




Clinical effect of indocyanine green angiography-assisted design and harvest of expanded flaps for scar reconstruction
-
摘要:
目的 探讨在吲哚菁绿血管造影(ICGA)辅助下设计、切取扩张皮瓣整复瘢痕的临床效果。 方法 该研究为回顾性观察性研究。2019年4月—2023年8月,中国医学科学院北京协和医学院整形外科医院收治19例符合入选标准的瘢痕患者,其中男8例、女11例,年龄3~38岁,瘢痕分布于头面部、躯干及四肢。Ⅰ期手术:于瘢痕周围选择合适区域埋置皮肤软组织扩张器行皮肤软组织扩张术。Ⅱ期手术:切除瘢痕组织(形成创面面积100~210 cm²)并设计扩张皮瓣,行ICGA确定扩张皮瓣的目标穿支及其伴行静脉,调整皮瓣设计确保包含完整动静脉轴,使用单侧回切法切取面积为120~240 cm²扩张皮瓣并转移至受区。直接缝合供区创面。记录扩张皮瓣设计过程中ICGA的动脉期和静脉期持续时间。统计不同部位回切皮瓣的长宽比。Ⅱ期术后,观察皮瓣的血流灌注及成活情况、供区创面愈合情况及并发症发生情况。随访时,观察患者皮瓣外观、色泽和质地。 结果 ICGA的动脉期持续时间为10~27(18±5)s,静脉期持续时间为78~116(100±10)s。头面部、躯干和四肢的回切皮瓣长宽比分别为1.22±0.32、1.63±0.12和1.15±0.21。Ⅱ期术后,1例患者皮瓣存在大面积血流灌注不足,通过比较转移皮瓣前后的ICGA图像,行松开口角处的缝线处理,皮瓣血运得以恢复;其余患者皮瓣血流灌注良好。皮瓣均完全成活;供区创面愈合良好,无并发症发生。随访0.5~14.0个月显示,所有患者皮瓣外观良好,色泽和质地与周围皮肤相近。 结论 ICGA作为浅表血流可视化手段,不仅可以清晰呈现术前扩张皮瓣的微血管分布,辅助优化皮瓣设计,还能够评估术后皮瓣的血流灌注情况,减少并发症的发生,为扩张皮瓣的切取提供全程导航,提高该皮瓣转移整复瘢痕手术的安全性。 Abstract:Objective To investigate the clinical effect of indocyanine green angiography (ICGA)-assisted design and harvest of expanded flaps for scar reconstruction. Methods This study was a retrospective observational study. From April 2019 to August 2023, 19 patients with scars (8 males, 11 females; aged 3-38 years) treated at the Plastic Surgery Hospital of Peking Union Medical College and Chinese Academy of Medical Sciences met the inclusion criteria. The scars were distributed on the head, face, trunk, and extremities. In stage Ⅰ surgery, skin soft tissue expanders were implanted in suitable areas around the scars for skin soft tissue expansion. In stage Ⅱ surgery, the scar tissue was excised, resulting in wound areas ranging from 100 to 210 cm2, and expanded flaps were designed. ICGA was used to identify target perforators and their accompanying veins, and the flap design was adjusted to ensure the inclusion of complete arterial and venous axes. The expanded flap with an area of 120 to 240 cm² was harvested using unilateral back-cut technique and transferred to the recipient site, and the donor site wound was sutured directly. The durations of the arterial and venous phases of ICGA during flap design were recorded. The length-to-width ratios of the back-cut flaps were calculated for different regions. After stage Ⅱ surgery, the blood perfusion and survival of the flap, the wound healing at the donor site, and the occurrence of complications were observed. During follow-up, the appearance, color, and texture of the patient's flap were observed. Results The arterial phase of ICGA lasted 10-27 (18±5) s, and the venous phase lasted 78-116 (100±10) s. The length-to-width ratios of the back-cut flaps were 1.22±0.32, 1.63±0.12, and 1.15±0.21 for the head and neck, trunk, and limb regions, respectively. After stage Ⅱ surgery, one patient had a large area of insufficient blood perfusion in the flap. By comparing ICGA images before and after flap transfer, the sutures at the oral commissure were loosened, the blood flow of the flap was restored. The blood perfusion of the flaps in other patients was good. All flaps survived completely, with well-healed donor site wounds and no complications. During 0.5-14.0 months of follow-up, all flaps of patients demonstrated excellent appearance, with color and texture matching the surrounding skin. Conclusions As a means of superficial blood flow visualization, ICGA can not only clearly show the microvascular distribution of the expanded flap before operation, assist in optimizing the design of the flap, but also evaluate the blood perfusion of the flap after operation, reduce the occurrence of complications, and provide a full-process navigation for the harvesting of expanded flaps, thereby improving the safety of flap transfer for scar reconstruction. -
Key words:
- Cicatrix /
- Angiography /
- Perforator flap /
- Indocyanine green angiography /
- Skin and soft tissue expansion /
- Flap design /
- Wound repair
-
参考文献
(35) [1] GuoY, SongY, XiongS, et al. Mechanical stretch induced skin regeneration: molecular and cellular mechanism in skin soft tissue expansion[J]. Int J Mol Sci, 2022,23(17): 9622. DOI: 10.3390/ijms23179622. [2] RadwanAM, ZideMF. Tissue expansion in the head and neck[J]. Atlas Oral Maxillofac Surg Clin North Am, 2019,27(2):167-173. DOI: 10.1016/j.cxom.2019.05.010. [3] TongX, LuJ, ZhangW, et al. Efficacy and safety of external tissue expansion technique in the treatment of soft tissue defects: a systematic review and meta-analysis of outcomes and complication rates[J/OL]. Burns Trauma, 2022,10:tkac045[2025-01-08]. https://pubmed.ncbi.nlm.nih.gov/36518877/. DOI: 10.1093/burnst/tkac045. [4] 张伟, 张卫东, 陈斓, 等. 扩张皮瓣整复大面积烧伤后面颈部瘢痕挛缩畸形的临床效果[J]. 中华烧伤与创面修复杂志, 2023, 39(9):826-834. DOI: 10.3760/cma.j.cn501225-20230706-00248. [5] ZideBM, KarpNS. Maximizing gain from rectangular tissue expanders[J]. Plast Reconstr Surg, 1992,90(3):500-504; discussion 505-506. [6] CherryGW, AustadE, PasykK, et al. Increased survival and vascularity of random-pattern skin flaps elevated in controlled, expanded skin[J]. Plast Reconstr Surg, 1983,72(5):680-687. DOI: 10.1097/00006534-198311000-00018. [7] ZhuH, XieY, XieF, et al. Prevention of necrosis of adjacent expanded flaps by surgical delay[J]. Ann Plast Surg, 2014,73(5):525-530. DOI: 10.1097/SAP.0b013e31827fafce. [8] XieT, LiuY, ZhuS, et al. Finding perforator "freeway" for design optimization of expanded flaps by indocyanine green angiography[J]. Plast Reconstr Surg, 2025,155(2):414e-418e. DOI: 10.1097/PRS.0000000000011545. [9] TaylorGI, ChubbDP, AshtonMW. True and 'choke' anastomoses between perforator angiosomes: part Ⅰ. Anatomical location[J]. Plast Reconstr Surg, 2013,132(6):1447-1456. DOI: 10.1097/PRS.0b013e3182a80638. [10] OgawaR, OkiK, HyakusokuH. Skin perforator freeways and pathways: understanding the role of true and choke anastomoses between perforator angiosomes and their impact on skin flap planning and outcomes[J]. Plast Reconstr Surg, 2014,133(5):719e-720e. DOI: 10.1097/PRS.0000000000000139. [11] AltafFM. The anatomical basis of the medial sural artery perforator flaps[J]. West Indian Med J, 2011,60(6):622-627. [12] GurtnerGC, JonesGE, NeliganPC, et al. Intraoperative laser angiography using the SPY system: review of the literature and recommendations for use[J]. Ann Surg Innov Res, 2013,7(1):1. DOI: 10.1186/1750-1164-7-1. [13] NarushimaM, YamasobaT, IidaT, et al. Pure skin perforator flaps: the anatomical vascularity of the superthin flap[J]. Plast Reconstr Surg, 2018,142(3):351e-360e. DOI: 10.1097/PRS.0000000000004698. [14] Saint-CyrM, WongC, SchaverienM, et al. The perforasome theory: vascular anatomy and clinical implications[J]. Plast Reconstr Surg, 2009,124(5):1529-1544. DOI: 10.1097/PRS.0b013e3181b98a6c. [15] HyakusokuH, GaoJH, PenningtonDG, et al. The microvascular augmented subdermal vascular network (ma-SVN) flap: its variations and recent development in using intercostal perforators[J]. Br J Plast Surg, 2002,55(5):402-411. DOI: 10.1054/bjps.2002.3865. [16] LiuY, ZangM, ZhuS, et al. Pre-expanded paraumbilical perforator flap[J]. Clin Plast Surg, 2017,44(1):99-108. DOI: 10.1016/j.cps.2016.08.003. [17] OnodaS, AzumiS, HasegawaK, et al. Preoperative identification of perforator vessels by combining MDCT, doppler flowmetry, and ICG fluorescent angiography[J]. Microsurgery, 2013,33(4):265-269. DOI: 10.1002/micr.22079. [18] Vander KolkCA, McCannJJ, KnightKR, et al. Some further characteristics of expanded tissue[J]. Clin Plast Surg, 1987,14(3):447-453. [19] ChanP, ColonAF, CluneJ, et al. External tissue expansion in complex extremity reconstruction[J]. J Hand Surg Am, 2021,46(12):1094-1103. DOI: 10.1016/j.jhsa.2021.07.039. [20] ErogluS, BuyukdoganH, DuranA. Direct-to-implant retropectoral dual plane approach with autologous inferior-based dermal flap: does SPY-elite laser angiographic system reduce complication rates?[J]. Aesthetic Plast Surg, 2024,48(21):4414-4420. DOI: 10.1007/s00266-024-04075-1. [21] TaghizadehF, TroobSH, WaxMK. The role of fluorescent angiography in free flap reconstruction of the head and neck[J]. Laryngoscope, 2023,133(6):1388-1393. DOI: 10.1002/lary.30450. [22] GoncalvesLN, van den HovenP, van SchaikJ, et al. Perfusion parameters in near-infrared fluorescence imaging with indocyanine green: a systematic review of the literature[J]. Life (Basel), 2021,11(5):433. DOI: 10.3390/life11050433. [23] YangCE, ChungSW, LeeDW, et al. Evaluation of the relationship between flap tension and tissue perfusion in implant-based breast reconstruction using laser-assisted indocyanine green angiography[J]. Ann Surg Oncol, 2018,25(8):2235-2240. DOI: 10.1245/s10434-018-6527-1. [24] 王石, 董帅, 曹阳, 等. 高选择性动脉吲哚菁绿造影在游离股前外侧皮瓣设计中的应用[J]. 中华烧伤与创面修复杂志, 2024, 40(10): 948-954. DOI: 10.3760/cma.j.cn501225-20240513-00174. [25] WangC, ZhangJ, HyakusokuH, et al. An overview of pre-expanded perforator flaps: part 2, clinical applications[J]. Clin Plast Surg, 2017,44(1):13-20. DOI: 10.1016/j.cps.2016.09.007. [26] TanO, AtikB, BekereciogluM. Supercharged reverse-flow sural flap: a new modification increasing the reliability of the flap[J]. Microsurgery, 2005,25(1):36-43. DOI: 10.1002/micr.20072. [27] KimuraN, SaitohM, OkamuraT, et al. Concept and anatomical basis of microdissected tailoring method for free flap transfer[J]. Plast Reconstr Surg, 2009,123(1):152-162. DOI: 10.1097/PRS.0b013e3181934756. [28] DriessenC, ArnardottirTH, LorenzoAR, et al. How should indocyanine green dye angiography be assessed to best predict mastectomy skin flap necrosis? A systematic review[J]. J Plast Reconstr Aesthet Surg, 2020,73(6):1031-1042. DOI: 10.1016/j.bjps.2020.02.025. [29] BigcasJM, DeBiaseCA, HoT. Indocyanine green angiography as the principal design and perfusion assessment tool for the supraclavicular artery island flap in head and neck reconstruction[J]. Cureus, 2022,14(9):e29007. DOI: 10.7759/cureus.29007. [30] GelişkenF. Indocyanine green angiography[J]. Turk J Ophthalmol, 2024,54(1):38-45. DOI: 10.4274/tjo.galenos.2023.89735. [31] PanettellaT, MeroniM, ScaglioniMF. How to increase the success rate in microsurgical free and pedicled flap reconstructions with intraoperative multistep ICG imaging: a case series with 400 consecutive cases[J]. J Plast Reconstr Aesthet Surg, 2024,97:147-155. DOI: 10.1016/j.bjps.2024.07.047. [32] WangM, ZangM, ZhuS, et al. Utility of indocyanine green angiography for preventing pre-expanded extended lower trapezius myocutaneous flap necrosis: how to make the correct decision for hypoperfused areas[J]. J Reconstr Microsurg, 2023,39(5):383-391. DOI: 10.1055/a-1939-5606. [33] MattisonGL, LewisPG, GuptaSC, et al. SPY imaging use in postmastectomy breast reconstruction patients: preventative or overly conservative?[J]. Plast Reconstr Surg, 2016,138(1):15e-21e. DOI: 10.1097/PRS.0000000000002266. [34] LiuEH, ZhuSL, HuJ, et al. Intraoperative SPY reduces post-mastectomy skin flap complications: a systematic review and meta-analysis[J]. Plast Reconstr Surg Glob Open, 2019,7(4):e2060. DOI: 10.1097/GOX.0000000000002060. [35] ZhangY, XiaoW, NgS, et al. Infrared thermography-guided designing and harvesting of pre-expanded pedicled flap for head and neck reconstruction[J]. J Plast Reconstr Aesthet Surg, 2021,74(9):2068-2075. DOI: 10.1016/j.bjps.2020.12.102. -

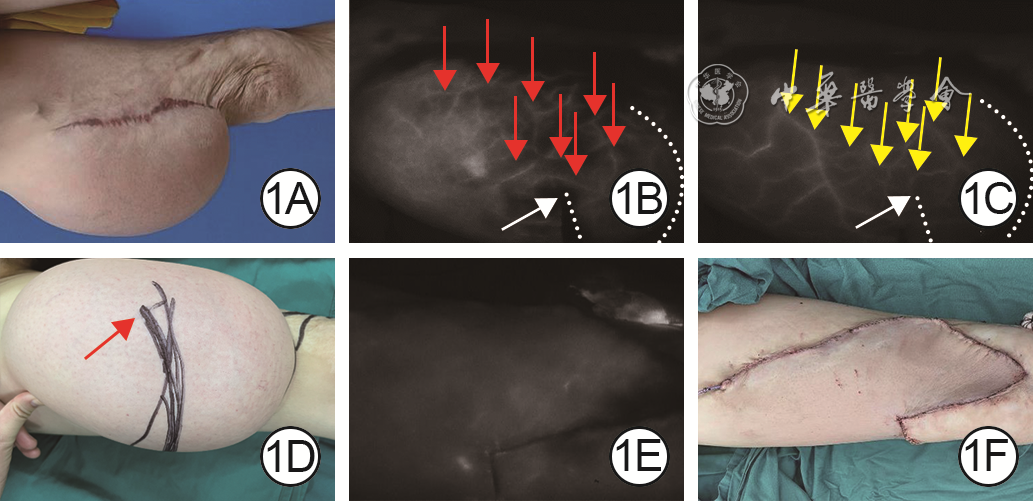
图 1 吲哚菁绿血管造影(ICGA)辅助下设计切取扩张皮瓣修复例1患者右腿瘢痕切除后形成的创面的效果。1A.Ⅱ期术前,瘢痕及扩张皮瓣情况;1B.Ⅱ期术前,扩张皮瓣的ICGA动脉期显像,其中红色箭头指示动脉穿支,白色虚线为回切设计线,白色箭头指示回切终点;1C.Ⅱ期术前,扩张皮瓣的ICGA静脉期显像,黄色箭头指示浅表静脉,白色虚线和白色箭头指示内容同图1B;1D.Ⅱ期术前皮瓣设计,红色箭头指示回切终点;1E.转移皮瓣后再次行ICGA检查,血流灌注情况良好;1F.皮瓣转移术后即刻

图 2 吲哚菁绿血管造影(ICGA)辅助下设计切取扩张皮瓣修复例2患者面部瘢痕切除后形成的创面的效果。2A.Ⅱ期术前,瘢痕情况及扩张皮瓣设计;2B.Ⅱ期术前,扩张皮瓣的ICGA动脉期显像,红色箭头指示穿支及其分支;2C.Ⅱ期术前,扩张皮瓣的ICGA静脉期显像,黄色箭头指示图2B中穿支及其分支的伴行浅表静脉;2D.Ⅱ期术中,首次ICGA检查显示回切皮瓣血流灌注可;2E.皮瓣与创面切口完全缝合后,第2次ICGA检查显示皮瓣血流灌注情况,白色虚线圈内区域(患者下唇部)存在动脉血流灌注不足;2F.松开口角处缝线后,第3次ICGA检查显示白色虚线圈内下唇区域血流灌注改善;2G.术后12.0个月随访,皮瓣外观良好,色泽和质地与周围皮肤相近
-
 胡雅楠 4月7日.mp4
胡雅楠 4月7日.mp4

-

 下载:
下载:





图(3)
计量
- 文章访问数: 2129
- HTML全文浏览量: 358
- PDF下载量: 42
- 被引次数: 0
