




Multicenter retrospective analysis of early coagulation characteristics and risk factors for prognosis of adult patients with severe burns
-
摘要:
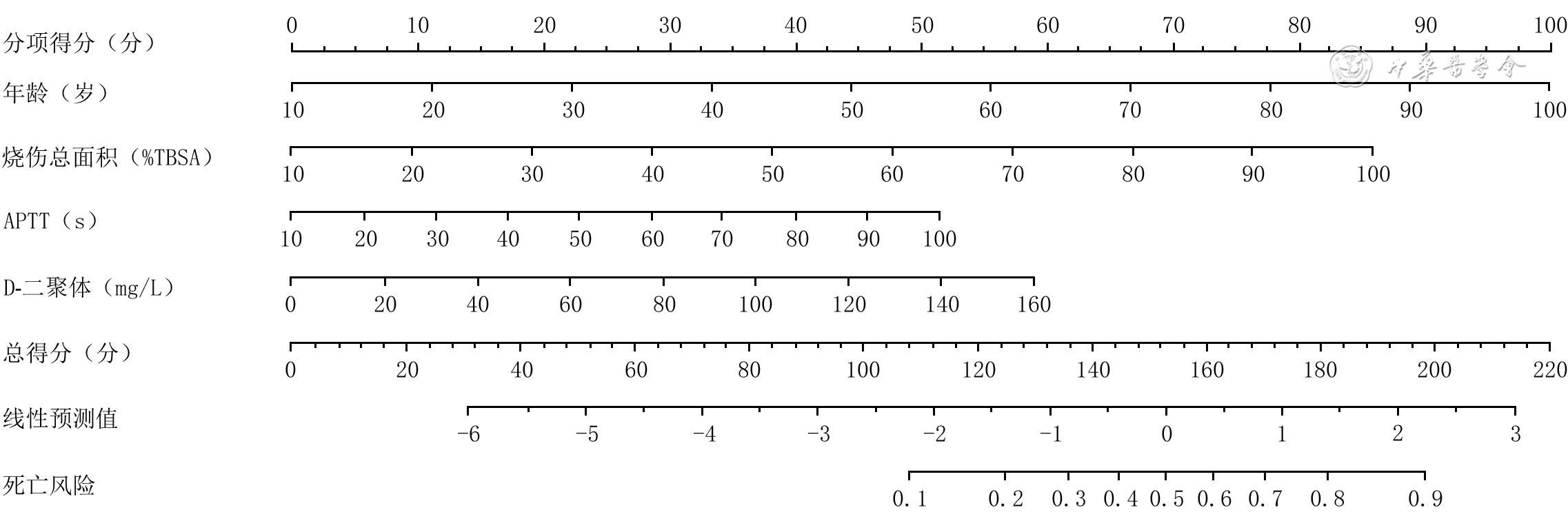
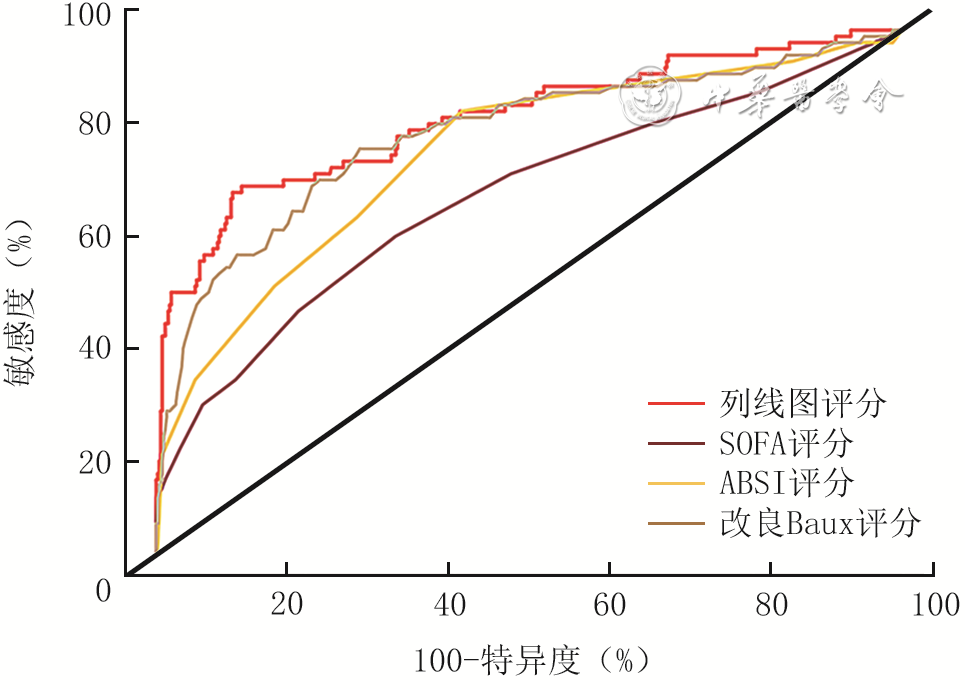
目的 探讨成年严重烧伤患者早期凝血特征及预后的危险因素。 方法 该研究为回顾性病例系列研究。2015年1月—2020年12月,全国12家医院共收治583例符合入选标准的成年严重烧伤患者,其中海军军医大学第一附属医院75例、武汉大学附属同仁医院暨武汉市第三医院64例、南通大学附属医院48例、暨南大学附属广州红十字会医院146例、解放军第924医院55例、郑州市第一人民医院46例、大连市第四人民医院35例、福建医科大学附属协和医院20例、张家港市第一人民医院18例、黑龙江省医院7例、浙江省台州医院18例、南昌大学第一附属医院51例。统计患者总体临床特征和伤后24 h内凝血功能指标,前者包括性别、年龄、烧伤总面积、吸入性损伤程度、致伤原因,后者包括凝血酶原时间(PT)、活化部分凝血活酶时间(APTT)、凝血酶时间(TT)、国际标准化比值(INR)及D-二聚体、纤维蛋白原(FIB)、血小板计数(PLT)和血清总钙水平。根据前述指标的相关数据,计算患者脓毒症相关性器官功能衰竭评价(SOFA)评分、改良Baux评分和简明烧伤严重指数(ABSI)评分。按照伤后28 d内的存活结局,将患者分为存活组(499例)和死亡组(84例)。比较2组患者总体临床特征指标及凝血功能指标。按照烧伤的严重程度,将患者分为烧伤总面积<50%体表总面积(TBSA)的重度烧伤组(185例)、烧伤总面积≥50%TBSA且<80%TBSA的特重烧伤组(251例)和烧伤总面积≥80%TBSA的危重烧伤组(147例),比较3组患者凝血功能指标。按照烧伤早期入院的具体时间,将伤后<2 h、≥2 h且<4 h、≥4 h且<8 h、≥8 h且<16 h及≥16 h且<24 h入院的患者分别设为烧伤早期1组(207例)、烧伤早期2组(158例)、烧伤早期3组(129例)、烧伤早期4组(54例)、烧伤早期5组(35例),比较5组患者凝血功能指标。筛选影响583例成年严重烧伤患者伤后28 d死亡的独立危险因素。根据独立危险因素绘制预测模型列线图。绘制基于SOFA评分、ABSI评分、改良Baux评分的预测模型的受试者操作特征(ROC)曲线并计算曲线下面积(AUC),并与基于列线图评分的预测模型的AUC进行比较。评估前述各预测模型的效能。 结果 583例患者中男409例、女174例,年龄18~97岁,烧伤总面积60.00%(44.50%,80.00%)TBSA,中重度吸入性损伤者138例。与存活组比较,死亡组患者年龄、烧伤总面积、INR更大,PT、APTT更长,D-二聚体、PLT水平及中重度吸入性损伤患者占比更高(Z值分别为6.47、7.48、3.48、2.89、2.79、5.33、2.59,χ2=11.30,P值均<0.05);2组患者仅D-二聚体水平高于正常范围的上限。重度烧伤组、特重烧伤组、危重烧伤组患者PT、APTT、INR及D-二聚体、PLT、血清总钙水平组间总体比较,差异均有统计学意义(H值分别为17.85、19.78、26.89、52.64、14.21、12.90,P<0.05)。烧伤早期1组、烧伤早期2组、烧伤早期3组、烧伤早期4组、烧伤早期5组患者PT、APTT、INR及D-二聚体、FIB、PLT及血清总钙水平组间总体比较,差异均有统计学意义(H值分别为29.66、60.13、25.51、28.24、14.38、11.41、42.96,P<0.05)。多因素logistic回归分析显示,年龄、烧伤总面积、APTT及D-二聚体水平均为成年严重烧伤患者伤后28 d死亡的独立危险因素(比值比分别为1.056、1.048、1.029、1.018,95%置信区间分别为1.036~1.076、1.033~1.063、1.005~1.053、1.002~1.035,P<0.05)。ROC曲线显示,基于SOFA评分、ABSI评分和改良Baux评分的预测模型的AUC分别为0.66、0.76、0.80,95%置信区间分别为0.61~0.75、0.71~0.82、0.74~0.86,均低于基于列线图评分的预测模型的0.81(95%置信区间为0.76~0.87)。DeLong检验显示,基于列线图评分的预测模型对成年严重烧伤患者伤后28 d死亡风险的预测能力明显优于基于SOFA评分和ABSI评分的预测模型(P值均<0.05),而与基于改良Baux评分的预测模型相近(P>0.05)。 结论 成年严重烧伤患者早期仅D-二聚体水平高于正常范围的上限。年龄、烧伤总面积、APTT与D-二聚体水平均为成年严重烧伤患者伤后28 d死亡的独立危险因素。 Abstract:Objective To investigate the early coagulation characteristics and risk factors for prognosis of adult patients with severe burns. Methods This study was a retrospective study of case series. A total of 583 adult patients with severe burns who met the inclusion criteria were admitted to the 12 hospitals in China from January 2015 to December 2020, including 75 cases from the First Affiliated Hospital of Naval Medical University, 64 cases from Tongren Hospital of Wuhan University & Wuhan Third Hospital, 48 cases from the Affiliated Hospital of Nantong University, 146 cases from the Guangzhou Red Cross Hospital of Jinan University, 55 cases from the 924th Hospital of PLA, 46 cases from Zhengzhou First People's Hospital, 35 cases from the Fourth People's Hospital of Dalian, 20 cases from Fujian Medical University Union Hospital, 18 cases from Zhangjiagang First People's Hospital, 7 cases from Heilongjiang Provincial Hospital, 18 cases from Taizhou Hospital of Zhejiang Province, and 51 cases from the First Affiliated Hospital of Nanchang University. The general clinical characteristics (including gender, age, total burn area, degree of inhalation injury, and cause of burn) and coagulation function indicators within 24 hours after injury (including prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), international normalized ratio (INR), and D-dimer, fibrinogen (FIB), platelets (PLT), and serum total calcium levels) of patients were statistically analyzed. Based on the data of the above indicators, the sepsis-related organ failure assessment (SOFA) score, modified Baux score, and abbreviated burn severity index (ABSI) score of patients were calculated. According to the survival outcome within 28 days after injury, the patients were divided into survival group (499 cases) and death group (84 cases). General clinical characteristics and coagulation function indicators were compared between the 2 groups of patients. According to the severity of burns, patients were divided into three groups: severe burn group (185 cases ) with a total burn area <50% total body surface area (TBSA), extremely severe burn group (251 cases) with a total burn area ≥50% and <80%TBSA, and critical burn group (147 cases) with a total burn area ≥80%TBSA. Coagulation function indicators were compared among the 3 groups of patients. Based on the specific time of admission at the early stage of burns, patients with admission time <2 h, ≥2 h and <4 h, ≥4 h and <8 h, ≥8 h and <16 h, and ≥16 h and <24 h after burns were divided respectively into early burn group 1 (207 cases), early burn group 2 (158 cases), early burn group 3 (129 cases), early burn group 4 (54 cases), and early burn group 5 (35 cases), and the coagulation function indicators were compared among the 5 groups of patients. The independent risk factors affecting mortality 28 days after injury in 583 adult patients with severe burns were screened. A predictive nomogram was constructed based on the independent risk factors. Receiver operating characteristic (ROC) curves were constructed and the area under the curves (AUCs) was calculated for prediction models based on SOFA score, ABSI score, and modified Baux score. The AUC based on the nomogram score was compared with those of the aforementioned prediction models. The efficacy of the aforementioned prediction models was assessed. Results Among the 583 patients, there were 409 males and 174 females, aged 18-97 years, with total burn area of 60.00% (44.50%, 80.00%) TBSA and 138 patients with moderate-to-severe inhalation injury. Compared with those in survival group, patients in death group had larger age, total burn area, and INR, longer PT and APTT, higher D-dimer and PLT levels, and proportion of moderate-to-severe inhalation injury (with Z values of 6.47, 7.48, 3.48, 2.89, 2.79, 5.33, and 2.59, respectively, χ2=11.30, all P values <0.05). Only D-dimer level in the 2 group of patients was above the upper limit of the normal range. There were statistically significant differences among severe burn group, extremely severe burn group, and critical burn group of patients in terms of PT, APTT, INR, and D-dimer, PLT, serum total calcium levels (with H values of 17.85, 19.78, 26.89, 52.64, 14.21, and 12.90, respectively, P<0.05). There were statistically significant differences among early burn group 1, early burn group 2, early burn group 3, early burn group 4, and early burn group 5 of patients in terms of PT, APTT, INR, and D-dimer, FIB, PLT, serum total calcium levels (with H values of 29.66, 60.13, 25.51, 28.24, 14.38, 11.41, and 42.96, respectively, P<0.05). Multivariate logistic regression analysis showed that age, total burn area, APTT, and D-dimer level were independent risk factors for mortality 28 days after injury in adult patients with severe burns (with odds ratios of 1.056, 1.048, 1.029, and 1.018, respectively, 95% cofidence intervals (CIs) of 1.036-1.076, 1.033-1.063, 1.005-1.053, and 1.002-1.035, respectively, P<0.05). The ROC curves showed that the AUCs of the predictive models based on the SOFA score, ABSI score, and modified Baux score were 0.66, 0.76, and 0.80, respectively, with 95% CIs of 0.61-0.75, 0.71-0.82, and 0.74-0.86, respectively, which were all lower than 0.81 (95% CI of 0.76-0.87) of the nomogram score-based predictive model. The DeLong test showed that the predictive ability of the nomogram score-based model for predicting mortality risk in adult patients with severe burns 28 days after injury was significantly better than those of the models based on the SOFA score and ABSI score (both P values <0.05), but similar to that of the prediction model based on the modified Baux score (P>0.05). Conclusions In the early stage of adult patients with severe burns, only D-dimer level was above the upper limit of the normal range. Age, total burn area, APTT, and D-dimer level are all independent risk factors for mortality in adult patients with severe burns 28 days after injury. -
Key words:
- Burns /
- Adult /
- Prognosis /
- Risk factors /
- Coagulation /
- Retrospective study
-
参考文献
(40) [1] KaitaY, NishimuraH, TanakaY, et al. Effect of acute coagulopathy before fluid administration in mortality for burned patients[J]. Burns, 2021,47(4):805-811. DOI: 10.1016/j.burns.2020.10.011. [2] KorkmazHI, FlokstraG, WaasdorpM, et al. The complexity of the post-burn immune response: an overview of the associated local and systemic complications[J]. Cells, 2023, 12(3):345.DOI: 10.3390/cells12030345. [3] GlasGJ, LeviM, SchultzMJ. Coagulopathy and its management in patients with severe burns[J]. J Thromb Haemost, 2016,14(5):865-874. DOI: 10.1111/jth.13283. [4] MeizosoJP, RayJJ, AllenCJ, et al. Hypercoagulability and venous thromboembolism in burn patients[J]. Semin Thromb Hemost, 2015,41(1):43-48. DOI: 10.1055/s-0034-1398380. [5] JeschkeMG, van BaarME, ChoudhryMA, et al. Burn injury[J]. Nat Rev Dis Primers, 2020,6(1):11. DOI: 10.1038/s41572-020-0145-5. [6] LavrentievaA, KontakiotisT, BitzaniM, et al. Early coagulation disorders after severe burn injury: impact on mortality[J]. Intensive Care Med, 2008,34(4):700-706. DOI: 10.1007/s00134-007-0976-5. [7] MitraB, WasiakJ, CameronPA, et al. Early coagulopathy of major burns[J]. Injury, 2013,44(1):40-43. DOI: 10.1016/j.injury.2012.05.010. [8] LuRP, NiA, LinFC, et al. Major burn injury is not associated with acute traumatic coagulopathy[J]. J Trauma Acute Care Surg, 2013,74(6):1474-1479. DOI: 10.1097/TA.0b013e3182923193. [9] SingerM, DeutschmanCS, SeymourCW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3)[J]. JAMA, 2016,315(8):801-810. DOI: 10.1001/jama.2016.0287. [10] LionelliGT, PickusEJ, BeckumOK, et al. A three decade analysis of factors affecting burn mortality in the elderly[J]. Burns, 2005,31(8):958-963. DOI: 10.1016/j.burns.2005.06.006. [11] PratNJ, HerzigMC, KreyerS, et al. Platelet and coagulation function before and after burn and smoke inhalation injury in sheep[J]. J Trauma Acute Care Surg, 2017,83(1 Suppl 1):S59-65. DOI: 10.1097/TA.0000000000001472. [12] GuilabertP, MartinN, UsúaG, et al. Coagulation alterations in major burn patients: a narrative review[J]. J Burn Care Res, 2023,44(2):280-292. DOI: 10.1093/jbcr/irac177. [13] LiN, TanJ, FengX, et al. Early coagulation disorder and the predictive value of D-dimer for deep vein thrombosis in major burn patients[J]. Burns, 2025,51(3):107398. DOI: 10.1016/j.burns.2025.107398. [14] 宋景春, 张伟, 张磊, 等. 重症患者凝血功能障碍标准化评估中国专家共识[J].解放军医学杂志,2022,47(2):107-117. DOI: 10.11855/j.issn.0577-7402.2022.02.0107. [15] 马琪敏, 刘晓彬, 伍国胜, 等. 特重度成年烧伤患者休克期凝血特征及其预警价值的回顾性队列研究[J].中华烧伤杂志,2021,37(2):150-156. DOI: 10.3760/cma.j.cn501120-20200907-00402. [16] JeschkeMG, MlcakRP, FinnertyCC, et al. Burn size determines the inflammatory and hypermetabolic response[J]. Crit Care, 2007,11(4):R90. DOI: 10.1186/cc6102. [17] 郭光华,孙威. 吸入性损伤气道内给药目标靶向治疗[J]. 中华烧伤杂志,2018,34(7):445-449.DOI: 10.3760/cma.j.issn.1009-2587.2018.07.005. [18] MurakamiK, TraberDL. Pathophysiological basis of smoke inhalation injury[J]. News Physiol Sci, 2003,18:125-129. DOI: 10.1152/nips.01427.2002. [19] CoxRA, MlcakRP, ChinkesDL, et al. Upper airway mucus deposition in lung tissue of burn trauma victims[J]. Shock, 2008,29(3):356-361. DOI: 10.1097/shk.0b013e31814541dd. [20] NetworkARDS, BrowerRG, MatthayMA, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome[J]. N Engl J Med, 2000,342(18):1301-1308. DOI: 10.1056/NEJM200005043421801. [21] 郭光华, 黄圣宇. 吸入性损伤再认识[J].中华烧伤与创面修复杂志,2024,40(11):1001-1006. DOI: 10.3760/cma.j.cn501225-20240616-00234. [22] LevinGY, EgorihinaMN. The role of fibrinogen in aggregation of platelets in burn injury[J]. Burns, 2010,36(6):806-810. DOI: 10.1016/j.burns.2009.05.005. [23] KoamiH, SakamotoY, MatsuokaA, et al. Thromboelastometric analysis of the correlation between burn-induced coagulopathy and severity of burn injury[J]. Cureus, 2024,16(2):e54489. DOI: 10.7759/cureus.54489. [24] AlkjaersigN, FletcherAP, PedenJCJr, et al. Fibrinogen catabolism in burned patients[J]. J Trauma, 1980,20(2):154-159. DOI: 10.1097/00005373-198002000-00009. [25] NikolaidouE, KakagiaD, KaldoudiE, et al. Coagulation disorders and mortality in burn injury: a systematic review[J]. Ann Burns Fire Disasters, 2022,35(2):103-115. [26] LawrenceC, AtacB. Hematologic changes in massive burn injury[J]. Crit Care Med, 1992,20(9):1284-1288. DOI: 10.1097/00003246-199209000-00015. [27] Kowal-VernA, WalengaJM, HoppensteadtD, et al. Prothrombin fragment 1.2 and modified antithrombin as predictors of disseminated intravascular coagulation and thrombotic risk in thermal injury[J]. J Burn Care Res, 2013,34(4):459-464. DOI: 10.1097/BCR.0b013e3182700659. [28] KingDR, NamiasN, AndrewsDM. Coagulation abnormalities following thermal injury[J]. Blood Coagul Fibrinolysis, 2010,21(7):666-669. DOI: 10.1097/MBC.0b013e32833ceb08. [29] NiemiT, SvartlingN, SyrjäläM, et al. Haemostatic disturbances in burned patients during early excision and skin grafting[J]. Blood Coagul Fibrinolysis, 1998,9(1):19-28. DOI: 10.1097/00001721-199801000-00003. [30] WiegeleM, SchadenE, KochS, et al. Thrombin generation in patients with severe thermal injury[J]. Burns, 2019,45(1):54-62. DOI: 10.1016/j.burns.2018.09.020. [31] 欧阳宇楠.探讨快速补液对烧伤休克延迟复苏病人脏器损害的防治作用[J].中国科技期刊数据库 医药,2024(6):82-85. [32] BallRL, KeylounJW, Brummel-ZiedinsK, et al. Burn-induced coagulopathies: a comprehensive review[J]. Shock, 2020,54(2):154-167. DOI: 10.1097/SHK.0000000000001484. [33] HuangS, MaQ, LiaoX, et al. Identification of early coagulation changes associated with survival outcomes post severe burns from multiple perspectives[J]. Sci Rep, 2024,14(1):10457. DOI: 10.1038/s41598-024-61194-0. [34] MaugeriN, BrambillaM, CameraM, et al. Human polymorphonuclear leukocytes produce and express functional tissue factor upon stimulation[J]. J Thromb Haemost, 2006,4(6):1323-1330. DOI: 10.1111/j.1538-7836.2006.01968.x. [35] MassbergS, GrahlL, von BruehlML, et al. Reciprocal coupling of coagulation and innate immunity via neutrophil serine proteases[J]. Nat Med, 2010,16(8):887-896. DOI: 10.1038/nm.2184. [36] DarboussetR, ThomasGM, MezouarS, et al. Tissue factor-positive neutrophils bind to injured endothelial wall and initiate thrombus formation[J]. Blood, 2012,120(10):2133-2143. DOI: 10.1182/blood-2012-06-437772. [37] García-AvelloA, LorenteJA, Cesar-PerezJ, et al. Degree of hypercoagulability and hyperfibrinolysis is related to organ failure and prognosis after burn trauma[J]. Thromb Res, 1998,89(2):59-64. DOI: 10.1016/s0049-3848(97)00291-0. [38] 李云, 张庭, 宁金斌, 等. 特重度烧伤患者死亡的风险预测模型构建[J].保健医学研究与实践,2024,21(12):108-113. [39] 陈华勇,辛国华. 烧伤患者预后相关预测模型的研究进展[J]. 中华烧伤与创面修复杂志,2023,39(9):891-895.DOI: 10.3760/cma.j.cn501225-20221022-00468. [40] HalgasB, BayC, FosterK. A comparison of injury scoring systems in predicting burn mortality[J]. Ann Burns Fire Disasters, 2018,31(2):89-93. -

图 3 基于不同评分的预测模型预测583例成年严重烧伤患者伤后28 d死亡风险能力比较
注:图中直线为参考线;列线图指基于年龄、烧伤总面积、活化部分凝血活酶时间及D-二聚体水平构建的预测模型;SOFA为脓毒症相关性器官功能衰竭评价,ABSI为简明烧伤严重指数
Table 1. 2组成年严重烧伤患者总体临床特征比较
组别 例数 性别(例) 年龄[岁,M(Q1,Q3)] 烧伤总面积[%TBSA,M(Q1,Q3)] 致伤原因(例) 吸入性损伤程度(例) 男 女 火焰烧伤 化学烧伤 电烧伤 热液烫伤 轻度或无 中重度 存活组 499 347 152 47.00(35.00,56.00) 55.00(40.00,75.00) 406 18 25 50 393 106 死亡组 84 62 22 56.00(47.75,68.00) 85.00(60.00,94.25) 73 1 1 9 52 32 统计量值 χ2 =0.44 Z=6.47 Z=7.48 — χ2=11.30 P值 0.508 <0.001 <0.001 0.268 <0.001 注:TBSA为体表总面积;按照伤后28 d内的存活结局,将患者分为存活组和死亡组;“—”表示无此项  下载: 导出CSV
下载: 导出CSV
Table 2. 2组成年严重烧伤患者凝血功能指标比较[M(Q1,Q3)]
组别 例数 PT(s) APTT(s) TT(s) D-二聚体(mg/L) INR FIB(g/L) PLT(×109/L) 血清总钙(mmol/L) 存活组 499 11.60(11.00,12.60) 27.10(23.35,31.65) 18.50(16.90,20.10) 2.27(1.05,5.27) 0.99(0.93,1.08) 2.50(2.00,3.12) 234.00(171.50,303.50) 2.04(1.82,2.19) 死亡组 84 12.20(11.25,14.00) 31.30(24.43,38.20) 18.60(16.88,20.33) 5.32(2.63,14.96) 1.06(0.97,1.19) 2.58(1.96,3.34) 267.50(197.75,363.50) 2.01(1.83,2.16) Z值 2.89 2.79 0.50 5.33 3.48 0.47 2.59 0.24 P值 0.004 0.005 0.614 <0.001 0.001 0.639 0.010 0.813 注:PT为凝血酶原时间,APTT为活化部分凝血活酶时间,TT为凝血酶时间,INR为国际标准化比值,FIB为纤维蛋白原,PLT为血小板计数;按照伤后28 d内的存活结局,将患者分为存活组和死亡组
下载: 导出CSV
Table 3. 3组成年严重烧伤患者凝血功能指标比较[M(Q1,Q3)]
组别 例数 PT(s) APTT(s) TT(s) D-二聚体(mg/L) INR FIB(g/L) PLT(×109/L) 血清总钙(mmol/L) 重度烧伤组 185 11.50(10.80,12.10) 25.90(23.10,29.20) 18.50(17.00,19.70) 1.60(0.70,3.70) 0.98(0.91,1.04) 2.60(2.00,3.10) 223.00(175.00,273.00) 2.08(1.87,2.20) 特重烧伤组 251 11.70(11.10,12.75) 27.90(23.55,32.85) 18.00(16.40,19.95) 2.59(1.20,6.20) 1.00(0.94,1.10) 2.51(2.00,3.26) 238.00(168.00,309.50) 2.03(1.87,2.17) 危重烧伤组 147 12.00(11.20,13.80) 29.60(23.90,37.45) 19.40(17.70,21.25) 4.70(2.07,7.42) 1.05(0.96,1.16) 2.43(1.86,3.12) 270.00(200.50,362.00) 1.96(1.67,2.14) H值 17.85 19.78 20.83 52.64 26.89 1.71 14.21 12.90 P值 <0.001 <0.001 0.614 <0.001 <0.001 0.424 0.001 0.002 注:PT为凝血酶原时间,APTT为活化部分凝血活酶时间,TT为凝血酶时间,INR为国际标准化比值,FIB为纤维蛋白原,PLT为血小板计数;按照烧伤的严重程度,将患者分为烧伤总面积<50%体表总面积(TBSA)的重度烧伤组、烧伤总面积≥50%TBSA且<80%TBSA的特重烧伤组和烧伤总面积≥80%TBSA的危重烧伤组
下载: 导出CSV
Table 4. 5组成年严重烧伤患者凝血功能指标比较[M(Q1,Q3)]
组别 例数 PT(s) APTT(s) TT(s) D-二聚体(mg/L) INR FIB(g/L) PLT(×109/L) 血清总钙(mmol/L) 烧伤早期1组 207 11.50(10.80,12.30) 25.10(22.10,29.90) 18.60(17.00,20.20) 1.65(0.76,4.49) 0.98(0.93,1.05) 2.57(2.00,3.22) 248.00(189.50,324.00) 2.11(1.96,2.24) 烧伤早期2组 158 11.65(11.00,12.67) 26.60(23.50,30.60) 18.30(16.90,20.20) 3.02(1.45,7.39) 1.00(0.93,1.10) 2.40(1.89,3.06) 245.50(171.75,320.25) 2.05(1.86,2.19) 烧伤早期3组 129 11.80(11.20,13.00) 29.00(24.50,33.00) 18.80(17.30,20.50) 3.22(1.23,6.61) 1.00(0.96,1.12) 2.46(2.00,3.12) 237.00(180.00,297.00) 1.97(1.73,2.11) 烧伤早期4组 54 12.65(11.72,14.50) 33.75(28.92,42.03) 17.85(16.50,19.80) 3.06(1.83,6.69) 1.08(1.01,1.24) 2.44(1.65,3.09) 220.50(168.00,279.50) 1.88(1.66,2.06) 烧伤早期5组 35 11.70(10.90,12.75) 29.60(25.00,35.80) 17.30(15.70,19.40) 1.87(0.98,3.92) 1.00(0.92,1.10) 2.94(2.58,3.80) 195.00(122.00,251.00) 1.86(1.30,2.02) H值 29.66 60.13 7.68 28.24 25.51 14.38 11.41 42.96 P值 <0.001 <0.001 0.104 <0.001 <0.001 0.006 0.022 <0.001 注:PT为凝血酶原时间,APTT为活化部分凝血活酶时间,TT为凝血酶时间,INR为国际标准化比值,FIB为纤维蛋白原,PLT为血小板计数;按照烧伤早期入院的具体时间,将伤后<2 h、≥2 h且<4 h、≥4 h且<8 h、≥8 h且<16 h及≥16 h且<24 h入院的患者分别设为烧伤早期1组、烧伤早期2组、烧伤早期3组、烧伤早期4组、烧伤早期5组
下载: 导出CSV
Table 5. 影响583例成年严重烧伤患者伤后28 d死亡的单因素logistic回归分析结果
自变量 比值比 95%置信区间 P值 年龄(岁) 1.039 1.025~1.053 <0.001 烧伤总面积(%TBSA) 1.048 1.033~1.063 <0.001 中重度吸入性损伤 1.604 1.326~1.941 <0.001 PT(s) 1.193 1.084~1.319 <0.001 APTT(s) 1.059 1.041~1.077 <0.001 D-二聚体(mg/L) 1.021 1.009~1.034 <0.001 INR 6.056 2.144~17.392 0.001 PLT(×109/L) 1.002 1.001~1.004 0.002 注:TBSA为体表总面积,PT为凝血酶原时间,APTT为活化部分凝血活酶时间,INR为国际标准化比值,PLT为血小板计数
下载: 导出CSV
Table 6. 影响583例成年严重烧伤患者伤后28 d死亡的多因素logistic回归分析结果
自变量 比值比 95%置信区间 P值 年龄(岁) 1.056 1.036~1.076 <0.001 烧伤总面积(%TBSA) 1.048 1.033~1.063 <0.001 APTT(s) 1.029 1.005~1.053 0.017 D-二聚体(mg/L) 1.018 1.002~1.035 0.027 注:TBSA为体表总面积,APTT为活化部分凝血活酶时间
下载: 导出CSV
-

 下载:
下载:


计量
- 文章访问数: 6506
- HTML全文浏览量: 1777
- PDF下载量: 40
- 被引次数: 0
