




Clinical efficacy of two-stage ear reconstruction using autologous rib cartilage in the correction of congenital microtia
-
摘要:
目的 探讨应用自体肋软骨行二期法全耳再造术矫正先天性小耳畸形的临床疗效。 方法 该研究为回顾性队列研究。2000年1月—2025年2月,上海交通大学医学院附属第九人民医院整复外科收治3 050例(男1 992例、女1 058例,年龄6~52岁)符合入选标准的先天性小耳畸形患者,均采用二期法全耳再造术进行矫正。Ⅰ期手术包括切取自体第6~8肋软骨(必要时切取自体第9肋软骨)进行支架雕刻,根据残耳组织量及位置设计横行、纵行、“V”形、“U”形或“W”形切口,然后植入雕刻的支架并封闭创面。术后3~6个月行Ⅱ期手术:先掀起再造耳并用预留软骨或钛板作为支撑材料构建颅耳角,再用耳后局部筋膜瓣+头部断层皮片封闭创面。对供皮区创面进行打包固定。术后,统计并发症发生情况并计算其发生率。随访时,观察再造耳外观,统计患者的满意度或不满意的原因。 结果 6.59%(201/3 050)的患者Ⅰ期术后发生静脉回流障碍、皮瓣坏死或软骨外露等并发症,9.18%(280/3 050)的患者Ⅱ期术后发生皮片部分坏死、筋膜瓣坏死、软骨外露等并发症,经采取针刺放血+用肝素溶液浸润的纱布湿敷、清创引流、高压氧治疗、合理应用抗生素及应用筋膜瓣+皮片移植修复等处理措施后均得到有效控制。Ⅱ期术后6个月~15年随访时,再造耳各亚单位形态显现,比例协调,结构柔和自然,89.02%(2 715/3 050)的患者及其家属对再造耳轮廓形态和位置大小表示满意,其余患者不满意原因为术后并发症引起再造耳局部结构缺陷或因半侧颜面短小畸形及异位耳道等因素引起再造耳位置不对称。 结论 应用自体肋软骨行二期法全耳再造术矫正先天性小耳畸形,术后并发症发生率低,再造耳结构自然,患者满意度高,是一种可靠的术式。 Abstract:Objective To explore the clinical efficacy of two-stage ear reconstruction using autologous rib cartilage in the correction of congenital microtia. Methods The study was a retrospective cohort study. From January 2000 to February 2025, 3 050 patients (1 992 males and 1 058 females, aged 6 to 52 years) with congenital microtia who met the inclusion criteria were admitted to the Department of Plastic and Reconstructive Surgery of Shanghai Ninth People's Hospital of Shanghai Jiao Tong University School of Medicine. All of them were corrected by the two-stage ear reconstruction. The first stage operation involved harvesting of the 6th to 8th autologous rib cartilages (the 9th autologous rib cartilage was harvested if necessary) for ear framework fabrication. Depending on the amount and location of residual ear tissue, the transverse, longitudinal, "V"-shaped, "U"-shaped, or "W"-shaped incisions were designed, and then fabricated frameworks were implanted, and the wounds were closed. The second stage operation was performed 3 to 6 months after operation. The reconstructed ear was first lifted, the reserved cartilage or titanium plate was used as supporting material to construct the cranio-auricular angle, and then the wound was closed with retroauricular fascial flap and split-thickness scalp skin graft. The wound at the donor site of the skin graft was packaged and fixed. After operation, the incidence of complications was recorded, and the occurrence rate was calculated. During the follow-up, the appearance of the reconstructed ear was observed, and the patients' satisfaction or reasons for dissatisfaction were counted. Results The complications, such as venous congestion, flap necrosis, and cartilage exposure, etc. occurred in the first stage operation, and the occurrence rate was 6.59% (201/3 050); partial skin graft necrosis, fascial flap necrosis, and cartilage exposure, etc. occurred in the second stage operation, and the occurrence rate was 9.18% (280/3 050). The complications were all controlled effectively after adopting treatment measures such as acupuncture and bloodletting combined with wet compress using gauze soaked in heparin solution, debridement and drainage, hyperbaric oxygen therapy, rational application of antibiotics, and repair with fascial flaps and skin grafts. During the follow-up of 6 months to 15 years after the second stage operation, the morphology of each sub-unit of the reconstructed ear appeared, the proportion was coordinated, and the structure was soft and natural. 89.02% (2 715/3 050) of the patients and their families were satisfied with the shape contour, position, and size of the reconstructed ear. The reasons for the dissatisfaction of the remaining patients were local structural defects of the reconstructed ear caused by postoperative complications, asymmetry in the position of the reconstructed ear due to factors such as hemifacial microsomia and ectopic auditory meatus. Conclusions Two-stage ear reconstruction using autologous rib cartilage in the correction of congenital microtia is a reliable surgical technique, characterized by a low incidence of postoperative complications, natural anatomical structure of the reconstructed ear, and high patient satisfaction. -
参考文献
(40) [1] TanzerRC. Total reconstruction of the auricle. The evolution of a plan of treatment[J]. Plast Reconstr Surg, 1971,47(6):523-533. DOI: 10.1097/00006534-197106000-00001. [2] BrentB. Technical advances in ear reconstruction with autogenous rib cartilage grafts: personal experience with 1200 cases[J]. Plast Reconstr Surg, 1999,104(2):319-334; discussion 335-338. DOI: 10.1097/00006534-199908000-00001. [3] NagataS. A new method of total reconstruction of the auricle for microtia[J]. Plast Reconstr Surg, 1993,92(2):187-201. DOI: 10.1097/00006534-199308000-00001. [4] ParkC. Subfascial expansion and expanded two-flap method for microtia reconstruction[J]. Plast Reconstr Surg, 2000,106(7):1473-1487. DOI: 10.1097/00006534-200012000-00005. [5] FirminF. Ear reconstruction in cases of typical microtia. Personal experience based on 352 microtic ear corrections[J]. Scand J Plast Reconstr Surg Hand Surg, 1998,32(1):35-47. DOI: 10.1080/02844319850158930. [6] ZhangQ, ZhangR, XuF, et al. Auricular reconstruction for microtia: personal 6-year experience based on 350 microtia ear reconstructions in China[J]. Plast Reconstr Surg, 2009,123(3):849-858. DOI: 10.1097/PRS.0b013e318199f057. [7] BauerBS. Reconstruction of microtia[J]. Plast Reconstr Surg, 2009,124(1):14e-26e. DOI: 10.1097/PRS.0b013e3181aa0e79. [8] WilkesGH, WongJ, GuilfoyleR. Microtia reconstruction[J]. Plast Reconstr Surg, 2014,134(3):464e-479e. DOI: 10.1097/PRS.0000000000000526. [9] 张如鸿,章庆国.外耳修复再造学[M].杭州:浙江科学技术出版社,2014:9-22. [10] 张如鸿.先天性小耳畸形患者耳廓再造的美学重建研究[J].中华耳鼻咽喉头颈外科杂志,2015,50(3):187-191. DOI: 10.3760/cma.j.issn.1673-0860.2015.03.003. [11] 章庆国.先天性小耳畸形治疗技术体系的构建[J].中国美容整形外科杂志,2023, 34(8):449-451,463. DOI: 10.3969/j.issn.1673-7040.2023.08.001. [12] 王秀, 张朕坡, 郭旭伦,等. 成年小耳畸形患者全耳廓再造术的总结与分析[J]. 中华耳鼻咽喉头颈外科杂志, 2023,58(5):476-480. DOI: 10.3760/cma.j.cn115330-20230113-00020. [13] 李腾海, 杨田野, 彭维海. 3D打印耳廓模型在耳廓再造软骨支架雕刻成形中的应用[J]. 吉林大学学报(医学版), 2023,49(3):770-776. DOI: 10.13481/j.1671-587X.20230328. [14] 王振宇, 王洪一, 金元,等. 内镜辅助切取颞浅筋膜瓣在Nagata法二期耳廓再造中的应用[J]. 中华整形外科杂志, 2023,39(11):1222-1228. DOI: 10.3760/cma.j.cn114453-20230131-00019. [15] 高德瑾, 王冰清, 章庆国. 先天性小耳畸形行耳再造术后的评价维度的总结与讨论[J]. 组织工程与重建外科,2025,21(3):316-318. DOI: 10.3969/j.issn.1673-0364.2025.03.017. [16] 曹烈旭, 龚志成, 黄坤,等. 数字化技术在耳再造术耳后软骨支架中的应用[J]. 中国美容整形外科杂志, 2025, 36(4):197-200. DOI: 10.3969/j.issn.1673-7040.2025.04.003. [17] YamadaA. Autologous rib microtia construction: Nagata technique[J]. Facial Plast Surg Clin North Am,2018,26(1):41-55. DOI: 10.1016/j.fsc.2017.09.006. [18] ChenX, ZhangR, ZhangQ, et al. Microtia part I: preoperation and in-operation lessons from 1012 ear reconstruction operations[J]. Aesthetic Plast Surg, 2022,46(6):2781-2787. DOI: 10.1007/s00266-022-02818-6. [19] LiD, XuF, ZhangR, et al. Surgical reconstruction of traumatic partial ear defects based on a novel classification of defect sizes and surrounding skin conditions[J]. Plast Reconstr Surg,2016,138(2):307e-316e. DOI: 10.1097/PRS.0000000000002408. [20] ParkJY, ParkC. Microtia reconstruction in hemifacial microsomia patients: three framework coverage techniques[J]. Plast Reconstr Surg,2018,142(6):1558-1570. DOI: 10.1097/PRS.0000000000005063. [21] 许志成, 张如鸿, 章庆国,等. 先天性小耳畸形应用自体肋软骨二期法全耳再造诊疗专家共识[J]. 组织工程与重建外科,2025,21(1):1-9. DOI: 10.3969/j.issn.1673-0364.2025.01.001. [22] LiY, LiD, XuZ, et al. New strategies for base frame fabrication in microtia reconstruction[J]. Sci Rep,2021,11(1):15947. DOI: 10.1038/s41598-021-95613-3. [23] XuZ, LiY, LiD, et al. Strategies for surgical refinement of the antihelical complex using autologous costal cartilage in auricular reconstruction for microtia[J/OL]. Facial Plast Surg Aesthet Med,2025(2025-04-23)[2025-09-23]. https://pubmed.ncbi.nlm.nih.gov/40265295/. DOI: 10.1089/fpsam.2024.0363. [published online ahead of print]. [24] XuZ, ZhangR, ZhangQ, et al. New strategies for tragus and antitragus complex fabrication in lobule-type microtia reconstruction[J]. Plast Reconstr Surg,2019,144(4): 913-921. DOI: 10.1097/PRS.0000000000006043. [25] XuZ, XuF, ZhangR, et al. A new classification of helix fabrication methods with autogenous costal cartilage in microtia reconstruction[J]. Plast Reconstr Surg,2017, 139(6):1315e-1324e. DOI: 10.1097/PRS.0000000000003375. [26] XuZ, LiY, LiD, et al. Strategies for ear elevation and the treatment of relevant complications in autologous cartilage microtia reconstruction[J]. Sci Rep,2022,12(1): 13536. DOI: 10.1038/s41598-022-17007-3. [27] NagataS. Modification of the stages in total reconstruction of the auricle: part Ⅱ. Grafting the three-dimensional costal cartilage framework for concha type microtia[J]. Plast Reconstr Surg,1994,93(2):231-242. [28] NagataS. Modification of the stages in total reconstruction of the auricle: part I. Grafting the three dimensional costal cartilage framework for lobule-type microtia[J]. Plast Reconstr Surg,1994,93(2):221-230. [29] XuZ, ZhangR, ZhangQ, et al. New strategies for remnant ear treatment in lobule-type microtia reconstruction[J]. Plast Reconstr Surg,2018,142(2):471-479. DOI: 10.1097/PRS.0000000000004610. [30] XuZ, LiY, LiD, et al. New strategies for remnant ear treatment in microtia reconstruction based on morphometric studies[J]. Laryngoscope,2024,134(6):2741-2747. DOI: 10.1002/lary.31224. [31] XuZ, ZhangR, ZhangQ, et al. An analysis of quantitative measurements of drainage exudate using negative suction in 96 microtia ear reconstructions[J]. Can J Plast Surg,2012,20(4):218-222. DOI: 10.1177/229255031202000401. [32] 刘新义, 周燕春, 石嘉栋,等. 先天性小耳畸形患者耳廓再造术后相关症状管理:经验介绍[J]. 中华整形外科杂志, 2025,41(10):1104-1105. DOI: 10.3760/cma.j.cn114453-20230831-00040. [33] 秦文英, 韩文娟, 桂芫芫. 小耳畸形外耳再造术后并发症相关危险因素预测模型建立及结构式与叙事疗法分析[J]. 组织工程与重建外科,2025,21(3):258-266. DOI: 10.3969/j.issn.1673-0364.2025.03.007. [34] LiD, SunJ, ZhangR, et al. Firm elevation of the auricle in reconstruction of microtia with a retroauricular fascial flap wrapping two titanium plate struts[J]. J Plast Reconstr Aesthet Surg,2023,83:134-140. DOI: 10.1016/j.bjps.2023.04.072. [35] LiY, ZhangR, ZhangQ, et al. An alternative posterosuperior auricular fascia flap for ear elevation during microtia reconstruction[J]. Aesthetic Plast Surg,2017,41(1):47-55. DOI: 10.1007/s00266-016-0743-5. [36] LiD, ZhangR, ZhangQ, et al. Clinical results of ear elevations in patients with microtia using skin grafts from three donor sites: a retrospective study[J]. Aesthetic Plast Surg,2020,44(5):1545-1552. DOI: 10.1007/s00266-020-01711-4. [37] 邓毅文, 潘博, 蒋海越. 自体肋软骨耳再造术后胸廓畸形发生机制和预防策略[J]. 中华整形外科杂志, 2025,41(8):860-864. DOI: 10.3760/cma.j.cn114453-20240109-00016. [38] CuiC, HoonSY, ZhangR, et al. Patient satisfaction and its influencing factors of microtia reconstruction using autologous cartilage[J]. Aesthetic Plast Surg,2017,41(5): 1106-1114. DOI: 10.1007/s00266-017-0907-y. [39] XuF, ZhangR, ZhangQ, et al. Hyperbaric oxygen therapy: an effective and noninvasive therapy for complications of ear reconstruction[J]. J Craniofac Surg, 2019,30(4):e382-e385. DOI: 10.1097/SCS.0000000000004969. [40] LiY, CuiC, ZhangR, et al. Anatomical and histological evaluation of the retroauricular fascia flap for staged auricular reconstruction[J]. Aesthetic Plast Surg, 2018,42(3):625-632. DOI: 10.1007/s00266-018-1098-x. -

图 1 应用自体第6~9肋软骨进行的耳支架雕刻。1A.应用第8肋软骨(红色箭头示)、第9肋软骨(黄色箭头示)雕刻为外耳轮结构,并将“Y”形对耳轮和对耳屏复合体固定于第6、7肋软骨雕刻的底板之上,残耳软骨拟雕刻为耳屏结构;1B.支架雕刻完成后即刻

图 2 二期法全耳再造术的Ⅰ期手术中的切口设计和残耳处理。2A.术中切口线设计;2B.术中切开皮下组织,保留皮下蒂;2C.术中切取自体肋软骨;2D.将雕刻完成的耳软骨支架植入残耳皮下后即刻

图 3 二期法全耳再造术的Ⅱ期手术过程。3A.术中切口设计;3B.术中应用的自体肋软骨块支撑材料的正面观(左侧)和侧面观(右侧);3C.术中应用自体软骨块支撑再造耳,用钛丝固定形成颅耳角;3D.术中应用耳后局部筋膜瓣翻转覆盖软骨块支撑材料;3E.应用头部断层皮片覆盖筋膜并封闭创面后即刻;3F.对耳后供皮区创面进行打包固定

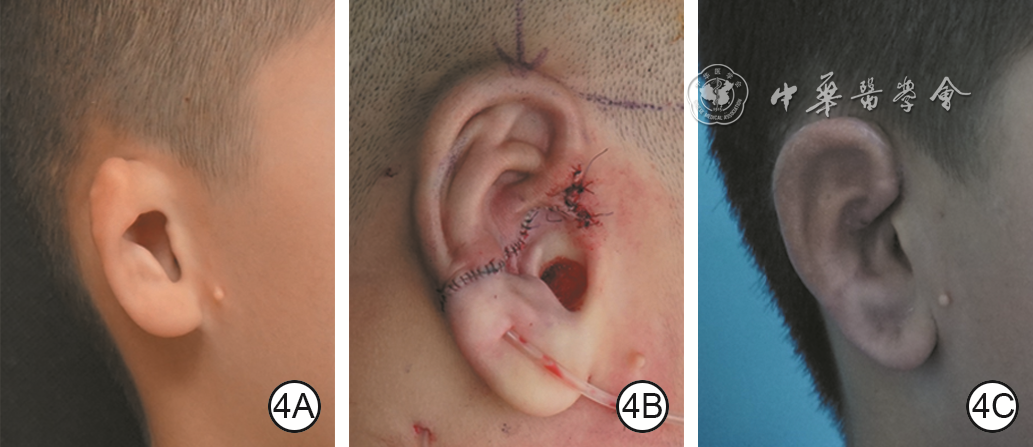
图 6 应用自体肋软骨行二期法全耳再造术矫正例3患者右侧腊肠型先天性小耳畸形的效果。6A.术前残耳侧面观;6B.Ⅰ期术后即刻;6C.Ⅱ期术后11年随访时残耳侧面观;6D.Ⅱ期术后11年随访时患者仰头,可见两耳对称;6E.Ⅱ期术后11年随访时残耳背侧面观
Table 1. 应用自体肋软骨行二期法全耳再造术矫正3 050例患者先天性小耳畸形术后并发症相关情况
发生时间 例数 类型 原因 处理措施 Ⅰ期术后 61 静脉回流障碍 皮瓣分离不均匀、皮下蒂位置不佳 针刺放血+用肝素溶液浸润的纱布湿敷、高压氧治疗 42 皮瓣坏死或软骨外露 支架边缘锐利、亚单位结构过于凸显、皮瓣分离不均匀、皮下蒂位置不佳 清创、应用筋膜瓣+皮片移植修复、高压氧治疗 31 血肿 止血不彻底、麻醉苏醒延迟 清创引流、加压包扎、高压氧治疗 31 钢丝外露 钢丝直径较粗 随访时或Ⅱ期术中去除外露钢丝 20 支架变形 钙化软骨处理不当、感染、睡姿不当、两期手术间隔时间过长 手术修复 16 感染(易发生于有外耳道的患者) 无菌操作和抗生素应用不规范 清创引流、合理应用抗生素、高压氧治疗 Ⅱ期术后 106 瘢痕增生 个人或家族史、皮肤张力过大、创面并发症处理不及时、预防和治疗措施不规范 定期随访并进行及时处理、瘢痕综合治疗、手术修复 97 部分皮片坏死 止血不彻底、打包压力不均匀、引流不充分、筋膜瓣血运不佳 对症换药、高压氧治疗 38 筋膜瓣坏死或软骨外露 支架背侧过于锐利、打包压力过大、筋膜瓣血运不佳 清创、应用颞浅筋膜瓣+皮片移植修复、高压氧治疗 26 支撑材料外露 筋膜瓣坏死、感染、打包固定不佳、睡姿不当、外力创伤 去除支撑材料、手术修复 13 感染(易发生于应用人工支撑材料的患者) 无菌操作和抗生素应用不规范 清创引流、合理应用抗生素、高压氧治疗 注:手术修复指根据并发症情况进行的切除部分软骨+封闭创面、应用筋膜瓣+皮片移植等手术  下载: 导出CSV
下载: 导出CSV
-

 下载:
下载:







计量
- 文章访问数: 1772
- HTML全文浏览量: 971
- PDF下载量: 21
- 被引次数: 0
