




Clinical effects of various special forms of the descending branch of the lateral circumflex femoral artery perforator flaps in repairing high-voltage electrical burn wounds on the wrist
-
摘要:
目的 探讨多种特殊形式旋股外侧动脉降支(DLCFA)穿支皮瓣修复腕部高压电烧伤创面的临床效果。 方法 该研究为回顾性观察性研究。2014年9月—2024年6月,首都医科大学附属北京积水潭医院收治符合入选标准的腕部高压电烧伤男性患者79例,其年龄为20~62岁,腕部高压电烧伤创面(下称腕部创面)分型为Ⅱ型或Ⅲ型。伤后早期,对患者腕部行清创术,根据创面情况及皮瓣适应证,单独采用血流桥接、分叶、嵌合、血流桥接-分叶、分叶-嵌合、血流桥接-嵌合、血流桥接-分叶-嵌合DLCFA穿支皮瓣或者联合采用血流桥接-嵌合DLCFA穿支皮瓣与阔筋膜张肌肌皮瓣修复创面。采用直接拉拢缝合或皮片移植方式修复供瓣区创面。记录术中切取各类DLCFA穿支皮瓣数及其修复的各型腕部创面数、供瓣区创面封闭情况,统计术后皮瓣成活情况、是否发生血管危象、创面或者缝合口愈合情况、血流桥接皮瓣重建动脉通畅情况。随访时,观察皮瓣外形、瘢痕形成情况,以及大腿肌疝发生情况。 结果 术中,切取11个血流桥接DLCFA穿支皮瓣修复11个Ⅱ型腕部创面,切取13个分叶DLCFA穿支皮瓣修复9个Ⅱ型和4个Ⅲ型腕部创面,切取16个嵌合DLCFA穿支皮瓣修复16个Ⅱ型腕部创面,切取11个血流桥接-分叶DLCFA穿支皮瓣修复5个Ⅱ型和6个Ⅲ型腕部创面,切取10个分叶-嵌合DLCFA穿支皮瓣修复5个Ⅱ型和5个Ⅲ型腕部创面,切取6个血流桥接-嵌合DLCFA穿支皮瓣修复6个Ⅱ型腕部创面,切取7个血流桥接-分叶-嵌合DLCFA穿支皮瓣修复7个Ⅲ型腕部创面,另切取5个血流桥接-嵌合DLCFA穿支皮瓣联合阔筋膜张肌肌皮瓣修复5个Ⅲ型腕部创面。74例患者供瓣区创面经直接缝合封闭,5例患者供瓣区创面经皮片移植封闭。术后,3例患者皮瓣发生血管危象,其中动脉危象1例、静脉危象2例,经急诊血管探查等处理后皮瓣成活;其余皮瓣完全成活。术后,3例患者皮瓣下方有渗出,经换药治疗后封闭;其余患者创面或缝合口均愈合。动脉造影显示,35例行血流桥接皮瓣移植患者术后重建动脉全部通畅。随访3个月~1年期间,20例患者皮瓣臃肿,其余患者皮瓣外形良好;行创面直接缝合的供瓣区遗留线性瘢痕,供瓣区创面植皮区片状瘢痕增生不明显;未出现大腿肌疝。 结论 充分利用穿支皮瓣优势,采用多种特殊形式DLCFA穿支皮瓣修复腕部高压电烧伤立体性损伤创面,既使供区损伤最小化,又使受区得到良好修复,近期随访外观较佳。 Abstract:Objective To explore the clinical effects of various special forms of the descending branch of the lateral circumflex femoral artery (DLCFA) perforator flaps in repairing high-voltage electrical burn wounds on the wrist. Methods This study was a retrospective observational study. From September 2014 to June 2024, 79 male patients with high-voltage electrical burns on the wrist, aged 20 to 62 years and met the inclusion criteria, were admitted to Beijing Jishuitan Hospital Affiliated to Capital Medical University, with wrist high-voltage electrical burn wound (hereinafter referred to as wrist wound) types being classified as type Ⅱ or type Ⅲ. In the early stage after injury, debridement was performed on the patients' wrists. Based on the wound condition and flap indications, the flow-through, lobed, chimeric, flow-through-lobed, lobed-chimeric, flow-through-chimeric, or flow-through-lobed-chimeric DLCFA perforator flap was employed individually, and the flow-through-chimeric DLCFA perforator flap and tensor fascia lata myocutaneous flap were employed in combination to repair the wounds. The donor site wounds were repaired using direct sutures or skin grafting. The number of various DLCFA perforator flaps resected during surgery and the number of various types of wrist wounds repaired were recorded, as well as the closure status of the donor site wound. The postoperative flap survival, occurrence of vascular crisis, wound or suture site healing, and patency of the reconstructed artery in flow-through flaps were recorded. During follow-up, the appearance of the flap, scar formation, and the presence of thigh muscle herniation were observed. Results Intraoperatively, 11 flow-through DLCFA perforator flaps were resected to repair 11 type Ⅱ wrist wounds, 13 lobed DLCFA perforator flaps were resected to repair 9 type Ⅱ and 4 type Ⅲ wrist wounds, 16 chimeric DLCFA perforator flaps were resected to repair 16 type Ⅱ wrist wounds, 11 flow-through-lobed DLCFA perforator flaps were resected to repair 5 type Ⅱ and 6 type Ⅲ wrist wounds, 10 lobed-chimeric DLCFA perforator flaps were resected to repair 5 type Ⅱ and 5 type Ⅲ wrist wounds, 6 flow-through-chimeric DLCFA perforator flaps were resected to repair 6 type Ⅱ wrist wounds, 7 flow-through-lobed-chimeric DLCFA perforator flaps were resected to repair 7 type Ⅲ wrist wounds, and 5 flow-through-chimeric DLCFA perforator flaps combined with tensor fascia lata myocutaneous flaps were resected to repair 5 type Ⅲ wrist wounds. Seventy-four patients had their donor site wounds closed by direct suturing, while 5 patients had their donor site wounds closed by skin grafting. Postoperatively, the flaps in 3 patients developed vascular crisis, including 1 case of arterial crisis and 2 cases of venous crises but survived after emergency vascular exploration and other treatments; the remaining flaps survived completely. Postoperatively, 3 patients had seepage beneath their flaps, which were closed after dressing changes; the remaining patients' wounds or suture sites all healed. Anteriography showed that all reconstructed arteries in 35 patients who underwent flow-through flap transplantation were patent postoperatively. During the follow-up period of 3 months to 1 year, 20 patients had bloated flap, while the rest had good flap appearance; linear scars were left in the donor sites that underwent direct wound closure, and the skin-grafted areas of the donor site wounds showed no significant patchy hypertrophic scarring; no thigh muscle herniation occurred. Conclusions Taking the full advantage of perforator flaps, various special forms of the DLCFA perforator flaps are used to repair the three-dimensionally injury wounds caused by high-voltage electrical burns on the wrist, which not only minimizes the damage to the donor site but also allow the recipient site to be well repaired, showing good appearance in the recent follow-up. -
参考文献
(40) [1] 沈余明.高压电烧伤创面修复与功能重建[J].中华烧伤杂志,2018,34(5):257-262.DOI: 10.3760/cma.j.issn.1009-2587.2018.05.001. [2] 张丕红,黄晓元,黄跃生.深度电烧伤创面早期修复专家共识(2020版)[J].中华创伤杂志,2020,36(10):865-871.DOI: 10.3760/cma.j.cn501098-20200706-00488. [3] 沈余明,马春旭,覃凤均,等.腕部高压电烧伤创面修复与功能重建[J].中华烧伤杂志,2017,33(12):738-743.DOI: 10.3760/cma.j.issn.1009-2587.2017.12.004. [4] 沈余明,代强.毁损性电烧伤患者的功能重建与康复策略探讨[J].中华烧伤与创面修复杂志,2023,39(8):713-717.DOI: 10.3760/cma.j.cn501225-20230506-00158. [5] 朱海锋,杨晓东,王海涛,等.结合内增压技术的股前外侧跨区皮瓣修复肢体较大创面临床研究[J].浙江大学学报(医学版),2024,53(4):401-410.DOI: 10.3724/zdxbyxb-2023-0613. [6] 仓飞成,周树萍,幸超峰,等.股前外侧嵌合穿支分叶肌皮瓣修复肢体腔隙性创面[J].实用手外科杂志,2023,37(1):44-46.DOI: 10.3969/j.issn.1671-2722.2023.01.013. [7] 唐举玉,吴攀峰,俞芳,等.特殊类型穿支皮瓣在创伤骨科的临床应用[J].中华创伤杂志,2014,30(11):1085-1088.DOI: 10.3760/cma.j.issn.1001-8050.2014.11.006. [8] 邢培朋,郭海娜,狄海萍,等.游离股前外侧皮瓣联合动脉血管重建修复腕部高压电烧伤创面的临床效果[J].中华烧伤杂志,2020,36(6):419-425.DOI: 10.3760/cma.j.cn501120-20200219-00067. [9] 杜伟力,臧子睿,沈余明,等.含肌瓣的股前外侧嵌合穿支皮瓣修复腕部高压电烧伤创面的效果观察[J].中国医刊,2024,59(5):513-516.DOI: 10.3969/j.issn.1008-1070.2024.05.012. [10] 沈祖尧,王乃佐,马春旭,等.应用带蒂与游离皮瓣修复腕部电烧伤创面的比较[J].中华整形烧伤外科杂志,1996,12(3):238-239.DOI: 10.3760/j.issn:1009-4598.1996.03.036. [11] CastroJC,ColtroPS,MillanLS,et al.Early application of microsurgical flaps in the electric burns of extremities: a two institutional case series[J].J Burn Care Res,2018,39(6):1037-1042.DOI: 10.1093/jbcr/irx010. [12] 杜伟力,沈余明,陈忠,等.多部位电烧伤毁损性创面修复方法的探讨[J/CD].中华损伤与修复杂志(电子版),2024,19(2):99-105.DOI: 10.3877/cma.j.issn.1673-9450.2024.02.002. [13] 沈余明,覃凤均,杜伟力,等.濒临截肢四肢高压电烧伤患者的保肢策略[J].中华烧伤杂志,2019,35(11):776-783.DOI: 10.3760/cma.j.issn.1009-2587.2019.11.003. [14] 杜伟力,沈余明,胡骁骅,等.巨大腹壁下动脉脐旁穿支皮瓣修复腕部环状高压电烧伤创面的临床效果[J].中华烧伤与创面修复杂志,2023,39(6):527-533.DOI: 10.3760/cma.j.cn501225-20220719-00296. [15] 覃凤均,王成,张颖,等.游离皮瓣联合血管重建在上肢毁损性创面合并血管损伤修复中的应用[J].中国普通外科杂志,2023,32(6):840-849.DOI: 10.7659/j.issn.1005-6947.2023.06.005. [16] 唐举玉,贺继强,吴攀峰,等.股前外侧分叶-嵌合穿支皮瓣在四肢复杂创伤修复中的应用[J].中华显微外科杂志,2020,43(4):326-330.DOI: 10.3760/cma.j.cn441206-20190309-00089. [17] 唐举玉,徐达传,徐永清,等.特殊形式穿支皮瓣及其衍生术式命名专家共识[J].中华显微外科杂志,2022,45(1):5-13.DOI: 10.3760/cma.j.cn441206-20220114-00010. [18] 唐举玉.特殊形式穿支皮瓣及其衍生术式的分型与命名[J].中华显微外科杂志,2021,44(3):245-254.DOI: 10.3760/cma.j.cn441206-20210530-00193. [19] 唐举玉,孙念哲,吴攀峰,等.股前外侧穿支皮瓣的个性化精准设计:十年1079例临床疗效分析[J].中国临床解剖学杂志,2024,42(5):510-516.DOI: 10.13418/j.issn.1001-165x.2024.5.04. [20] QingL,WuP,YuF,et al.Sequential chimeric deep circumflex iliac artery perforator flap and flow-through anterolateral thigh perforator flap for one-stage reconstruction of complex tissue defects[J].J Plast Reconstr Aesthet Surg,2019,72(7):1091-1099.DOI: 10.1016/j.bjps.2019.02.029. [21] QingL,WuP,YuF,et al.Use of a sequential chimeric perforator flap for one-stage reconstruction of complex soft tissue defects of the extremities[J].Microsurgery,2020,40(2):167-174.DOI: 10.1002/micr.30450. [22] AzouzSM,CastelNA,VijayasekaranA,et al.Lower-limb reconstruction with chimeric flaps: the quad flap[J].Microsurgery,2019,39(2):182-187.DOI: 10.1002/micr.30335. [23] BritoÍM,VazM,BrandãoC,et al.Bilateral lower limb salvage after fourth-degree burns: subscapular axis free and chimeric flaps effectiveness in complex reconstruction[J].Plast Reconstr Surg Glob Open,2020,8(6):e2911.DOI: 10.1097/GOX.0000000000002911. [24] 唐林 特殊形式穿支皮瓣修复四肢复杂创面的临床研究 泸州 西南医科大学 2023 唐林.特殊形式穿支皮瓣修复四肢复杂创面的临床研究[D].泸州:西南医科大学,2023.
[25] ZhangY,PanX,YangH,et al.Computed tomography angiography for the chimeric anterolateral thigh flap in the reconstruction of the upper extremity[J].J Reconstr Microsurg,2017,33(3):211-217.DOI: 10.1055/s-0036-1597587. [26] WangC,ShenYM,QinFJ,et al.Free flow-through anterolateral thigh flaps for wrist high-tension electrical burns: a retrospective case series[J].Biomed Environ Sci,2020,33(7):510-517.DOI: 10.3967/bes2020.064. [27] ChenX,ZhangC,ChengL,et al.Survival and versatility of the flow-through lateral-thigh free flap in severe electrical injuries to the wrist[J].Ann Plast Surg,2020,85(6):612-617.DOI: 10.1097/SAP.0000000000002355. [28] LeeDH,DesaiMJ,GaugerEM.Electrical injuries of the hand and upper extremity[J].J Am Acad Orthop Surg,2019,27(1):e1-e8.DOI: 10.5435/JAAOS-D-17-00833. [29] KoshimaI,FukudaH,YamamotoH,et al.Free anterolateral thigh flaps for reconstruction of head and neck defects[J].Plast Reconstr Surg,1993,92(3):421-428; discussion 429-430. [30] 陈黎明,刘毅,张诚,等.带肌瓣的嵌合穿支皮瓣修复合并深部死腔的难愈性创面[J].中华整形外科杂志,2020,36(3):279-283.DOI: 10.3760/cma.j.cn114453-20190605-00176. [31] 李伟,刘建惠,陈亚伟,等.旋股外侧动脉降支嵌合穿支皮瓣修复足部软组织缺损合并深部无效腔创面[J].中华显微外科杂志,2023,46(2):215-219.DOI: 10.3760/cma.j.cn441206-20220621-00126. [32] SongB,ChenJ,HanY,et al.The use of fabricated chimeric flap for reconstruction of extensive foot defects[J].Microsurgery,2016,36(4):303-309.DOI: 10.1002/micr.22399. [33] 计鹏,曹涛,张智,等.股前外侧嵌合穿支皮瓣修复足踝部复杂创面的效果[J].中华烧伤与创面修复杂志,2023,39(10):926-932.DOI: 10.3760/cma.j.cn501225-20230627-00232. [34] 周望高,张振伟,余少校,等.带肌瓣的旋股外侧动脉降支穿支皮瓣修复合并死腔的小腿软组织缺损[J].中国美容整形外科杂志,2021,32(7):411-414.DOI: 10.3969/j.issn.1673-7040.2021.07.009. [35] PerraultD,RochlinD,PhamC,et al.Timing of flap surgery in acute burn patients does not affect complications[J].J Burn Care Res,2020,41(5):967-970.DOI: 10.1093/jbcr/iraa096. [36] 张颖,沈余明.腕部高压电烧伤诊治的研究进展[J].中华创伤杂志,2021,37(5):467-472.DOI: 10.3760/cma.j.cn501098-20210105-00010. [37] 狄海萍,李永林,邢培朋,等.皮瓣修复腕部高压电烧伤创面的手术时机选择[J].中华显微外科杂志,2019,42(2):166-169.DOI: 10.3760/cma.j.issn.1001-2036.2019.02.016. [38] ZhaoJC,ShiK,HongL,et al.Retrospective review of free anterolateral thigh flaps for limb salvage in severely injured high-voltage electrical burn patients[J].Ann Plast Surg,2018,80(3):232-237.DOI: 10.1097/SAP.0000000000001283. [39] RadulovicN,MasonSA,RehouS,et al.Acute and long-term clinical, neuropsychological and return-to-work sequelae following electrical injury: a retrospective cohort study[J].BMJ Open,2019,9(5):e025990.DOI: 10.1136/bmjopen-2018-025990. [40] LiH,TanJ,ZhouJ,et al.Wound management and outcome of 595 electrical burns in a major burn center[J].J Surg Res,2017,214:182-189.DOI: 10.1016/j.jss.2017.02.032. -

图 1 采用右下肢嵌合旋股外侧动脉降支(DLCFA)穿支皮瓣修复例1患者Ⅱ型左腕部高压电烧伤创面的效果。1A、1B.分别为术前左腕部创面腕屈侧、腕背侧观;1C.左腕部切开减张术后即刻;1D.术前上肢动脉造影显示尺动脉栓塞,桡动脉通畅;1E.彻底清创,去除坏死屈指肌肉,保留屈指肌腱和正中神经,左腕部形成死腔;1F.设计大小为24 cm×11 cm的右下肢DLCFA穿支皮瓣;1G.切取嵌合股外侧肌肌瓣的DLCFA穿支皮瓣;1H.皮瓣转移至左腕部,肌瓣填塞腕部死腔;1I.术后2周,皮瓣存活良好,创面愈合;1J.术后2周,右大腿供瓣区愈合

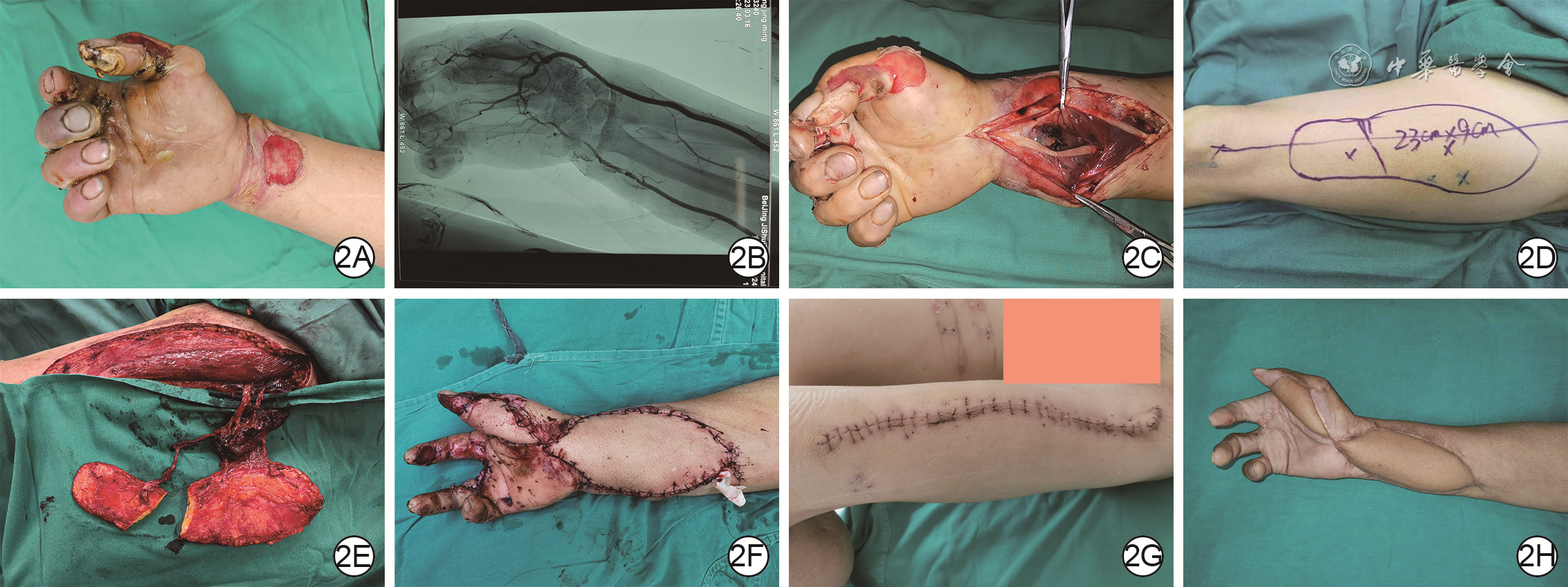
图 2 采用左下肢分叶-嵌合旋股外侧动脉降支(DLCFA)穿支皮瓣修复例2患者Ⅱ型右腕部高压电烧伤创面及右拇指Ⅲ度高压电烧伤创面的效果。2A.术前右腕部及右拇指创面;2B.术前右上肢动脉造影显示尺动脉栓塞,桡动脉通畅;2C.急诊行腕部切开减张后即刻;2D.设计总大小为23 cm×9 cm的左下肢分叶DLCFA穿支皮瓣;2E.切取皮瓣并分为2叶,在近端2条穿支附近携带部分股外侧肌,形成分叶-嵌合皮瓣;2F.皮瓣转移至右腕及右手,近端分叶嵌合皮瓣覆盖腕部死腔及创面,远端分叶皮瓣覆盖拇指创面;2G.术后2周,供瓣区缝合口愈合良好;2H.术后6个月,皮瓣存活良好,稍臃肿

图 3 采用右下肢血流桥接-分叶旋股外侧动脉降支(DLCFA)穿支皮瓣修复例3患者Ⅱ型右腕部高压电烧伤创面及右手Ⅲ度高压电烧伤创面的效果。3A.右腕部及右手创面;3B.右上肢动脉造影显示尺、桡动脉全部栓塞,骨间血管通畅;3C.设计总大小为30 cm×11 cm的右下肢分叶DLCFA穿支皮瓣;3D.腕部及手部创面彻底清创,血流桥接-分叶DLCFA穿支皮瓣切取完成后即刻;3E.转移皮瓣,近端分叶皮瓣覆盖腕部,远端分叶皮瓣覆盖手部,降支主干远端与手部尺动脉端端吻合;3F.术后右上肢动脉造影显示,重建尺动脉通畅;3G.术后6个月,皮瓣存活良好,手部皮瓣臃肿;3H.术后6个月,供瓣区遗留线性瘢痕

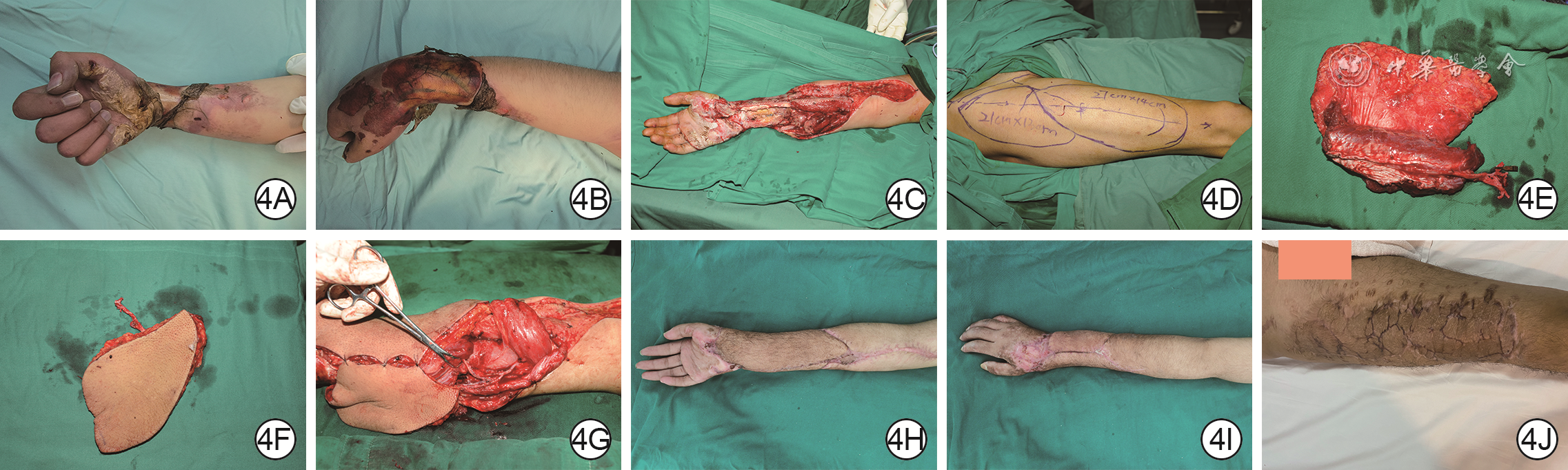
图 4 采用右下肢血流桥接-嵌合旋股外侧动脉降支(DLCFA)穿支皮瓣联合阔筋膜张肌肌皮瓣修复例4患者Ⅲ型右腕部高压电烧伤创面的效果。4A、4B.分别为术前右腕部创面腕屈侧、腕背侧观;4C.右腕部彻底清创去除所有坏死组织后即刻;4D.设计大小分别为21 cm×13 cm和27 cm×14 cm的右下肢DLCFA穿支皮瓣与阔筋膜张肌肌皮瓣;4E.切取的血流桥接-嵌合股外侧肌肌瓣的DLCFA穿支皮瓣;4F.切取的阔筋膜张肌肌皮瓣;4G.皮瓣转移至右腕部创面,DLCFA穿支皮瓣覆盖腕掌部创面,阔筋膜张肌肌皮瓣覆盖腕背侧创面,DLCFA主干近端与尺动脉端端吻合,阔筋膜张肌肌皮瓣血管与DLCFA主干串联吻合;4H、4I.分别为术后12个月受区腕屈侧、腕背侧观,皮瓣存活良好且不臃肿;4J.术后12个月,供瓣区创面植皮区片状瘢痕增生不明显
皮瓣类型 皮瓣数 修复的腕部高压电烧伤创面分型 Ⅱ型 Ⅲ型 血流桥接DLCFA穿支皮瓣 11 11 0 分叶DLCFA穿支皮瓣 13 9 4 嵌合DLCFA穿支皮瓣 16 16 0 血流桥接-分叶DLCFA穿支皮瓣 11 5 6 分叶-嵌合DLCFA穿支皮瓣 10 5 5 血流桥接-嵌合DLCFA穿支皮瓣 6 6 0 血流桥接-分叶-嵌合DLCFA穿支皮瓣 7 0 7 血流桥接-嵌合DLCFA穿支皮瓣联合阔筋膜张肌肌皮瓣 5 0 5 注:DLCFA为旋股外侧动脉降支  下载: 导出CSV
下载: 导出CSV
-
 杜伟力.mp4
杜伟力.mp4

-

 下载:
下载:






计量
- 文章访问数: 2361
- HTML全文浏览量: 973
- PDF下载量: 39
- 被引次数: 0
