




-
摘要:
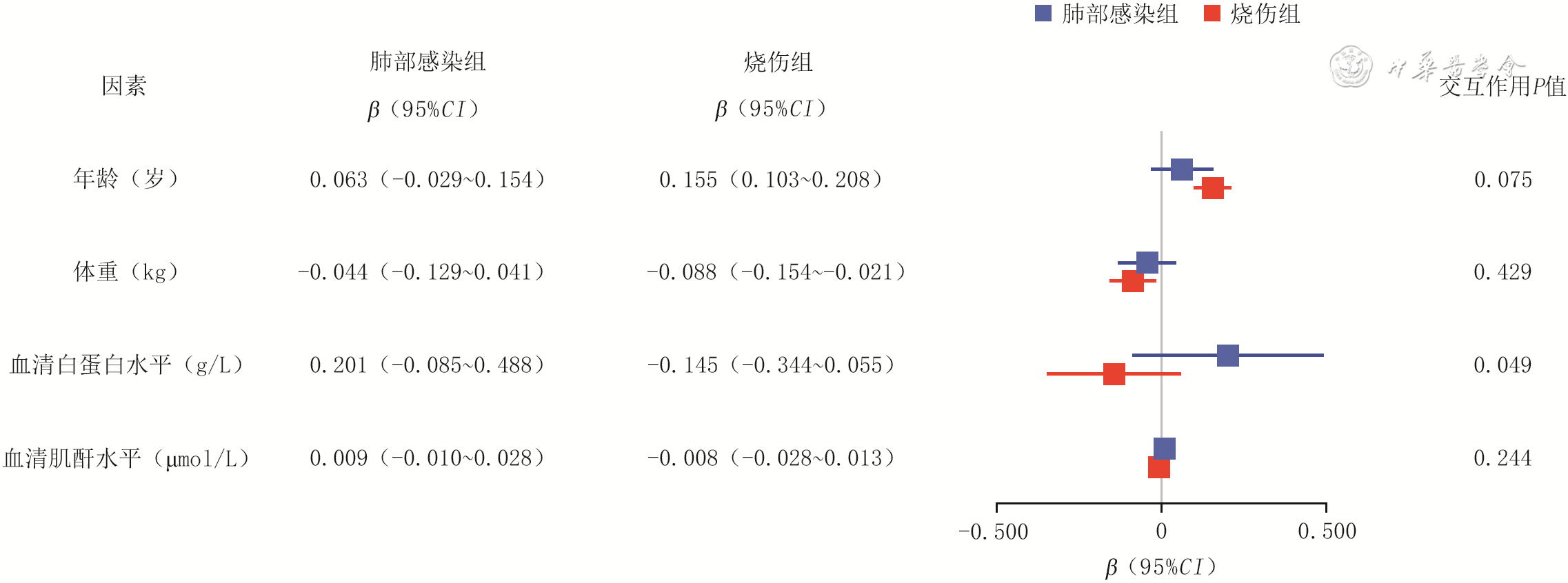
目的 探讨利奈唑胺在烧伤患者中的药代动力学特点及其影响因素。 方法 该研究为回顾性队列研究。将2024年8月1日—2025年8月1日上海交通大学医学院附属瑞金医院烧伤整形与创面修复科收治的按标准给药方案行利奈唑胺治疗(每12小时1次,每次600 mg)且完成利奈唑胺血药谷浓度(以下简称血药谷浓度)检测的74例(共行81次血药谷浓度检测)烧伤患者作为烧伤组,其中男22例、女52例,年龄16~87岁。将同期该院重症医学科收治的肺部感染患者中接受相同方案利奈唑胺治疗且完成血药谷浓度检测的74例患者(共行75次血药谷浓度检测)作为肺部感染组,其中男51例、女23例,年龄23~90岁。于第5次给药前30 min,采用液相色谱-串联质谱法检测2组患者血药谷浓度。分析烧伤组患者血药谷浓度与年龄、体重、烧伤总面积、Ⅲ度烧伤面积、伤后入院时间、血清白蛋白水平、血清肌酐水平及肌酐清除率之间的相关性,分析肺部感染组患者血药谷浓度与年龄、体重、血清白蛋白水平、血清肌酐水平及肌酐清除率之间的相关性。分析2组患者血药谷浓度与年龄、体重、血清白蛋白水平、血清肌酐水平的交互作用。 结果 烧伤组患者血药谷浓度为2.30(0.65,5.70)mg/L,明显低于肺部感染组的4.07(2.01,7.82)mg/L(Z=-3.131,P<0.05)。烧伤组患者中血药谷浓度<2 mg/L的比例达46.91%(38/81),明显高于肺部感染组的22.67%(17/75),χ2=10.030,P<0.05。烧伤组患者血药谷浓度与年龄呈明显正相关(rs=0.483,P<0.05),与体重及Ⅲ度烧伤面积均呈明显负相关(rs值分别为-0.247、-0.231,P<0.05)。肺部感染组患者血药谷浓度与肌酐清除率呈明显负相关(rs=-0.344,P<0.05),与血清肌酐水平呈明显正相关(rs=0.255,P<0.05)。肺部感染组和烧伤组患者血药谷浓度均仅与血清白蛋白水平存在明显交互作用(β值分别为0.201、-0.145,95%CI分别为-0.085~0.488、-0.344~0.055,P<0.05)。 结论 在利奈唑胺标准给药方案下,烧伤患者血药谷浓度较肺部感染患者显著降低且低血药暴露比例更高。烧伤患者血药谷浓度与年龄、体重及Ⅲ度烧伤面积相关,烧伤患者和肺部感染患者血药谷浓度均与血清白蛋白水平存在明显交互作用。 Abstract:Objective To explore the pharmacokinetic characteristic of linezolid in burn patients and its influencing factors. Methods This study was a retrospective cohort study. From August 1st, 2024 to August 1st, 2025, 74 burn patients who were admitted to the Department of Burn of Ruijin Hospital of Shanghai Jiao Tong University School of Medicine, received linezolid treatment under the standard dosing regimen of 600 mg every 12 hours, and completed monitoring of plasma trough concentration of linezolid (hereinafter referred to as plasma trough concentration), were included as burn group, including 22 males and 52 females, aged 16-87 years, with a total of 81 plasma trough concentration measurements. During the same period, 74 patients with pulmonary infection who were admitted to the Department of Critical Care Medicine of the same hospital, received the same linezolid treatment, and completed monitoring of plasma trough concentration, were included as pulmonary infection group, including 51 males and 23 females, aged 23-90 years, with a total of 75 plasma trough concentration measurements. The plasma trough concentrations of patients in two groups were detected at 30 min before the fifth administration using liquid chromatography-tandem mass spectrometry. In burn group of patients, the correlations between the plasma trough concentration and age, body weight, total burn area, full-thickness burn area, admission time after burn, serum albumin level, serum creatinine level, and creatinine clearance rate were analyzed. In pulmonary infection group of patients, the correlations between the plasma trough concentration and age, body weight, serum albumin level, serum creatinine level, and creatinine clearance rate were analyzed. The interaction of plasma trough concentration with age, body weight, serum albumin level, and serum creatinine level in two groups of patients were analyzed. Results The plasma trough concentration in burn group of patients was 2.30 (0.65, 5.70) mg/L, which was significantly lower than 4.07 (2.01, 7.82) mg/L in pulmonary infection group (Z=-3.131, P<0.05). The proportion with plasma trough concentration <2 mg/L in burn group of patients was 46.91% (38/81), which was significantly higher than 22.67% (17/75) in pulmonary infection group (χ²=10.030, P<0.05). In burn group of patients, the plasma trough concentration was significantly positively correlated with age (rs=0.483, P<0.05), and significantly negatively correlated with body weight and full-thickness burn area (with rs values of -0.247 and -0.231, respectively, P<0.05). In pulmonary infection group of patients, the plasma trough concentration was significantly negatively correlated with creatinine clearance rate (rs=-0.344, P<0.05), and significantly positively correlated with serum creatinine level (rs=0.255, P<0.05). In both pulmonary infection group and burn group of patients, the plasma trough concentration showed a significant interaction with the serum albumin level (with β values of 0.201 and -0.145, respectively, 95%CI of -0.085 to 0.488 and -0.344 to 0.055, respectively, P<0.05). Conclusions Under the standard dosing regimen of linezolid, the plasma trough concentration in patients with burns was significantly lower than that in patients with pulmonary infection, and the proportion of low drug exposure was higher. In patients with burns, the plasma trough concentration was correlated with age, body weight, and full-thickness burn area. The plasma trough concentration in both patients with burns and patients with pulmonary infection showed a significant interaction with the serum albumin level. -
Key words:
- Burns /
- Pharmacokinetics /
- Linezolid /
- Plasma trough concentration /
- Precision medication
-
参考文献
(40) [1] ShaoJL,ZhuYQ,XieMS,et al.Assessing the global burns burden in the context of the WHO prevention and care strategy: insights from the Global Burden of Disease study 2021[J].Nurs Health Sci,2026,28(2):e70329.DOI: 10.1111/nhs.70329. [2] MustehsanMA,BodlaMA,ShehzadMM,et al.Health-related quality of life in burn survivors from low-and middle-income countries: a systematic review and targeted comparative analysis of rehabilitation interventions[J].Burns,2026,52(4):107962.DOI: 10.1016/j.burns.2026.107962. [3] ŻwierełłoW,PiorunK,Skórka-MajewiczM,et al.Burns: classification, pathophysiology, and treatment: a review[J].Int J Mol Sci,2023,24(4):3749.DOI: 10.3390/ijms24043749. [4] MuellerSW, GibsonC, WiktorAJ. 510 antibiotic serum concentrations in burn patients with augmented renal clearance and adjusted regimens[J]. J Burn Care Res, 2024, 45(Supplement_1): S118. DOI: 10.1093/jbcr/irae036.145. [5] UdyAA,RobertsJA,LipmanJ,et al.The effects of major burn related pathophysiological changes on the pharmacokinetics and pharmacodynamics of drug use: an appraisal utilizing antibiotics[J].Adv Drug Deliv Rev,2018,123:65-74.DOI: 10.1016/j.addr.2017.09.019. [6] MatsunoVK,CamposEV,Silva JuniorEMD,et al.Changes in fluconazole pharmacokinetics can impact on antifungal effectiveness in critically ill burn patients: a pharmacokinetic-pharmacodynamic (PK/PD) approach[J].Clinics (Sao Paulo),2024,79:100491.DOI: 10.1016/j.clinsp.2024.100491. [7] AlharthiAF,Al SulaimanK,AlotaibiS,et al.Managing infections in burn patients: strategies and considerations for antimicrobial dosing[J].Eur Burn J,2025,6(4):53.DOI: 10.3390/ebj6040053. [8] HallRG,HooperL,DissanaikeS,et al.Pharmacokinetics of ceftolozane/tazobactam in patients with partial- and full-thickness skin burns[J].Pharmacotherapy,2025,45(11):774-779.DOI: 10.1002/phar.70076. [9] YangJ,LiuF,ZhaoY,et al.Population pharmacokinetics and dosing optimisation of polymyxin B in patients with severe burns[J].Burns,2025,51(9):107696.DOI: 10.1016/j.burns.2025.107696. [10] AzzouzA, PreussCV. Linezolid[M/OL]. Treasure Island (FL): StatPearls Publishing, 2024[2025-10-28]. https://pubmed.ncbi.nlm.nih.gov/30969615/. https://pubmed.ncbi.nlm.nih.gov/30969615/ [11] HashemianSMR,FarhadiT,GanjparvarM.Linezolid: a review of its properties, function, and use in critical care[J].Drug Des Devel Ther,2018,12:1759-1767.DOI: 10.2147/DDDT.S164515. [12] 苟军强,李倩,尹东锋,等. 利奈唑胺相关血液及代谢系统不良反应研究进展[J]. 解放军医学杂志,2024,49(8):965-972. DOI: 10.11855/j.issn.0577-7402.1083.2024.0124. [13] LaarhuisSRE,KerskesCHM,NijzielMR,et al.Linezolid-induced thrombocytopenia in patients with renal impairment: a case series, review and dose advice[J].Drugs R D,2024,24(1):109-115.DOI: 10.1007/s40268-024-00458-6. [14] GüntherS, ReimerA, VoglH, et al. Therapeutic drug monitoring of linezolid: HPLC-based assays for routine quantification of linezolid in human serum and cerebrospinal fluid[J]. Eur J Hosp Pharm, 2023, 30(6):353-358. DOI: 10.1136/ejhpharm-2021-003036. [15] LiuL,ZhangL,ZhengX,et al.LC-MS/MS-based multiplex antibacterial platform for therapeutic drug monitoring in intensive care unit patients[J].Front Pharmacol,2023,14:1116071.DOI: 10.3389/fphar.2023.1116071. [16] 刘瑾瑶,李文艳,董婧. 生物样本中利奈唑胺浓度测定方法及在治疗药物监测中应用的研究进展[J]. 中国临床药学杂志,2025,34(2):154-160. DOI: 10.19577/j.1007-4406.2025.02.016. [17] 张献朝,王雪剑,张明伟.临床应用Ccockcroft-Gault公式计算肌酐清除率判断肾功能状态的可行性研究[J].中原医刊,2004,36(6):1-2.DOI: 10.3760/cma.j.issn.1674-4756.2004.06.001. [18] WulkersdorferB,BergmannF,AmannL,et al.Effect of albumin substitution on pharmacokinetics of piperacillin/tazobactam in patients with severe burn injury admitted to the ICU[J].J Antimicrob Chemother,2024,79(2):262-270.DOI: 10.1093/jac/dkad368. [19] BlanchetB,JullienV,VinsonneauC,et al.Influence of burns on pharmacokinetics and pharmacodynamics of drugs used in the care of burn patients[J].Clin Pharmacokinet,2008,47(10):635-654.DOI: 10.2165/00003088-200847100-00002. [20] TedescoDJ,HutterMF,KhalafF,et al.Sex- and age-related differences in post-burn pathophysiology[J].Crit Care Med,2025,53(10):e1941-e1951.DOI: 10.1097/CCM.0000000000006789. [21] 毕昱,洪曦菲,汪健蕾,等.重症患者发生肾功能亢进的危险因素分析[J].转化医学杂志,2025,14(1):88-93. DOI: 10.3639/i.issn.2095-3097.2025.01.019. [22] 席宇菁,隋龙,陆徽,等. 重症感染及严重创伤患者肾功能亢进危险因素分析[J]. 中国药业,2024,33(18):90-93. DOI: 10.3969/j.issn.1006-4931.2024.18.021. [23] 史景泉,陈意生.我国烧伤病理学研究的回顾与展望[J].中华烧伤杂志,2008,24(5):323-324,327. DOI: 10.3760/cma.j.issn.1009-2587.2008.05.002. [24] LiuJ,PangY,LiW,et al.Impact of hepatic impairment and renal failure on the pharmacokinetics of linezolid and its metabolites: contribution of hepatic metabolism and renal excretion[J].Antimicrob Agents Chemother,2025,69(5):e0189224.DOI: 10.1128/aac.01892-24. [25] 邱红玉,荣礼,谢梦圆,等.基于群体药动学的利奈唑胺个体化给药研究进展[J].中国药房,2023,34(5):636-640.DOI: 10.6039/j.issn.1001-0408.2023.05.23. [26] HeidariS,KhaliliH.Linezolid pharmacokinetics: a systematic review for the best clinical practice[J].Eur J Clin Pharmacol,2023,79(2):195-206.DOI: 10.1007/s00228-022-03446-4. [27] AgliardiS,BrunoniB,GazzanigaG,et al.Linezolid serum concentration variability among critically ill patients based on renal function and continuous renal replacement therapy administration[J].Antibiotics (Basel),2025,14(12):1188.DOI: 10.3390/antibiotics14121188. [28] HuiLA,BodoleaC,VlaseL,et al.Linezolid administration to critically ill patients: intermittent or continuous infusion? A systematic literature search and review[J].Antibiotics (Basel),2022,11(4):436.DOI: 10.3390/antibiotics11040436. [29] ZollerM,MaierB,HornussC,et al.Variability of linezolid concentrations after standard dosing in critically ill patients: a prospective observational study[J].Crit Care,2014,18(4):R148.DOI: 10.1186/cc13984. [30] HillDM,YangB,LaizureSC,et al.Pharmacokinetic analysis of intravenous push cefepime in burn patients with augmented renal clearance[J].J Burn Care Res,2024,45(1):151-157.DOI: 10.1093/jbcr/irad134. [31] 周冉,张圣雨,沈爱宗.肾功能亢进在危重症患者中的研究进展[J].中国医院药学杂志,2019,39(19):2009-2013.DOI: 10.13286/j.cnki.chinhosppharmacyj.2019.19.20. [32] SilvaCM,BaptistaJP,SantosI,et al.Recommended antibiotic dosage regimens in critically ill patients with augmented renal clearance: a systematic review[J].Int J Antimicrob Agents,2022,59(5):106569.DOI: 10.1016/j.ijantimicag.2022.106569. [33] QinY,ZhangLL,YeYR,et al.Parametric population pharmacokinetics of linezolid: a systematic review[J].Br J Clin Pharmacol,2022,88(9):4043-4066.DOI: 10.1111/bcp.15368. [34] MonogueML,SandersJM,MercuroNJ,et al.Antimicrobial pharmacokinetic and pharmacodynamic considerations in special populations: a call to action[J].Open Forum Infect Dis,2026,13(3):ofag093.DOI: 10.1093/ofid/ofag093. [35] SteeleAN,GrimsrudKN,SenS,et al.Gap analysis of pharmacokinetics and pharmacodynamics in burn patients: a review[J].J Burn Care Res,2015,36(3):e194-211.DOI: 10.1097/BCR.0000000000000120. [36] KnuthCM,AugerC,JeschkeMG.Burn-induced hypermetabolism and skeletal muscle dysfunction[J].Am J Physiol Cell Physiol,2021,321(1):C58-C71.DOI: 10.1152/ajpcell.00106.2021. [37] NunezJH,ClarkAT.Burn patient metabolism and nutrition[J].Phys Med Rehabil Clin N Am,2023,34(4):717-731.DOI: 10.1016/j.pmr.2023.06.001. [38] RousseauAF,PantetO,HeylandDK.Nutrition after severe burn injury[J].Curr Opin Clin Nutr Metab Care,2023,26(2):99-104.DOI: 10.1097/MCO.0000000000000904. [39] BhandariRK,RohillaR,ShafiqN,et al.Clinical pharmacokinetics of antimicrobials in critical care: a narrative review[J].Expert Rev Anti Infect Ther,2024,22(11):951-964.DOI: 10.1080/14787210.2024.2406466. [40] MoklineA, GharsallahL, RahmaniI, et al. Pharmacokinetics and pharmacodynamics of linezolid in burn patients[J]. Ann Burns Fire Disasters, 2018,31(2):118-121. -

图 1 2组患者利奈唑胺血药谷浓度与其影响因素的交互作用森林图
注:肺部感染组74例患者共进行75次血药谷浓度检测,烧伤组74例患者共进行81次血药谷浓度检测;于利奈唑胺第5次给药前30 min检测血药谷浓度及血清肌酐、白蛋白水平
Table 1. 2组行利奈唑胺治疗的患者的一般资料比较[M(Q1,Q3)]
组别 例数 年龄(岁) 体重(kg) 肌酐清除率(mL/min) 血清肌酐水平(μmol/L) 血清白蛋白水平(g/L) 烧伤组 74 45.5(34.0,60.0) 66.0(59.3,75.8) 64.00(51.50,95.42) 102.00(67.39,140.28) 33.00(30.00,37.50) 肺部感染组 74 72.0(63.8,81.0) 61.0(50.0,70.0) 79.42(39.90,105.52) 71.00(50.00,98.00) 31.00(28.00,33.00) Z值 -6.805 -2.872 -0.625 -3.340 -4.011 P值 <0.001 0.004 0.532 <0.001 <0.001 注:烧伤组患者共进行81次检测,肺部感染者组患者共进行75次检测;于利奈唑胺第5次给药前30 min检测血清肌酐、白蛋白水平并计算肌酐清除率  下载: 导出CSV
下载: 导出CSV
Table 2. 2组患者利奈唑胺血药谷浓度分布[例(%)]
组别 例次 <2 mg/L 2~8 mg/L >8 mg/L 烧伤组 81 38(46.91) 28(34.57) 15(18.52) 肺部感染组 75 17(22.67) 43(57.33) 15(20.00) 注:于利奈唑胺第5次给药前30 min检测血药谷浓度
下载: 导出CSV
Table 3. 烧伤组患者利奈唑胺血药谷浓度与其影响因素之间的相关性
影响因素 rs值 P值 年龄(岁) 0.483 <0.001 体重(kg) -0.247 0.026 烧伤总面积(%TBSA) -0.177 0.114 Ⅲ度烧伤面积(%TBSA) -0.231 0.038 伤后入院时间(d) 0.100 0.374 血清白蛋白水平(g/L) -0.151 0.178 血清肌酐水平(μmol/L) -0.139 0.217 肌酐清除率(mL/min) -0.151 0.179 注:74例患者共进行81次血药谷浓度检测;于利奈唑胺第5次给药前30 min检测血药谷浓度及血清肌酐、白蛋白水平并计算肌酐清除率;TBSA为体表总面积
下载: 导出CSV
Table 4. 肺部感染组患者利奈唑胺血药谷浓度与其影响因素之间的相关性
影响因素 rs值 P值 年龄(岁) 0.225 0.052 体重(kg) -0.130 0.267 血清白蛋白水平(g/L) 0.164 0.159 血清肌酐水平(μmol/L) 0.255 0.027 肌酐清除率(mL/min) -0.344 0.002 注:74例患者共进行75次血药谷浓度检测;于利奈唑胺第5次给药前30 min检测血药谷浓度及血清肌酐、白蛋白水平并计算肌酐清除率
下载: 导出CSV
-

 下载:
下载:

图(2) / 表(4)
计量
- 文章访问数: 261
- HTML全文浏览量: 189
- PDF下载量: 11
- 被引次数: 0
