.34489. [37] Partsch H, Mosti G. Thigh compression[J]. Phlebology, 2008, 23(6): 252-258. DOI: 10.1258/phleb.2008.008053. [38] O'Brien JG, Chennubhotla SA, Chennubhotla RV. Treatment of edema[J]. Am Fam Physician, 2005, 71(11): 2111-2117. [39] Devitt M, Ramanan D, Armitstead J, et al. Usability evaluation of a novel compact pneumatic compression device for the treatment of lymphoedema: pilot study[J]. Phlebology, 2022, 37(8): 564-571. DOI: 10.1177/02683555221096298. [40] Soran A, Toktas O, Grassi A, et al. Adding pneumatic compression therapy in lower extremity lymphedema increases compliance of treatment, while decreasing the infection rate[J]. Lymphat Res Biol, 2022, 20(3): 315-318. DOI: 10.1089/lrb.2020.0086. [41] Hobday A. Use of compression therapy in patients with lymphoedema[J]. Nurs Stand, 2016, 30(27): 50-58; quiz 60. DOI: 10.7748/ns.30.27.50.s46. -

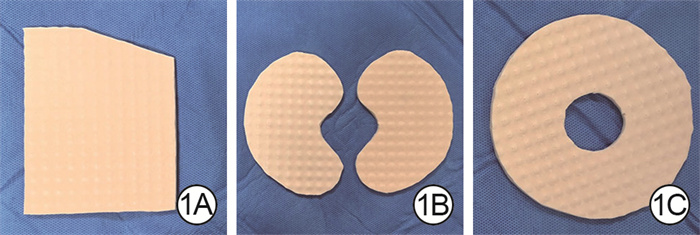
图 1 足背、踝关节及膝关节淋巴垫。1A.足背淋巴垫;1B.踝关节淋巴垫;1C.膝关节淋巴垫
Figure 1. Lymph pads for the dorsum of the foot, ankle joint, and knee joint

图 2 右下肢淋巴水肿患者行淋巴管-静脉吻合术联合脂肪抽吸术后行综合消肿治疗及淋巴垫治疗的效果。2A.治疗前,右下肢足背、踝关节、膝关节水肿明显;2B.治疗6个月,右下肢足背、踝关节、膝关节水肿明显减轻;2C.治疗12个月,右下肢足背、踝关节、膝关节水肿与健侧差别不大
Figure 2. Effects of complete decongestive therapy and lymph pad treatment after lymphatic-venous anastomosis combined with liposuction in a patient with lymphedema in the right lower limb
表 1 2组行LVA联合脂肪抽吸术后行综合消肿治疗的下肢淋巴水肿患者一般资料比较
Table 1. Comparison of general data in two groups of patients with lower limb lymphedema undergoing complete decongestive therapy after LVA combined with liposuction
组别 例数 性别(例) 年龄(岁,x±s) 体重指数(kg/m2,x±s) 淋巴水肿时间(月,x±s) 淋巴水肿分期(例) 淋巴水肿部位(例) 男 女 Ⅰ期 Ⅱ期 Ⅲ期 左下肢 右下肢 双下肢 淋巴垫组 23 3 20 59±11 27±4 311±80 2 10 11 9 7 7 对照组 23 2 21 58±10 26±3 335±56 1 8 14 10 6 7 统计量值 — t=0.37 t=0.67 t=-1.16 χ2=1.01 χ2=0.13 P值 > 0.999 0.714 0.504 0.253 0.650 0.937 组别 例数 肿瘤时间(月,x±s) 患病类型(例) 放射治疗史(例) 化学治疗史(例) 基础疾病(例) 子宫内膜癌 宫颈癌 其他 有 无 有 无 有 无 淋巴垫组 23 430±124 12 9 2 17 6 19 4 13 10 对照组 23 461±169 9 10 4 15 8 17 6 17 6 统计量值 t=-0.72 χ2=1.15 χ2=0.41 χ2=0.51 χ2=1.53 P值 0.475 0.563 0.522 0.475 0.216 注:淋巴垫组患者在对照组患者综合消肿治疗的基础上,增加淋巴垫治疗;LVA为淋巴管-静脉吻合术;淋巴水肿分期按照国际淋巴学会标准[14];“—”表示无此项;其他患病类型包括卵巢癌、外伤及无明确病因的淋巴水肿  下载: 导出CSV
下载: 导出CSV
表 2 2组行LVA联合脂肪抽吸术后行综合消肿治疗的下肢淋巴水肿患者不同时间点足背和踝关节及膝关节上缘周径的比较(cm,x±s)
Table 2. Comparison of the circumferences of the dorsum of the foot, ankle joint, and upper edge of knee joint at different time points in two groups of patients with lower limb lymphedema undergoing complete decongestive therapy after LVA combined with liposuction
组别 例数 治疗前 治疗6个月 治疗12个月 足背 踝关节 膝关节上缘 足背 踝关节 膝关节上缘 足背 踝关节 膝关节上缘 淋巴垫组 23 25.2±1.6 26±3 50±9 22.9±1.7 26±3 44±8 20.7±1.7 25±3 42±6 对照组 23 24.6±2.4 29±4 50±10 24.3±2.3 29±4 49±10 23.9±2.2 29±4 48±12 均数差值(95%置信区间) -0.6(-1.8~0.6) 0(-2~2) 0(-5~6) 1.3(0.1~2.5) 2(0~4) 5(0~10) 3.3(2.2~4.5) 4(2~6) 6(1~12) t值 0.98 0.08 0.05 2.18 2.29 2.09 5.84 3.92 2.31 P值 0.332 0.935 0.961 0.035 0.027 0.043 < 0.001 < 0.001 0.025 注:淋巴垫组患者在对照组患者综合消肿治疗的基础上,增加淋巴垫治疗;LVA为淋巴管-静脉吻合术;足背、踝关节、膝关节上缘周径时间因素主效应,F值分别为119.43、78.71、5.32,P值分别为 < 0.001、 < 0.001、0.009;处理因素主效应,F值分别为5.72、4.43、5.39,P值分别为 < 0.001、0.041、0.025;两者交互作用,F值分别为59.47、51.97、2.49,P值分别为 < 0.001、 < 0.001、0.090
下载: 导出CSV
表 3 2组LVA联合脂肪抽吸术后行综合消肿治疗的下肢淋巴水肿患者不同时间点Lymph-ICF-LL总得分比较(分,x±s)
Table 3. Comparison of total Lymph-ICF-LL scores at different time points in two groups of patients with lower limb lymphedema undergoing complete decongestive therapy after LVA combined with liposuction
组别 例数 治疗前 治疗6个月 治疗12个月 淋巴垫组 23 41±14 39±14 37±10 对照组 23 41±15 40±14 39±11 均数差值(95%置信区间) 0(-9~8) 1(-7~9) 1(-5~8) t值 0.09 0.17 0.45 P值 0.926 0.864 0.655 注:淋巴垫组患者在对照组患者综合消肿治疗的基础上,增加淋巴垫治疗;LVA为淋巴管-静脉吻合术,Lymph-ICF-LL为下肢淋巴水肿功能、残疾与健康问卷;时间因素主效应,F=2.59,P=0.087;处理因素主效应,F=0.04,P=0.850;两者交互作用,F=0.33,P=0.723
下载: 导出CSV
表 4 2组行LVA联合脂肪抽吸术后行综合消肿治疗的下肢淋巴水肿患者不同时间点下肢功能得分比较(分,x±s)
Table 4. Comparison of lower limb function scores at different time points in two groups of patients with lower limb lymphedema undergoing complete decongestive therapy after LVA combined with liposuction
组别 例数 治疗前 治疗6个月 治疗12个月 淋巴垫组 23 43±7 36±7 35±7 对照组 23 42±8 40±6 40±7 均数差值(95%置信区间) -1(-5~5) 5(1~9) 5(1~9) t值 0.12 2.24 2.44 P值 0.860 0.030 0.019 注:淋巴垫组患者在对照组患者综合消肿治疗的基础上,增加淋巴垫治疗;LVA为淋巴管-静脉吻合术;时间因素主效应,F=12.48,P < 0.001;处理因素主效应,F=2.51,P=0.120;两者交互作用,F=2.61,P=0.086
下载: 导出CSV
-
 杨晨 5月22日.mp4
杨晨 5月22日.mp4

-

 下载:
下载:




计量
- 文章访问数: 1749
- HTML全文浏览量: 257
- PDF下载量: 18
- 被引次数: 0
