




Effects of medial plantar artery perforator flap transplantation in the reconstruction of palmar scar contracture
-
摘要:
目的 探讨足底内侧动脉穿支皮瓣移植整复手部掌侧瘢痕挛缩的效果。 方法 该研究为回顾性观察性研究。2016年1月—2023年1月, 广州和平骨科医院收治15例符合入选标准的手部掌侧瘢痕挛缩患者, 其中男12例、女3例, 年龄15~50岁。术前患手功能密歇根大学手概况问卷调查表(MHQ)得分为58~77分, 患手总主动活动度为190~220°。患手掌侧瘢痕切除后皮肤软组织缺损面积为5.2 cm×3.2 cm~7.2 cm×6.0 cm。根据创面位置和面积, 采用足底内侧动脉浅支穿支皮瓣或足底内侧动脉浅支皮穿支、足底内侧动脉深支内侧支联体皮瓣修复创面, 皮瓣切取面积为5.5 cm×3.5 cm~7.5 cm×6.8 cm。足部供区创面采用旋髂浅动脉穿支皮瓣修复。术后观察足底内侧动脉穿支皮瓣和旋髂浅动脉穿支皮瓣成活情况。皮瓣成活后指导患者行患手康复锻炼。术后定期门诊随访, 观察足底内侧动脉穿支皮瓣外形、色泽、质地及足部功能恢复情况。末次随访时, 测定足底内侧动脉穿支皮瓣两点辨别觉距离, 采用中华医学会手外科学会上肢部分功能评定试用标准及MHQ对患手功能进行评估。 结果 术后2例患者足底内侧动脉穿支皮瓣出现血管危象, 经急诊探查后皮瓣成活;其余患者足底内侧动脉穿支皮瓣和旋髂浅动脉穿支皮瓣均成活。术后随访6~18个月, 足底内侧动脉穿支皮瓣外观不臃肿, 色泽、质地与周围皮肤接近;足部跑、跳功能未受影响。末次随访时, 足底内侧动脉穿支皮瓣两点辨别觉距离为7~10 mm, 平均8 mm;患手功能评定为优者12例、良者3例;患手功能MHQ得分为81~95分, 患者对术后患手外观、疼痛情况、功能恢复情况均满意。 结论 应用足底内侧动脉穿支皮瓣整复手部掌侧瘢痕挛缩, 皮瓣切取简便、成活率高, 术后皮瓣感觉及患手功能恢复好, 足部供区损伤小, 值得临床推广。 Abstract:Objective To investigate the effects of medial plantar artery perforator flap in the reconstruction of palmar scar contracture. Methods This study was a retrospective observational study. From January 2016 to January 2023, 15 patients with palmar scar contracture who met the inclusion criteria were admitted to Guangzhou Peace Orthopedic Hospital, including 12 males and 3 females, aged 15 to 50 years. Before surgery, the Michigan Hand Outcomes Questionnaire (MHQ) scores for the affected hands ranged from 58 to 77, and the total active motion for the affected hands ranged from 190° to 220°. The skin and soft tissue defect area after scar excision on the palmar side of the affected hands was 5.2 cm×3.2 cm to 7.2 cm×6.0 cm. According to the location and area of the wounds, the defects were repaired using either medial plantar artery superficial perforator flaps or combined flaps of the cutaneous perforator of superficial branch of medial plantar artery and medial branch of medial plantar artery deep branch. The area of the harvested flaps was 5.5 cm×3.5 cm to 7.5 cm×6.8 cm. The donor site wounds on the feet were repaired using superficial circumflex iliac artery perforator flaps. Postoperatively, the survivals of the medial plantar artery perforator flaps and superficial circumflex iliac artery perforator flaps were observed. After survival of the flaps, patients were guided for rehabilitation exercises for the affected hands. Regular outpatient follow-up was conducted after surgery to observe the appearance, color, and texture of the medial plantar artery perforator flaps, and the recovery of foot function. At the final follow-up, the two-point discrimination distance of the medial plantar artery perforator flap was measured, the function of the affected hands was evaluated using the trial criteria for evaluation of partial function of upper extremity by the Hand Surgery Society of Chinese Medical Association and the MHQ. Results Postoperatively, two patients experienced vascular crisis of the medial plantar artery perforator flaps, while the flaps survived after emergency exploration; the medial plantar artery perforator flaps and superficial circumflex iliac artery perforator flaps survived in other patients. Follow-up for 6 to 18 months postoperatively showed that the medial plantar artery perforator flaps had no bulky appearance, similar color and texture to the surrounding skin, and the foot functions such as running and jumping were not affected. At the final follow-up, the two-point discrimination distance of the medial plantar artery perforator flap ranged from 7 to 10 mm, with an average of 8 mm; the affected hand function was rated as excellent in 12 cases and good in 3 cases; the MHQ scores of the affected hand function ranged from 81 to 95, and the patients were satisfied with the postoperative appearance, pain relief, and functional recovery of the affected hand. Conclusions The medial plantar artery perforator flap is used for the reconstruction of palmar scar contracture. The flap is easy to harvest, and has a high survival rate, resulting in good postoperative recovery of the flap sensation and function of the affected hand, and minimal donor site injury in the foot. It is therefore worthy of clinical promotion. -
Key words:
- Hand /
- Cicatrix /
- Perforator flap /
- Medial plantar artery /
- Hand surgery
本文亮点(1) 证实足底内侧动脉穿支血管走行恒定、位置表浅, 术中可根据创面需要灵活设计皮瓣, 皮瓣切取不损伤足底内侧动脉主干血管, 不影响足部血运;皮瓣供区隐蔽, 且位于足部非负重区, 皮瓣切取后不影响足部功能。(2) 证实足底内侧动脉穿支皮瓣与掌侧皮肤质地相近, 采用该皮瓣移植整复手部掌侧瘢痕挛缩, 术后患手外形、感觉、功能恢复良好, 患者满意度高。 -
参考文献
(41) [1] 朱婵, 何林, 张博文, 等. 儿童手烧伤后瘢痕挛缩家庭康复治疗模式的探索[J]. 中华烧伤与创面修复杂志, 2023, 39(1): 45-52. DOI: 10.3760/cma.j.cn501225-20220622-00253. [2] 叶门勒汉·巴合苏提汉, 王鑫, 艾合买提江·玉素甫. 游离股薄肌肌皮瓣修复上肢软组织缺损[J]. 组织工程与重建外科杂志, 2023, 19(2): 124-129. DOI: 10.3969/j.issn.1673-0364.2023.02.004. [3] 樊佳俊, 许佳, 李馨, 等. 3D打印手指静态进展性牵伸支具的设计及临床应用[J]. 组织工程与重建外科杂志, 2021, 17(4): 308-313. DOI: 10.3969/j.issn.1673-0364.2021.04.005. [4] Raposo-Amaral CE, Oliveira YM, Denadai R, et al. Apert hand reconstruction: do partial-thickness skin grafts result in flexion scar contracture?[J]. J Craniofac Surg, 2021, 32(1): 184-186. DOI: 10.1097/SCS.0000000000007064. [5] 宋春林, 罗成军, 朱雨. 四肢创伤性软组织缺损患者游离皮瓣移植失败的危险因素及预测模型构建[J]. 组织工程与重建外科杂志, 2024, 20(3): 305-311. DOI: 10.3969/j.issn.1673-0364.2024.03.005. [6] Cho H, Ono S, Chung KC. Management of scar contractures of the hand-our therapeutic strategy and challenges[J]. J Clin Med, 2024, 13(5): 1516. DOI: 10.3390/jcm13051516. [7] 王志刚, 裴蛟淼, 刘超华, 等. 预扩张肩胛皮瓣游离移植整复颈部瘢痕挛缩畸形的临床疗效[J]. 中华烧伤与创面修复杂志, 2023, 39(9): 813-819. DOI: 10.3760/cma.j.cn501225-20230225-00059. [8] 陈光, 芮永军, 宋骁军, 等. 五瓣术治疗指蹼蹼状挛缩伴手指掌侧挛缩[J]. 中华手外科杂志, 2017, 33(6): 404-405. DOI: 10.3760/cma.j.issn.1005-054X.2017.06.002. [9] 韩夫, 杨薛康, 何亭, 等. 足底内侧游离皮瓣整复手掌电烧伤创面及瘢痕挛缩的疗效[J]. 中华烧伤与创面修复杂志, 2023, 39(9): 820-825. DOI: 10.3760/cma.j.cn501225-20230601-00197. [10] Lu Y, Shen R, Zhou J, et al. Effect of transverse wrist crease perforator flap on repairing soft tissue defect of fingers and its influence on hand function[J]. Am J Transl Res, 2022, 14(10): 7156-7163. [11] Chung KC, Hamill JB, Walters MR, et al. The Michigan Hand Outcomes Questionnaire (MHQ): assessment of responsiveness to clinical change[J]. Ann Plast Surg, 1999, 42(6): 619-622. DOI: 10.1097/00000637-199906000-00006. [12] 潘生德, 顾玉东, 侍德. 中华医学会手外科学会上肢部分功能评定试用标准[J]. 中华手外科杂志, 2000, 16(3): 130. DOI: 10.3760/cma.j.issn.1005-054X.2000.03.003. [13] 杨鹏, 罗高兴. 具有分形亲水微通道的自泵油水凝胶促进烧伤创面愈合[J]. 中华烧伤与创面修复杂志, 2024, 40(1): 32. DOI: 10.3760/cma.j.issn.2097-1109.2024.01.101. [14] 刘彩霞, 陈文琦, 陈奕鹤, 等. 强脉冲光联合得宝松局部注射治疗瘢痕疙瘩的疗效观察[J]. 中国美容医学, 2025, 34(1): 117-120. [15] 林萱, 毛华荣, 庞凯. 环钻手术、药物注射联合PDL治疗瘢痕疙瘩疗效评价[J]. 中国麻风皮肤病杂志, 2025, 41(1): 33-36. DOI: 10.12144/zgmfskin202501033. [16] 吴杰, 吴烈霞. 预用局部浸润麻醉对瘢痕疙瘩内药物注射疼痛的影响[J]. 中国美容整形外科杂志, 2024, 35(3): 175-178. DOI: 10.3969/j.issn.1673-7040.2024.03.013. [17] 黄仲路, 胡鹏, 梁彦, 等. 增生性瘢痕注射治疗所用药物或生物相关制剂的研究[J]. 中国美容整形外科杂志, 2023, 34(11): 680-682, 后插4. DOI: 10.3969/j.issn.1673-7040.2023.11.010. [18] 姚敏, 张逸秋. 光生物调节在创伤修复和医学美容中的临床应用[J]. 中华烧伤与创面修复杂志, 2024, 40(4): 307-313. DOI: 10.3760/cma.j.cn501225-20240203-00048. [19] Wang Y, Sun Z, Cai L, et al. Comparative efficacy and safety of six photoelectric therapies for the atrophic acne scars: a network meta-analysis[J]. Indian J Dermatol Venereol Leprol, 2023, 89(3): 353-362. DOI: 10.25259/IJDVL_572_2021. [20] Zhang S, Zhao ZM, Xue HY, et al. Effects of photoelectric therapy on proliferation and apoptosis of scar cells by regulating the expression of microRNA-206 and its related mechanisms[J]. Int Wound J, 2020, 17(2): 317-325. DOI: 10.1111/iwj.13272. [21] Lin Y, Lin H, Zhu X, et al. Three-dimensional characterizations of two-photon excitation fluorescence images of elastic fibers affected by cutaneous scar duration[J]. Quant Imaging Med Surg, 2021, 11(8): 3584-3594. DOI: 10.21037/qims-20-1051. [22] 杨艳, 商颖, 吕强, 等. CO2点阵激光结合丝素蛋白载积雪草苷水凝胶治疗兔耳增生性瘢痕的实验研究[J]. 组织工程与重建外科杂志, 2022, 18(3): 227-232. DOI: 10.3969/j.issn.1673-0364.2022.03.005. [23] Lubczyńska A, Garncarczyk A, Wcisło-Dziadecka D. Effectiveness of various methods of manual scar therapy[J]. Skin Res Technol, 2023, 29(3): e13272. DOI: 10.1111/srt.13272. [24] Ogawa R, Dohi T, Tosa M, et al. The latest strategy for keloid and hypertrophic scar prevention and treatment: the Nippon Medical School (NMS) protocol[J]. J Nippon Med Sch, 2021, 88(1): 2-9. DOI: 10.1272/jnms.JNMS.2021_88-106. [25] Adams KL, Gallo V. The diversity and disparity of the glial scar[J]. Nat Neurosci, 2018, 21(1): 9-15. DOI: 10.1038/s41593-017-0033-9. [26] Amjadian S, Moradi S, Mohammadi P. The emerging therapeutic targets for scar management: genetic and epigenetic landscapes[J]. Skin Pharmacol Physiol, 2022, 35(5): 247-265. DOI: 10.1159/000524990. [27] Chen Z, Gao J, Li L. New challenges in scar therapy: the novel scar therapy strategies based on nanotechnology[J]. Nanomedicine (Lond), 2024, 19(28): 2413-2432. DOI: 10.1080/17435889.2024.2401768. [28] 沈余明, 马春旭, 覃凤均, 等. 腕部高压电烧伤创面修复与功能重建[J]. 中华烧伤杂志, 2017, 33(12): 738-743. DOI: 10.3760/cma.j.issn.1009-2587.2017.12.004. [29] 李海, 肖顺娥, 邓呈亮, 等. 不同类型游离穿支皮瓣组合在四肢复杂创面修复中的临床应用[J]. 中华烧伤与创面修复杂志, 2023, 39(8): 758-764. DOI: 10.3760/cma.j.cn501225-20220720-00300. [30] Opoku-Agyeman JL, Allen A, Humenansky K. The use of local medial plantar artery flap for heel reconstruction: a systematic review[J]. Cureus, 2020, 12(8): e9880. DOI: 10.7759/cureus.9880. [31] Xu X, Wang C, Chen Z, et al. Medial plantar artery perforator (MPAP) flap is an ideal option for reconstruction of complex soft tissue defect in the finger: clinical experience from 11 cases[J]. Front Surg, 2022, 9: 934173. DOI: 10.3389/fsurg.2022.934173. [32] Zhou JD, Zhang XF, Xu TL, et al. Super-thin anterolateral thigh flap for reconstruction of the medial plantar artery perforator flap donor site[J]. J Orthop Surg (Hong Kong), 2023, 31(2): 10225536231181706. DOI: 10.1177/10225536231181706. [33] Khan FH, Beg MSA, Obaid-Ur-Rahman. Medial plantar artery perforator flap: experience with soft-tissue coverage of heel[J]. Plast Reconstr Surg Glob Open, 2018, 6(12): e1991. DOI: 10.1097/GOX.0000000000001991. [34] Wu H, Sheng JG, Zhang CQ. Free medial plantar flap connection with a posterior tibial artery flap in reconstruction of fore-mid foot skin defect[J]. Plast Reconstr Surg Glob Open, 2016, 4(11): e1091. DOI: 10.1097/GOX.0000000000001091. [35] 刘辉, 邓呈亮, 陈健达, 等. 足底内侧动脉深支远端穿支皮瓣的血管解剖和临床应用研究[J]. 中华整形外科杂志, 2020, 36(9): 1005-1010. DOI: 10.3760/cma.j.cn114453-20200217-00051. [36] Li J, Luo X, Zou Y. Reconstruction of the palmar defect of the hand with a sensory medial plantar artery flap[J]. Front Surg, 2022, 9: 874629. DOI: 10.3389/fsurg.2022.874629. [37] Sundaramurthy N, Venkata Mahipathi SR, Durairaj AR, et al. "Like for like" reconstruction of heel pad with medial plantar artery flap-functional and aesthetic outcomes in a series of 19 cases[J]. Indian J Plast Surg, 2021, 54(3): 358-361. DOI: 10.1055/s-0041-1735424. [38] Scaglioni MF, Rittirsch D, Giovanoli P. Reconstruction of the heel, middle foot sole, and plantar forefoot with the medial plantar artery perforator flap: clinical experience with 28 cases[J]. Plast Reconstr Surg, 2018, 141(1): 200-208. DOI: 10.1097/PRS.0000000000003975. [39] Patel PK, Tewari S, Khunteta N. Medial plantar artery perforator flap for reconstruction of the soft tissue defect of heel melanoma[J]. Indian J Cancer, 2017, 54(4): 699-700. DOI: 10.4103/ijc.IJC_197_17. [40] 吴霄, 伍翰笙, 邓建林, 等. 足底内侧动脉穿支皮瓣移植修复手部掌侧瘢痕挛缩的早期康复[J]. 中华显微外科杂志, 2021, 44(2): 184-187. DOI: 10.3760/cma.j.cn441206-20200318-00155. [41] 石盛生, 费国芳. 桡动脉掌浅支腕横纹皮瓣游离移植修复手指软组织缺损[J]. 临床骨科杂志, 2019, 22(6): 701-704. DOI: 10.3969/j.issn.1008-0287.2019.06.022. -

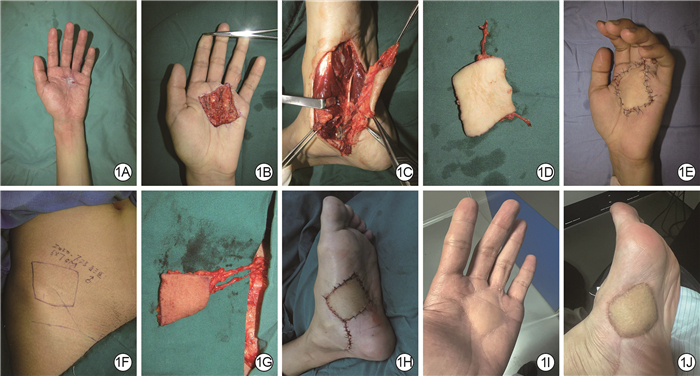
图 1 足底内侧动脉穿支皮瓣移植整复患者左手掌瘢痕挛缩的效果。1A.术前可见左手掌侧瘢痕挛缩, 左手中指、环指屈曲畸形;1B.术中切除左手掌侧瘢痕后;1C.术中切开足底内侧动脉穿支皮瓣, 显露足底内侧动脉浅支皮穿支、足底内侧动脉深支内侧支;1D.术中足底内侧动脉穿支皮瓣切取后;1E.术中将足底内侧动脉穿支皮瓣移植到左手掌后;1F、1G.分别为术中右侧旋髂浅动脉穿支皮瓣设计及切取后外观;1H.术中右侧旋髂浅动脉穿支皮瓣移植修复左足供区创面后;1I.术后1年随访时, 左手掌皮瓣外形不臃肿, 色泽接近正常手掌皮肤;1J.术后1年随访时, 左足供区移植的旋髂浅动脉穿支皮瓣外形美观
Figure 1. Effects of medial plantar artery perforator flap transplantation in the reconstruction of scar contracture on the left palm of a patient
-
 于玉芝 5月29日.mp4
于玉芝 5月29日.mp4

-

 下载:
下载:



图(1)
计量
- 文章访问数: 3514
- HTML全文浏览量: 541
- PDF下载量: 34
- 被引次数: 0
