




Two-sample Mendelian randomization analysis of the causal relationship between human immune cell phenotypes and keloids
-
摘要:
目的 探讨人免疫细胞表型与瘢痕疙瘩之间的因果关系。 方法 该研究为基于双样本孟德尔随机化(MR)分析的研究。以人免疫细胞表型为暴露因素,以瘢痕疙瘩为结局,从全基因组关联分析数据库中获取免疫细胞表型(3 757个样本)与瘢痕疙瘩(668个样本)的数据。将与免疫细胞表型显著相关的单核苷酸多态性(SNP)作为工具变量并排除弱工具变量的影响,应用双样本MR分析评估731种人免疫细胞表型与瘢痕疙瘩之间的因果关系。采用逆方差加权(IVW)法推断因果关系,使用MR-Egger法、加权模式法和加权中位数法进行验证。针对符合假设的免疫细胞表型SNP,利用Cochran Q检验评估异质性,利用MR-Egger回归检验及MR-PRESSO离群值检验评估水平多效性。 结果 筛选出18 204个达到显著阈值(P<1×10-5)的SNP作为代表731种免疫细胞表型的工具变量,这些SNP均不是弱工具变量(F值均>10)。根据IVW法,确定了21种与瘢痕疙瘩存在潜在因果关系的免疫细胞表型,其中CD62L-单核细胞绝对计数、初始-成熟B细胞上的CD19表达、IgD+B细胞上的CD19表达、浆细胞前体(浆母细胞)上的CD27表达、CD62L+髓系树突状细胞上的CD86表达、自然杀伤T细胞上的CD45表达、CD39+CD4+调节性T细胞上的CD25表达、来源于单核髓系的抑制细胞上的CD45表达、效应记忆CD8+T细胞上的CD8表达、静息CD4+调节性T细胞上的CD45RA表达与瘢痕疙瘩均呈显著正相关(比值比分别为1.12、1.09、1.08、1.21、1.13、1.12、1.17、1.11、1.10、1.07,95%置信区间分别为1.03~1.23、1.02~1.16、1.01~1.15、1.06~1.38、1.02~1.25、1.01~1.24、1.03~1.33、1.00~1.23、1.00~1.20、1.01~1.13,P<0.05),激活并分泌的CD4+调节性T细胞绝对计数、未转换记忆B细胞上的CD25表达、浆细胞样树突状细胞绝对计数、来源于单核髓系的抑制细胞上的CD14表达、自然杀伤T细胞上的CD8表达、IgD+CD38+B细胞上的CD20表达、CD11c+CD62L-单核细胞绝对计数、CD66b++髓系细胞绝对计数、粒细胞上的CD11c表达、CD14+CD16+单核细胞上的CD14表达、中心记忆CD8+T细胞上的CD3表达与瘢痕疙瘩均呈显著负相关(比值比分别为0.95、0.93、0.93、0.93、0.91、0.89、0.89、0.88、0.87、0.86、0.85,95%置信区间分别为0.90~1.00、0.87~0.99、0.88~0.99、0.87~0.99、0.84~1.00、0.81~0.98、0.81~0.98、0.79~0.99、0.78~0.96、0.75~0.99、0.74~0.96,P<0.05)。经MR-Egger法验证,CD39+CD4+调节性T细胞上的CD25表达、CD62L+髓系树突状细胞上的CD86表达、IgD+B细胞上的CD19表达、静息CD4+调节性T细胞上的CD45RA表达、中心记忆CD8+T细胞上的CD3表达与瘢痕疙瘩存在潜在因果关系(比值比分别为1.32、1.22、1.11、1.09、0.73,95%置信区间分别为1.03~1.70、1.04~1.44、1.02~1.21、1.01~1.19、0.55~0.95,P<0.05);经加权中位数法验证,自然杀伤T细胞上的CD45表达、激活并分泌的CD4+调节性T细胞绝对计数、IgD+CD38+B细胞上的CD20表达、CD66b++髓系细胞绝对计数与瘢痕疙瘩存在潜在因果关系(比值比分别为1.15、0.93、0.87、0.83,95%置信区间分别为1.01~1.31、0.86~1.00、0.77~0.98、0.71~0.96,P<0.05),其中IgD+CD38+B细胞上的CD20表达与瘢痕疙瘩的潜在因果关系另得到加权模式法的验证(比值比为0.86,95%置信区间为0.77~0.97,P<0.05)。根据前述IVW法分析结果,评估显示,与瘢痕疙瘩存在显著因果关系的21种免疫细胞表型的SNP均不存在显著异质性(P>0.05)或显著水平多效性(P>0.05)。 结论 从遗传学角度揭示了21种人免疫细胞表型和瘢痕疙瘩之间存在潜在因果关系,其中10种免疫细胞表型可能是瘢痕疙瘩的危险因素,11种免疫细胞表型可能是瘢痕疙瘩的保护因素。 Abstract:Objective To explore the causal relationship between human immune cell phenotypes and keloids. Methods This study was based on a two-sample Mendelian randomization (MR) analysis. Human immune cell phenotypes were considered as the exposure factors, and keloid was the outcome. Data on immune cell phenotypes (3 757 samples) and keloids (668 samples) were obtained from the genome-wide association study database. Using single nucleotide polymorphisms (SNPs) significantly associated with immune cell phenotypes as instrumental variables with the influence of weak instrumental variables being excluded, two-sample MR analysis was employed to evaluate the causal relationship between 731 human immune cell phenotypes and keloids. The inverse variance weighted (IVW) method was used to infer causal relationships, and the MR-Egger, weighted median, and weighted mode methods were used for validation. For SNPs of immune cell phenotypes meeting the hypothesis, the Cochran Q test was used to assess heterogeneity, and the MR-Egger regression and MR-PRESSO outlier tests were used to evaluate horizontal pleiotropy. Results A total of 18 204 SNPs meeting the significant threshold (P<1×10⁻⁵) were selected as instrumental variables for 731 immune cell phenotypes, and none of these SNPs were weak instrumental variables (with F values all >10). According to the IVW method, 21 immune cell phenotypes were identified with potential causal relationships to keloids, among which the CD62L- monocyte absolute count, CD19 on naive-mature B cell, CD19 on IgD+ B cell, CD27 on plasma blast-plasma cell, CD86 on CD62L+ myeloid dendritic cell, CD45 on natural killer T cell, CD25 on CD39+ CD4+ regulatory T cell, CD45 on monocytic myeloid-derived suppressor cells, CD8 on effector memory CD8+ T cell, and CD45RA on resting CD4+ regulatory T cell showed significant positive correlations with keloids (with odds ratios of 1.12, 1.09, 1.08, 1.21, 1.13, 1.12, 1.17, 1.11, 1.10, and 1.07, respectively, 95% confidence intervals of 1.03-1.23, 1.02-1.16, 1.01-1.15, 1.06-1.38, 1.02-1.25, 1.01-1.24, 1.03-1.33, 1.00-1.23, 1.00-1.20, and 1.01-1.13, respectively, P<0.05), while the activated and secreted CD4+ regulatory T cell absolute count, CD25 on unswitched memory B cell, plasmacytoid dendritic cell absolute count, CD14 on monocytic myeloid-derived suppressor cells, CD8 on natural killer T cell, CD20 on IgD+ CD38+ B cell, CD11c+ CD62L- monocyte absolute count, CD66b++ myeloid cell absolute count, CD11c on granulocytes, CD14 on CD14+ CD16+ monocyte, and CD3 on central memory CD8+ T cell showed significant negative correlations with keloids (with odds ratios of 0.95, 0.93, 0.93, 0.93, 0.91, 0.89, 0.89, 0.88, 0.87, 0.86, and 0.85, respectively, 95% confidence intervals of 0.90-1.00, 0.87-0.99, 0.88-0.99, 0.87-0.99, 0.84-1.00, 0.81-0.98, 0.81-0.98, 0.79-0.99, 0.78-0.96, 0.75-0.99, and 0.74-0.96, respectively, P<0.05). MR-Egger method confirmed the potential causal relationship existing respectively between CD25 on CD39+ CD4+ regulatory T cell, CD86 on CD62L+ myeloid dendritic cell, CD19 on IgD+ B cell, CD45RA on resting CD4+ regulatory T cell, CD3 on central memory CD8+ T cell and keloids (with odds ratios of 1.32, 1.22, 1.11, 1.09, and 0.73, respectively, 95% confidence intervals of 1.03-1.70, 1.04-1.44, 1.02-1.21, 1.01-1.19, and 0.55-0.95, respectively, P<0.05). The weighted median method confirmed the potential causal relationship existing respectively between CD45 on natural killer T cell, activated and secreted CD4+ regulatory T cells absolute count, CD20 on IgD+ CD38+ B cell, CD66b++ myeloid cell absolute count and keloids (with odds ratios of 1.15, 0.93, 0.87, and 0.83, respectively, 95% confidence intervals of 1.01-1.31, 0.86-1.00, 0.77-0.98, and 0.71-0.96, respectively, P<0.05). Among them, the potential causal relationship between CD20 on IgD+ CD38+ B cell and keloids was further verified by the weighted mode method (with odds ratio of 0.86, 95% confidence interval of 0.77-0.97, P<0.05). According to the aforementioned IVW method analysis results, the SNPs associated with the 21 immune cell phenotypes that had a significant causal relationship with keloids showed no significant heterogeneity (P>0.05) or significant horizontal pleiotropy (P>0.05). Conclusions From a genetic perspective, the potential causal relationships between 21 human immune cell phenotypes and keloids have been revealed, of which 10 immune cell phenotypes may be risk factors for keloids, while 11 immune cell phenotypes may act as protective factors for keloids. -
Key words:
- Keloid /
- Immunity, cellular /
- Mendelian randomization analysis /
- Immune system /
- Databases, genetic /
- Causality
-
参考文献
(40) [1] 雷继安,周圆,秦泽莲.炎症反应参与瘢痕疙瘩形成的研究进展[J].中华烧伤杂志,2021,37(6):591-595.DOI: 10.3760/cma.j.cn501120-20200312-00154. [2] OgawaR,AkitaS,AkaishiS,et al.Diagnosis and treatment of keloids and hypertrophic scars-Japan Scar Workshop consensus document 2018[J/OL].Burns Trauma,2019,7:39[2023-11-30]. https://pubmed.ncbi.nlm.nih.gov/31890718/.DOI: 10.1186/s41038-019-0175-y. [3] 贾赤宇,陈泠西.瘢痕疙瘩的肿瘤特征[J].中华烧伤杂志,2021,37(4):301-305.DOI: 10.3760/cma.j.cn501120-20200529-00289. [4] WangZC,ZhaoWY,CaoY,et al.The roles of inflammation in keloid and hypertrophic scars[J].Front Immunol,2020,11:603187.DOI: 10.3389/fimmu.2020.603187. [5] LeeAR,LeeSY,ChoiJW,et al.Establishment of a humanized mouse model of keloid diseases following the migration of patient immune cells to the lesion: patient-derived keloid xenograft (PDKX) model[J].Exp Mol Med,2023,55(8):1713-1719.DOI: 10.1038/s12276-023-01045-6. [6] HellwegeJN,RussellSB,WilliamsSM,et al.Gene-based evaluation of low-frequency variation and genetically-predicted gene expression impacting risk of keloid formation[J].Ann Hum Genet,2018,82(4):206-215.DOI: 10.1111/ahg.12245. [7] YinX,BuW,FangF,et al.Keloid biomarkers and their correlation with immune infiltration[J].Front Genet,2022,13:784073.DOI: 10.3389/fgene.2022.784073. [8] XuH,ZhuZ,HuJ,et al.Downregulated cytotoxic CD8+ T-cell identifies with the NKG2A-soluble HLA-E axis as a predictive biomarker and potential therapeutic target in keloids[J].Cell Mol Immunol,2022,19(4):527-539.DOI: 10.1038/s41423-021-00834-1. [9] JinQ,GuiL,NiuF,et al.Macrophages in keloid are potent at promoting the differentiation and function of regulatory T cells[J].Exp Cell Res,2018,362(2):472-476.DOI: 10.1016/j.yexcr.2017.12.011. [10] LeeCC,TsaiCH,ChenCH,et al.An updated review of the immunological mechanisms of keloid scars[J].Front Immunol,2023,14:1117630.DOI: 10.3389/fimmu.2023.1117630. [11] DaviesNM,HolmesMV,Davey SmithG.Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians[J].BMJ,2018,362:k601.DOI: 10.1136/bmj.k601. [12] SandersonE,GlymourMM,HolmesMV,et al. Mendelian randomization[J].Nat Rev Methods Primers,2022,2:6.DOI: 10.1038/s43586-021-00092-5. [13] Gagliano TaliunSA,EvansDM.Ten simple rules for conducting a mendelian randomization study[J].PLoS Comput Biol,2021,17(8):e1009238.DOI: 10.1371/journal.pcbi.1009238. [14] OrrùV,SteriM,SidoreC,et al.Complex genetic signatures in immune cells underlie autoimmunity and inform therapy[J].Nat Genet,2020,52(10):1036-1045.DOI: 10.1038/s41588-020-0684-4. [15] SidoreC,BusoneroF,MaschioA,et al.Genome sequencing elucidates Sardinian genetic architecture and augments association analyses for lipid and blood inflammatory markers[J].Nat Genet,2015,47(11):1272-1281.DOI: 10.1038/ng.3368. [16] SakaueS,KanaiM,TanigawaY,et al.A cross-population atlas of genetic associations for 220 human phenotypes[J].Nat Genet,2021,53(10):1415-1424.DOI: 10.1038/s41588-021-00931-x. [17] LvX,HuZ,LiangF,et al.Causal relationship between ischemic stroke and its subtypes and frozen shoulder: a two-sample Mendelian randomization analysis[J].Front Neurol,2023,14:1178051.DOI: 10.3389/fneur.2023.1178051. [18] BurgessS,ThompsonSG,Genetics CollaborationCRP CHD.Avoiding bias from weak instruments in Mendelian randomization studies[J].Int J Epidemiol,2011,40(3):755-764.DOI: 10.1093/ije/dyr036. [19] BurgessS,ThompsonSG.Interpreting findings from Mendelian randomization using the MR-Egger method[J].Eur J Epidemiol,2017,32(5):377-389.DOI: 10.1007/s10654-017-0255-x. [20] GauglitzGG,KortingHC,PavicicT,et al.Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies[J].Mol Med,2011,17(1/2):113-125.DOI: 10.2119/molmed.2009.00153. [21] BurgessS,ButterworthA,ThompsonSG.Mendelian randomization analysis with multiple genetic variants using summarized data[J].Genet Epidemiol,2013,37(7):658-665.DOI: 10.1002/gepi.21758. [22] YangWY,ShaoY,Lopez-PastranaJ,et al.Pathological conditions re-shape physiological Tregs into pathological Tregs[J/OL].Burns Trauma,2015,3(1):1[2023-11-30].https://pubmed.ncbi.nlm.nih.gov/26623425/.DOI: 10.1186/s41038-015-0001-0. [23] MuraoN,SeinoK,HayashiT,et al.Treg-enriched CD4+ T cells attenuate collagen synthesis in keloid fibroblasts[J].Exp Dermatol,2014,23(4):266-271.DOI: 10.1111/exd.12368. [24] ShortWD,WangX,KeswaniSG.The role of T lymphocytes in cutaneous scarring[J].Adv Wound Care (New Rochelle),2022,11(3):121-131.DOI: 10.1089/wound.2021.0059. [25] ChenY,JinQ,FuX,et al.Connection between T regulatory cell enrichment and collagen deposition in keloid[J].Exp Cell Res,2019,383(2):111549.DOI: 10.1016/j.yexcr.2019.111549. [26] TianY,BaborM,LaneJ,et al.Unique phenotypes and clonal expansions of human CD4 effector memory T cells re-expressing CD45RA[J].Nat Commun,2017,8(1):1473.DOI: 10.1038/s41467-017-01728-5. [27] CheungJ,ZahorowskaB,SuranyiM,et al.CD4+CD25+ T regulatory cells in renal transplantation[J].Front Immunol,2022,13:1017683.DOI: 10.3389/fimmu.2022.1017683. [28] HarrisF,BerdugoYA,TreeT.IL-2-based approaches to Treg enhancement[J].Clin Exp Immunol,2023,211(2):149-163.DOI: 10.1093/cei/uxac105. [29] AbbasAK,TrottaE,Simeonov DR,et al.Revisiting IL-2: biology and therapeutic prospects[J].Sci Immunol,2018,3(25):eaat1482.DOI: 10.1126/sciimmunol.aat1482. [30] LykhopiyV,MalviyaV,Humblet-BaronS,et al.IL-2 immunotherapy for targeting regulatory T cells in autoimmunity[J].Genes Immun,2023,24(5):248-262.DOI: 10.1038/s41435-023-00221-y. [31] ShanM,LiuH,HaoY,et al.The role of CD28 and CD8+ T cells in keloid development[J].Int J Mol Sci,2022,23(16):8862.DOI: 10.3390/ijms23168862. [32] ChenZ,ZhouL,WonT,et al.Characterization of CD45RO+ memory T lymphocytes in keloid disease[J].Br J Dermatol,2018,178(4):940-950.DOI: 10.1111/bjd.16173. [33] TannoH,KawakamiK,KannoE,et al.Invariant NKT cells promote skin wound healing by preventing a prolonged neutrophilic inflammatory response[J].Wound Repair Regen,2017,25(5):805-815.DOI: 10.1111/wrr.12588. [34] SîrbulescuRF,BoehmCK,SoonE,et al.Mature B cells accelerate wound healing after acute and chronic diabetic skin lesions[J].Wound Repair Regen,2017,25(5):774-791.DOI: 10.1111/wrr.12584. [35] AndersonJB,HarrantAB,Navarro-AlvarezN,et al. 4371 The role of B cells in keloid formation[J]. J Clin Transl Sci,2020, 4(Suppl 1):S18-19. DOI: 10.1017/cts.2020.97. [36] ShanM,WangY.Viewing keloids within the immune microenvironment[J].Am J Transl Res,2022,14(2):718-727. [37] RathM,PitiotA,KirrM,et al.Multi-antigen imaging reveals inflammatory DC, ADAM17 and Neprilysin as effectors in keloid formation[J].Int J Mol Sci,2021,22(17):9417.DOI: 10.3390/ijms22179417. [38] CalventeCJ,TamedaM,JohnsonCD,et al.Neutrophils contribute to spontaneous resolution of liver inflammation and fibrosis via microRNA-223[J].J Clin Invest,2019,129(10):4091-4109.DOI: 10.1172/JCI122258. [39] SaijouE,EnomotoY,MatsudaM,et al.Neutrophils alleviate fibrosis in the CCl4-induced mouse chronic liver injury model[J].Hepatol Commun,2018,2(6):703-717.DOI: 10.1002/hep4.1178. [40] ShaoY,GuoZ,YangY,et al.Neutrophil extracellular traps contribute to myofibroblast differentiation and scar hyperplasia through the Toll-like receptor 9/nuclear factor Kappa-B/interleukin-6 pathway[J/OL].Burns Trauma,2022,10:tkac044[2023-11-30].https://pubmed.ncbi.nlm.nih.gov/36406661/.DOI: 10.1093/burnst/tkac044. -

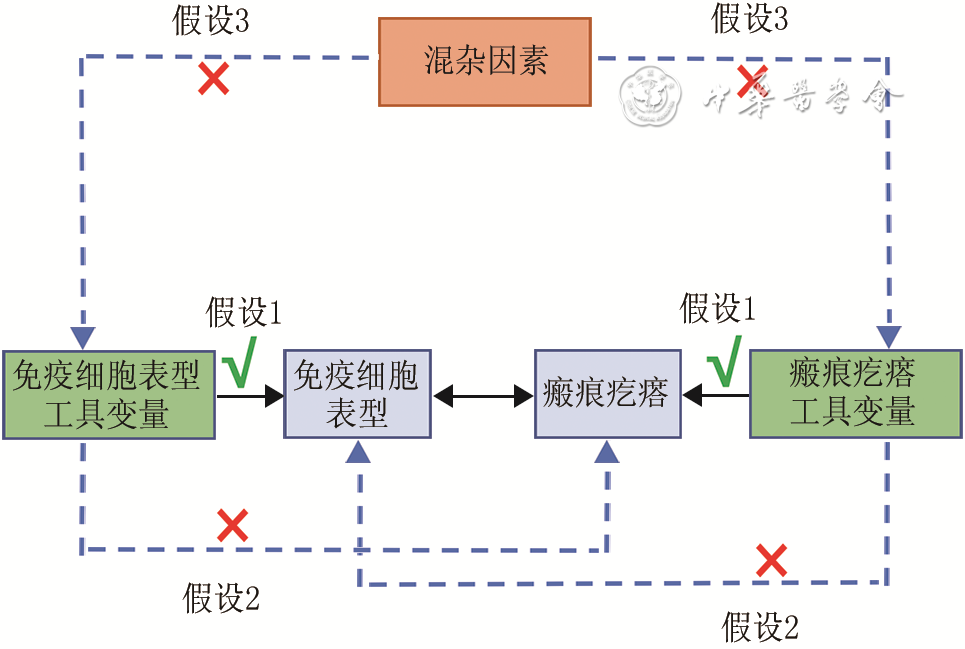
图 1 人免疫细胞表型与瘢痕疙瘩的正反向双样本孟德尔随机化分析核心假设及分析流程图
注:假设1为关联性假设,假设2为独立性假设,假设3为限定准则;图中“×”和虚线表示2个因子之间不产生作用,“✓”和实线表示2个因子之间可以产生作用;图中免疫细胞表型目前已知有731种
Table 1. 逆方差加权法分析得出21种人免疫细胞表型与瘢痕疙瘩存在潜在因果关系
免疫细胞表型 单核苷酸多态性数(个) 比值比 95%置信区间 P值 浆细胞前体(浆母细胞)上的CD27表达 19 1.21 1.06~1.38 0.006 CD39+CD4+调节性T细胞上的CD25表达 17 1.17 1.03~1.33 0.014 CD62L+髓系树突状细胞上的CD86表达 23 1.13 1.02~1.25 0.016 自然杀伤T细胞上的CD45表达 22 1.12 1.01~1.24 0.012 CD62L-单核细胞绝对计数 21 1.12 1.03~1.23 0.036 来源于单核髓系的抑制细胞上的CD45表达 17 1.11 1.00~1.23 0.047 效应记忆CD8+T细胞上的CD8表达 24 1.10 1.00~1.20 0.047 初始-成熟B细胞上的CD19表达 28 1.09 1.02~1.16 0.009 IgD+B细胞上的CD19表达 28 1.08 1.01~1.15 0.035 静息CD4+调节性T细胞上的CD45RA表达 29 1.07 1.01~1.13 0.023 激活并分泌的CD4+调节性T细胞绝对计数 23 0.95 0.90~1.00 0.036 未转换记忆B细胞上的CD25表达 24 0.93 0.87~0.99 0.029 浆细胞样树突状细胞绝对计数 30 0.93 0.88~0.99 0.021 来源于单核髓系的抑制细胞上的CD14表达 24 0.93 0.87~0.99 0.026 自然杀伤T细胞上的CD8表达 19 0.91 0.84~1.00 0.048 IgD+CD38+B细胞上的CD20表达 26 0.89 0.81~0.98 0.017 CD11c+CD62L-单核细胞绝对计数 25 0.89 0.81~0.98 0.016 CD66b++髓系细胞绝对计数 16 0.88 0.79~0.99 0.026 粒细胞上的CD11c表达 25 0.87 0.78~0.96 0.006 CD14+CD16+单核细胞上的CD14表达 17 0.86 0.75~0.99 0.036 中心记忆CD8+T细胞上的CD3表达 18 0.85 0.74~0.96 0.013  下载: 导出CSV
下载: 导出CSV
Table 2. 补充双样本MR分析方法得出9种人免疫细胞表型与瘢痕疙瘩存在潜在因果关系
分析方法与免疫细胞表型 单核苷酸多态性数(个) 比值比 95%置信区间 P值 MR-Egger法 CD39+CD4+调节性T细胞上的CD25表达 17 1.32 1.03~1.70 0.043 CD62L+髓系树突状细胞上的CD86表达 23 1.22 1.04~1.44 0.022 IgD+B细胞上的CD19表达 28 1.11 1.02~1.21 0.020 静息CD4+调节性T细胞上的CD45RA表达 29 1.09 1.01~1.19 0.041 中心记忆CD8+T细胞上的CD3表达 18 0.73 0.55~0.95 0.035 加权中位数法 自然杀伤T细胞上的CD45表达 22 1.15 1.01~1.31 0.030 激活并分泌的CD4+调节性T细胞绝对计数 23 0.93 0.86~1.00 0.039 IgD+CD38+B细胞上的CD20表达 26 0.87 0.77~0.98 0.026 CD66b++髓系细胞绝对计数 16 0.83 0.71~0.96 0.014 加权模式法 IgD+CD38+B细胞上的CD20表达 26 0.86 0.77~0.97 0.016 注:MR为孟德尔随机化
下载: 导出CSV
Table 3. 与瘢痕疙瘩存在显著因果关系的21种人免疫细胞表型SNP的异质性与水平多效性分析结果
免疫细胞表型 SNP数(个) Cochran Q检验 MR-Egger回归检验 MR-PRESSO离群值检验 Q值 P值 截距 P值 RSSobs P值 浆细胞前体(浆母细胞)上的CD27表达 19 10.24 0.924 0.019 0.424 11.66 0.927 CD39+CD4+调节性T细胞上的CD25表达 17 8.00 0.949 -0.031 0.285 9.30 0.946 CD62L+髓系树突状细胞上的CD86表达 23 21.73 0.476 -0.025 0.225 23.27 0.522 自然杀伤T细胞上的CD45表达 22 21.63 0.421 0.004 0.884 24.93 0.409 CD62L-单核细胞绝对计数 21 13.33 0.863 -0.011 0.565 14.25 0.887 来源于单核髓系的抑制细胞上的CD45表达 17 8.22 0.942 -0.006 0.858 9.05 0.943 效应记忆CD8+T细胞上的CD8表达 24 19.71 0.659 -0.022 0.316 20.81 0.696 初始-成熟B细胞上的CD19表达 28 29.50 0.337 0.005 0.797 32.20 0.356 IgD+B细胞上的CD19表达 28 25.83 0.528 -0.020 0.200 28.83 0.507 静息CD4+调节性T细胞上的CD45RA表达 29 21.40 0.808 -0.019 0.434 22.51 0.841 激活并分泌的CD4+调节性T细胞绝对计数 23 22.13 0.452 0.016 0.519 23.82 0.516 未转换记忆B细胞上的CD25表达 24 17.97 0.759 -0.015 0.333 19.20 0.790 浆细胞样树突状细胞绝对计数 30 36.26 0.166 0.001 0.955 38.83 0.217 来源于单核髓系的抑制细胞上的CD14表达 24 20.94 0.585 -0.016 0.492 21.99 0.648 自然杀伤T细胞上的CD8表达 19 19.02 0.390 -0.026 0.206 21.72 0.428 IgD+CD38+B细胞上的CD20表达 26 32.18 0.153 0.012 0.561 33.65 0.194 CD11c+CD62L-单核细胞绝对计数 25 14.78 0.927 -0.008 0.679 15.65 0.938 CD66b++髓系细胞绝对计数 16 10.26 0.803 -0.003 0.927 11.87 0.806 粒细胞上的CD11c表达 25 17.64 0.820 -0.016 0.481 18.73 0.843 CD14+CD16+单核细胞上的CD14表达 17 16.03 0.451 0.007 0.870 18.26 0.461 中心记忆CD8+T细胞上的CD3表达 18 15.39 0.568 0.036 0.231 16.99 0.620 注:SNP为单核苷酸多态性,MR为孟德尔随机化;Cochran Q检验评估异质性,另2种检验评估水平多效性
下载: 导出CSV
Table 4. 瘢痕疙瘩与21种人免疫细胞表型之间因果关系的逆方差加权法分析结果
免疫细胞表型 单核苷酸多态性数(个) 比值比 95%置信区间 P值 CD62L-单核细胞绝对计数 10 0.99 0.93~1.06 0.821 CD11c+CD62L-单核细胞绝对计数 10 0.98 0.91~1.05 0.495 浆细胞样树突状细胞绝对计数 20 0.99 0.95~1.04 0.789 激活并分泌的CD4+调节性T细胞绝对计数 16 1.01 0.96~1.05 0.778 CD66b++髓系细胞绝对计数 9 1.00 0.90~1.10 0.956 初始-成熟B细胞上的CD19表达 12 1.01 0.96~1.07 0.608 IgD+B细胞上的CD19表达 12 1.01 0.96~1.06 0.675 IgD+CD38+B细胞上的CD20表达 15 1.00 0.96~1.04 0.998 未转换记忆B细胞上的CD25表达 11 0.99 0.93~1.06 0.808 浆细胞前体(浆母细胞)上的CD27表达 13 1.00 0.95~1.04 0.910 中心记忆CD8+T细胞上的CD3表达 15 0.99 0.94~1.05 0.809 CD62L+髓系树突状细胞上的CD86表达 14 1.02 0.95~1.09 0.559 自然杀伤T细胞上的CD45表达 10 1.00 0.95~1.05 0.993 CD39+CD4+调节性T细胞上的CD25表达 12 1.00 0.94~1.06 0.918 CD14+CD16+单核细胞上的CD14表达 8 1.01 0.94~1.08 0.749 来源于单核髓系的抑制细胞上的CD14表达 8 1.01 0.92~1.10 0.891 来源于单核髓系的抑制细胞上的CD45表达 5 1.00 0.80~1.26 0.986 效应记忆CD8+T细胞上的CD8表达 13 1.00 0.94~1.07 0.965 自然杀伤T细胞上的CD8表达 10 1.01 0.92~1.10 0.871 粒细胞上的CD11c表达 7 0.99 0.93~1.06 0.785 静息CD4+调节性T细胞上的CD45RA表达 13 0.99 0.92~1.06 0.781
下载: 导出CSV
-

 下载:
下载:


图(2) / 表(4)
计量
- 文章访问数: 800
- HTML全文浏览量: 239
- PDF下载量: 14
- 被引次数: 0
