




Clinical efficacy of vascularized lymph node transfer combined with lymphatico-venous anastomosis in treating unilateral upper limb lymphedema after radical mastectomy for breast cancer
-
摘要:
目的 研究血管化淋巴结移植(VLNT)联合淋巴静脉吻合术(LVA)治疗乳腺癌根治术后单侧上肢淋巴水肿的临床效果。 方法 该研究为回顾性队列研究。2021年4月—2024年1月,遵义医科大学附属医院收治40例符合入选标准的乳腺癌根治术后单侧上肢淋巴水肿女性患者,年龄35~75岁。根据患者采用的治疗方法将其分为仅行LVA治疗的LVA组(18例)和行VLNT联合LVA治疗的VLNT+LVA组(22例)。治疗前及治疗后3、6、12个月测量2组患者患肢体积,计算治疗前与治疗后各时间点患肢体积的差值(即治疗后各时间点患肢体积差),采用协方差分析控制基线资料等混杂因素对治疗后各时间点患肢体积差的影响。治疗前与治疗后12个月,采用淋巴水肿生活质量问卷对2组患者进行生活质量评定。随访期间观察2组患者感染性并发症发生情况,治疗后12个月对VLNT+LVA组患者行超声检查或放射性核素显像评估淋巴结存活情况。 结果 VLNT+LVA组患者治疗后6、12个月患肢体积差分别为(521±193)、(694±355)cm3,显著大于LVA组的(377±92)、(452±229)cm3(均数差值分别为144、242 cm3,95%置信区间分别为44~244、46~438 cm3,t值分别为2.90、2.49,P值均 < 0.05)。协方差分析显示,校正基线资料后,VLNT+LVA组患者治疗后6、12个月患肢体积差均显著大于LVA组(F值分别为6.52、5.26,P < 0.05)。LVA组、VLNT+LVA组患者治疗后12个月生活质量评分分别为8(4,9)、7(4,9)分,显著高于治疗前的6(3,7)、5(2,7)分(Z值分别为-2.97、-3.46,P值均 < 0.05);但2组患者治疗后12个月生活质量评分比较,差异无统计学意义(P > 0.05)。2组患者在治疗后12个月随访期间均未发生丹毒、蜂窝组织炎及淋巴管炎等感染性并发症;治疗后12个月,VLNT+LVA组患者移植淋巴结存活可。 结论 相较于单纯LVA,VLNT联合LVA也可改善乳腺癌根治术后单侧上肢淋巴水肿患者患肢体积和生活质量,且中远期疗效更佳,值得临床推广。 Abstract:Objective To investigate the clinical efficacy of vascularized lymph node transfer (VLNT) combined with lymphatico-venous anastomosis (LVA) in treating unilateral upper limb lymphedema after radical mastectomy for breast cancer. Methods This study was a retrospective cohort study. Forty female patients aged 35-75 years with unilateral upper limb lymphedema after radical mastectomy for breast cancer who met the inclusion criteria were admitted to the Affiliated Hospital of Zunyi Medical University from April 2021 to January 2024. Based on the treatment method, patients were divided into LVA group (18 cases) who underwent LVA treatment only and VLNT+LVA group (22 cases) who underwent VLNT combined with LVA treatment. The volumes of the affected limbs in both groups of patients were measured before treatment and 3, 6, and 12 months after treatment. The differences in affected limb volumes at each time point before and after treatment (i.e., the volume differences of affected limbs at each time point after treatment) were calculated. Analysis of covariance (ANCOVA) was used to control the influence of confounding factors such as baseline data on the volume differences of affected limbs at each time point after treatment. The quality of life was assessed using the Lymphedema Quality of Life Questionnaire before treatment and 12 months after treatment. During the follow-up period, the occurrence of infectious complications in patients of both groups were monitored. Ultrasonography or radionuclide imaging was performed 12 months after treatment to evaluate the survival of lymph nodes in patients in VLNT+LVA group. Results The volume differences of affected limbs in patients in VLNT+LVA group 6 and 12 months after treatment were (521±193) and (694±355) cm3, respectively, which were significantly greater than (377±92) and (452±229) cm3 in LVA group (with mean differences of 144 and 242 cm3, respectively, 95% confidence intervals of 44-244 and 46-438 cm3, respectively, t values of 2.90 and 2.49, respectively, both P values < 0.05). ANCOVA showed that after adjusting for baseline data, the volume difference of affected limb of patients in VLNT+LVA group 6 and 12 months after treatment were significantly greater than those in LVA group (with F values of 6.52 and 5.26, respectively, P < 0.05). Twelve months after treatment, the quality of life scores of patients in LVA group and VLNT+LVA group were 8 (4, 9) and 7 (4, 9), respectively, which were significantly higher than 6 (3, 7) and 5 (2, 7) before treatment (with Z values of -2.97 and -3.46, respectively, both P values < 0.05). However, there was no statistically significant difference in quality of life score of patients between the two groups 12 months after treatment (P > 0.05). During the 12-month post-treatment follow-up, patients in neither group developed infectious complications such as erysipelas, cellulitis, or lymphangitis. Transplanted lymph nodes of patients survived well in VLNT+LVA group 12 months after treatment. Conclusions Compared with LVA alone, VLNT combined with LVA also improves the volume of affected limb and the quality of life of patients with unilateral upper limb lymphedema following radical mastectomy for breast cancer with better mid- and long-term efficacy, which is worthy of clinical promotion. 本文亮点(1) 血管化淋巴结移植(VLNT)与淋巴静脉吻合术(LVA)联合应用在乳腺癌根治术后单侧上肢淋巴水肿治疗中具有互补效应,中远期疗效优于单纯LVA,突破单纯LVA疗效衰减瓶颈。(2) 应用吲哚菁绿-亚甲蓝双向示踪技术定位下肢淋巴结供区,减少供区医源性淋巴水肿发生。(3) 提出肘部挤压作用可加强“淋巴结泵”理论,为淋巴引流优化提供进一步的机制方面的见解。 -
参考文献
(40) [1] Jørgensen MG, Toyserkani NM, Hansen FG, et al. The impact of lymphedema on health-related quality of life up to 10 years after breast cancer treatment[J]. NPJ Breast Cancer, 2021, 7(1): 70. DOI: 10.1038/s41523-021-00276-y. [2] 宋达疆, 李赞, 章一新, 等. 带蒂腹直肌肌皮瓣联合游离腹壁下动脉穿支皮瓣及携带髂腹股沟淋巴组织瓣行乳腺癌根治术后乳房再造及上肢淋巴水肿治疗的效果[J]. 中华烧伤杂志, 2020, 36(4): 297-303. DOI: 10.3760/cma.j.cn501120-20190117-00011. [3] Huang J, Li J, Li Y, et al. Bibliometric analysis of breast cancer-related lymphedema research trends over the last 2 decades[J]. Front Oncol, 2024, 14: 1360899. DOI: 10.3389/fonc.2024.1360899. [4] Shang R, Zhou J, Pan T, et al. Bibliometric and visual analysis of breast cancer-related lymphedema: knowledge structure, research status, and future trends[J]. Medicine (Baltimore), 2025, 104(7): e41510. DOI: 10.1097/MD.0000000000041510. [5] Gillespie TC, Sayegh HE, Brunelle CL, et al. Breast cancer-related lymphedema: risk factors, precautionary measures, and treatments[J]. Gland Surg, 2018, 7(4): 379-403. DOI: 10.21037/gs.2017.11.04. [6] Gilchrist L, Levenhagen K, Davies CC, et al. Effectiveness of complete decongestive therapy for upper extremity breast cancer-related lymphedema: a review of systematic reviews[J]. Med Oncol, 2024, 41(11): 297. DOI: 10.1007/s12032-024-02421-6. [7] Thompson B, Gaitatzis K, Janse de Jonge X, et al. Manual lymphatic drainage treatment for lymphedema: a systematic review of the literature[J]. J Cancer Surviv, 2021, 15(2): 244-258. DOI: 10.1007/s11764-020-00928-1. [8] AlJindan FK, Lin CY, Cheng MH. Comparison of outcomes between side-to-end and end-to-end lymphovenous anastomoses for early-grade extremity lymphedema[J]. Plast Reconstr Surg, 2019, 144(2): 486-496. DOI: 10.1097/PRS.0000000000005870. [9] Seidenstuecker K, Fertsch S, Ghazaleh AA, et al. Improving quality of life after breast cancer: a comparison of two microsurgical treatment options for breast cancer-related lymphedema (BCRL) [J]. Clin Exp Med, 2024, 24(1): 82. DOI: 10.1007/s10238-024-01344-w. [10] Drobot D, Zeltzer AA. Surgical treatment of breast cancer related lymphedema-the combined approach: a literature review[J]. Gland Surg, 2023, 12(12): 1746-1759. DOI: 10.21037/gs-23-247. [11] Sun F, Hall A, Tighe MP, et al. Perometry versus simulated circumferential tape measurement for the detection of breast cancer-related lymphedema[J]. Breast Cancer Res Treat, 2018, 172(1): 83-91. DOI: 10.1007/s10549-018-4902-z. [12] Lo Torto F, Kaciulyte J, Di Meglio F, et al. Orthotopic vascularized lymph node transfer in breast cancer-related lymphedema treatment: functional and life quality outcomes[J]. Microsurgery, 2024, 44(2): e31147. DOI: 10.1002/micr.31147. [13] Lim P, Li H, Neoh D, et al. Health-related quality of life measurement tools for lymphedema: a review of the literature[J]. Plast Reconstr Surg Glob Open, 2022, 10(4): e4276. DOI: 10.1097/GOX.0000000000004276. [14] Wolfs JAGN, de Joode LGEH, van der Hulst RRWJ, et al. Correlation between patency and clinical improvement after lymphaticovenous anastomosis (LVA) in breast cancer-related lymphedema: 12-month follow-up[J]. Breast Cancer Res Treat, 2020, 179(1): 131-138. DOI: 10.1007/s10549-019-05450-2. [15] Qiu SS, Pruimboom THJP, Cornelissen A, et al. Outcomes following lymphaticovenous anastomosis (LVA) for 100 cases of lymphedema: results over 24-months follow-up[J]. Breast Cancer Res Treat, 2020, 184(1): 173-183. DOI: 10.1007/s10549-020-05839-4. [16] Morishima S, Tsukuura R. Comments on "long-term patency of multiple lymphatic-venous anastomoses in cancer-related lymphedema: a single-center observational study"[J]. Microsurgery, 2023, 43(2): 199. DOI: 10.1002/micr.30998. [17] Boccardo F, Santori G, Villa G, et al. Long-term patency of multiple lymphatic-venous anastomoses in cancer-related lymphedema: a single center observational study[J]. Microsurgery, 2022, 42(7): 668-676. DOI: 10.1002/micr.30944. [18] Winters H, Tielemans HJP, Verhulst AC, et al. The long-term patency of lymphaticovenular anastomosis in breast cancer-related lymphedema[J]. Ann Plast Surg, 2019, 82(2): 196-200. DOI: 10.1097/SAP.0000000000001674. [19] Yoshida S, Koshima I, Imai H, et al. Modified intraoperative distal compression method for lymphaticovenous anastomosis with high success and a low venous reflux rates[J]. J Plast Reconstr Aesthet Surg, 2021, 74(9): 2050-2058. DOI: 10.1016/j.bjps.2020.12.103. [20] Yang JC. Lymphatic-based lymphosome: a novel hypothesis with clinical implication for supermicrosurgical lymphaticovenous anastomosis[J]. Plast Reconstr Surg Glob Open, 2023, 11(12): e5503. DOI: 10.1097/GOX.0000000000005503. [21] Suami H. Anatomical theories of the pathophysiology of cancer-related lymphoedema[J]. Cancers (Basel), 2020, 12(5): 1338. DOI: 10.3390/cancers12051338. [22] Suami H, Scaglioni MF. Anatomy of the lymphatic system and the lymphosome concept with reference to lymphedema[J]. Semin Plast Surg, 2018, 32(1): 5-11. DOI: 10.1055/s-0038-1635118. [23] Onoda S, Satake T, Kinoshita M. Relationship between lymphaticovenular anastomosis outcomes and the number and types of anastomoses[J]. J Surg Res, 2022, 269: 103-109. DOI: 10.1016/j.jss.2021.08.012. [24] Schaverien MV, Badash I, Patel KM, et al. Vascularized lymph node transfer for lymphedema[J]. Semin Plast Surg, 2018, 32(1): 28-35. DOI: 10.1055/s-0038-1632401. [25] Ngo QD, Munot S, Mackie H, et al. Vascularized lymph node transfer for patients with breast cancer-related lymphedema can potentially reduce the burden of ongoing conservative management[J]. Lymphat Res Biol, 2020, 18(4): 357-364. DOI: 10.1089/lrb.2019.0048. [26] Donahue PMC, MacKenzie A, Filipovic A, et al. Advances in the prevention and treatment of breast cancer-related lymphedema[J]. Breast Cancer Res Treat, 2023, 200(1): 1-14. DOI: 10.1007/s10549-023-06947-7. [27] Subramanyam P, Janarthanan R, Palaniswamy SS. Early demonstration of spontaneous perinodal lymphangiogenesis by lymphoscintigraphy after vascularized lymph node transplantation - a pilot study[J]. Indian J Nucl Med, 2022, 37(1): 1-6. DOI: 10.4103/ijnm.ijnm_123_21. [28] Kusajima EG, Yamamoto Y, Ishikawa K, et al. Sentinel node restoration by vascularized lymph node transfer in mice[J]. Microsurgery, 2024, 44(1): e30981. DOI: 10.1002/micr.30981. [29] Kwiecien GJ, Gharb BB, Tadisina KK, et al. Quantity of lymph nodes in the vascularized lymph node transfer influences its lymphaticovenous drainage[J]. J Reconstr Microsurg, 2018, 34(1): 41-46. DOI: 10.1055/s-0037-1606320. [30] Ward J, King I, Monroy-Inglesias M, et al. Limb volume reduction and infection outcomes following vascularized lymph node transfer for cancer treatment-related lymphoedema: a systematic review and meta-analysis[J]. Eur J Surg Oncol, 2022, 48(2): e147. DOI: 10.1016/j.ejso.2021.12.286. [31] Cheng MH, Chen SC, Henry SL, et al. Vascularized groin lymph node flap transfer for postmastectomy upper limb lymphedema: flap anatomy, recipient sites, and outcomes [J]. Plast Reconstr Surg, 2013, 131(6): 1286-1298. DOI: 10.1097/PRS.0b013e31828bd3b3. [32] Wei M, Wang L, Wu X, et al. Synchronous supraclavicular vascularized lymph node transfer and liposuction for gynecological cancer-related lower extremity lymphedema: a clinical comparative analysis of three different procedures[J]. J Vasc Surg Venous Lymphat Disord, 2024, 12(5): 101905. DOI: 10.1016/j.jvsv.2024.101905. [33] Gould DJ, Mehrara BJ, Neligan P, et al. Lymph node transplantation for the treatment of lymphedema[J]. J Surg Oncol, 2018, 118(5): 736-742. DOI: 10.1002/jso.25180. [34] Scaglioni MF, Arvanitakis M, Chen YC, et al. Comprehensive review of vascularized lymph node transfers for lymphedema: outcomes and complications[J]. Microsurgery, 2018, 38(2): 222-229. DOI: 10.1002/micr.30079. [35] Di Taranto G, Bolletta A, Chen SH, et al. A prospective study on combined lymphedema surgery: gastroepiploic vascularized lymph nodes transfer and lymphaticovenous anastomosis followed by suction lipectomy[J]. Microsurgery, 2021, 41(1): 34-43. DOI: 10.1002/micr.30641. [36] Yang JC, Wu SC, Hayashi A, et al. Lower limb lymphedema patients can still benefit from supermicrosurgical lymphaticovenous anastomosis (LVA) after vascularized lymph node flap transfer (VLNT) as delayed lymphatic reconstruction-a retrospective cohort study[J]. J Clin Med, 2021, 10(14): 3121. DOI: 10.3390/jcm10143121. [37] Garza RM, Beederman M, Chang DW. Physical and functional outcomes of simultaneous vascularized lymph node transplant and lymphovenous bypass in the treatment of lymphedema[J]. Plast Reconstr Surg, 2022, 150(1): 169-180. DOI: 10.1097/PRS.0000000000009247. [38] Kappos EA, Fabi A, Halbeisen FS, et al. Vascularized lymph node transfer (VLNT) versus lymphaticovenous anastomosis (LVA) for chronic breast cancer-related lymphedema (BCRL): a retrospective cohort study of effectiveness over time[J]. Breast Cancer Res Treat, 2025, 210(2): 319-327. DOI: 10.1007/s10549-024-07567-5. [39] Elia R, Chen HC, Cazzato G, et al. Evaluation of modulation of immunity by lymph node transfer: a preliminary histological evidence in lymphedema patients[J]. Microsurgery, 2024, 44(1): e31123. DOI: 10.1002/micr.31123. [40] 邓呈亮, 陈君哲, 章一新. 继发性肢体淋巴水肿的外科整合治疗[J/CD]. 中华损伤与修复杂志(电子版), 2024, 19(3): 185-191. DOI: 10.3877/cma.j.issn.1673-9450.2024.03.001 . -

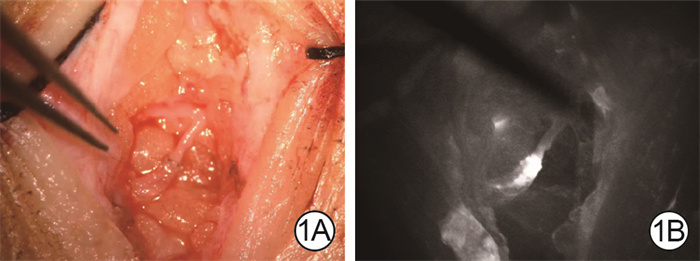
图 1 乳腺癌根治术后右上肢淋巴水肿患者淋巴静脉吻合术中情况。1A.淋巴管与邻近静脉吻合后情况机器人手术显微镜×25;1B.吲哚菁绿近红外淋巴成像验证淋巴管与邻近静脉吻合口处通畅
Figure 1. Intraoperative details of lymphatico-venous anastomosis in patients with right upper limb lymphedema following radical mastectomy for breast cancer

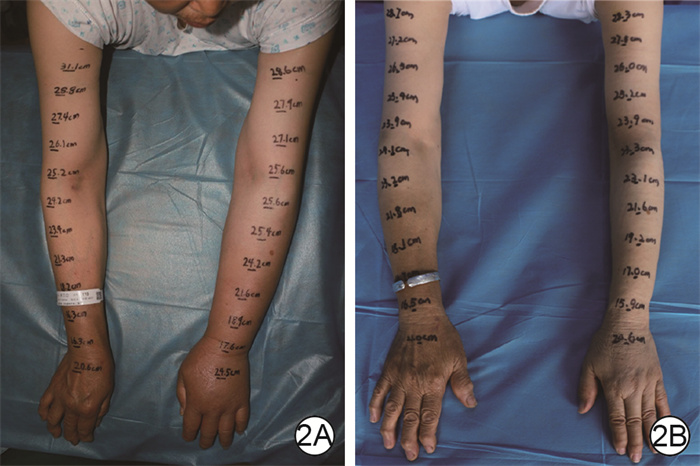
图 2 例1乳腺癌根治术后左上肢淋巴水肿患者行淋巴静脉吻合术治疗前后患肢对比。2A.治疗前患肢肿胀明显;2B.治疗后12个月患肢肿胀明显改善
Figure 2. Comparison of the affected limb before and after lymphatico-venous anastomosis treatment in case 1 with left upper limb lymphedema following radical mastectomy for breast cancer

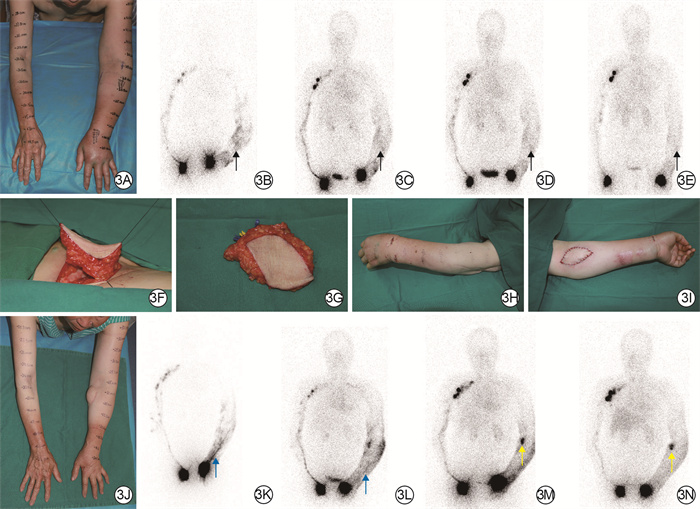
图 3 血管化淋巴结移植联合淋巴静脉吻合术治疗例2患者乳腺癌根治术后左上肢淋巴水肿的效果。3A.治疗前患肢肿胀明显;3B、3C、3D、3E.分别为治疗前行淋巴放射性核素显像后10 min、1 h、3 h、6 h情况,左上肢淋巴管未见明显显影,提示左上肢淋巴回流障碍(黑色箭头所示);3F、3G.分别为腹股沟淋巴结皮瓣切取中、切取后;3H.淋巴静脉吻合术后即刻外观;3I.血管化淋巴结皮瓣移植后即刻外观;3J.治疗后12个月患肢肿胀改善,手背皮肤皱褶出现;3K、3L、3M、3N.分别为治疗后12个月行淋巴放射性核素显像后10 min、1 h、3 h、6 h情况,左上肢淋巴管显影(蓝色箭头所示),肘部移植淋巴结显影(黄色箭头所示),提示淋巴回流较图 3B、3C、3D、3E明显改善,移植淋巴结存活
Figure 3. Effects of vascularized lymph node transfer combined with lymphatico-venous anastomosis in treating left upper limb lymphedema following radical mastectomy for breast cancer in case 2
表 1 2组乳腺癌根治术后单侧上肢淋巴水肿患者的一般资料比较
Table 1. Comparison of general data between two groups of patients with unilateral upper limb lymphedema after radical mastectomy for breast cancer
组别 例数 年龄(岁,x±s) 体重指数(kg/m2,x±s) 入院前水肿持续时间(月,x±s) 水肿所在部位(例) 治疗前CDT持续时间[月,M(min,max)] 左上肢 右上肢 LVA组 18 55±12 26.0±2.0 10±4 8 10 0(0,6) VLNT+LVA组 22 58±10 26.7±2.6 13±6 10 12 0(0,6) 统计量值 t=-0.97 t=-1.01 t=-1.49 — Z=-0.62 P值 0.340 0.318 0.144 0.949 0.535 注:淋巴静脉吻合术(LVA)组患者仅行LVA治疗,血管化淋巴结移植(VLNT)+LVA组患者行VLNT联合LVA治疗;CDT为综合消肿疗法;“—”表示无此项  下载: 导出CSV
下载: 导出CSV
表 2 2组乳腺癌根治术后单侧上肢淋巴水肿患者治疗前后患肢体积变化比较(cm3,x±s)
Table 2. Comparison of pre-treatment and post-treatment affected limb volume changes between two groups of patients with unilateral upper limb lymphedema after radical mastectomy for breast cancer
组别 例数 治疗前患肢体积 治疗后3个月患肢体积差 治疗后6个月患肢体积差 治疗后12个月患肢体积差 LVA组 18 2 465±429 327±81 377±92 452±229 VLNT+LVA组 22 2 559±385 310±72 521±193 694±355 均数差值(95%置信区间) 94(-167~355) -17(-66~32) 144(44~244) 242(46~438) t值 0.73 -0.72 2.90 2.49 P值 0.467 0.478 0.006 0.017 注:淋巴静脉吻合术(LVA)组患者仅行LVA治疗,血管化淋巴结移植(VLNT)+LVA组患者行VLNT联合LVA治疗;处理因素主效应,F=5.46,P=0.025;时间因素主效应,F=30.96,P < 0.001;两者交互作用,F=8.18,P=0.004;治疗后3、6、12个月患肢体积差分别为治疗前与治疗后3、6、12个月患肢体积的差值
下载: 导出CSV
表 3 2组乳腺癌根治术后单侧上肢淋巴水肿患者各时间点患肢体积差的协方差分析结果(cm3,$ \bar{x} \pm s_{\bar{x}}$)
Table 3. Results of analysis of covariance for affected limb volume reductions at various time points between two groups of patients with unilateral upper limb lymphedema after radical mastectomy for breast cancer
组别 例数 治疗后3个月 治疗后6个月 治疗后12个月 LVA组 18 329±19 381±38 454±74 VLNT+LVA组 22 308±17 518±34 692±66 均数差值(95%置信区间) -21(-75~35) 137(28~245) 238(27~448) F值 0.57 6.52 5.26 P值 0.454 0.015 0.028 注:淋巴静脉吻合术(LVA)组患者仅行LVA治疗,血管化淋巴结移植(VLNT)+LVA组患者行VLNT联合LVA治疗;治疗后3、6、12个月患肢体积差分别为治疗前与治疗后3、6、12个月患肢体积的差值
下载: 导出CSV
-
 陈宗灿.mp4
陈宗灿.mp4

-

 下载:
下载:



计量
- 文章访问数: 2329
- HTML全文浏览量: 779
- PDF下载量: 17
- 被引次数: 0
