




The LENS four-element diagnostic method and WDSR scoring and grading system applicable to the discipline of wound repair
-
摘要: 随着人口老龄化进程加剧,各类老年急慢性创面已成为全球公共健康的重要负担,创面修复学科的成立和发展具有迫切的时代需求。目前创面类疾病的诊断具有描述性和异质性特点,客观上限制了学术交流和学科发展。该文提出普遍适用于局灶性创面的LENS四要素诊断法,包括部位(location)、病因(etiology)、性质(nature)和严重程度(severity)4个要素,期望能够全面、准确地反映创面情况,为创面治疗、疾病分级、预后评价等提供宝贵信息。该文还提出WDSR计分分级系统,选择创面宽度(width)、深度(depth)、窦腔(sinus)及复发情况(recurrence)共4项指标进行计分,并按照总分进行分级(Ⅰ~Ⅳ级),可对创面局部的严重程度进行量化评估。倡议有条件的创面修复科试点应用LENS四要素诊断法和WDSR计分分级系统,以促进创面修复学科的规范化发展。Abstract: With the aging of population intensifying, various acute and chronic wounds in the elderly have become an important burden on global public health. The establishment and development of the wound repair discipline have become an urgent need of the times. Currently, the diagnosis of wound diseases is descriptive and heterogeneous, which objectively limits academic exchanges and the development of the discipline. This article proposed the LENS four-element diagnostic method that is universally applicable to focal wounds, including location, etiology, nature, and severity. It is expected to comprehensively and accurately reflect the condition of the wounds and provide valuable information for wound treatment, disease grading, and prognosis evaluation. This article proposed the WDSR scoring and grading system, which selects four indicators for scoring, including wound width, depth, sinus, and recurrence. The system grades the wounds according to the total score (grades Ⅰ-Ⅳ), which can quantitatively assess the severity of the local wounds. It is advocated that the wound repair departments with conditions pilot the LENS four-element diagnostic method and the WDSR scoring and grading system to promote the standardized development of the wound repair discipline.
-
Key words:
- Ulcer /
- Diagnosis /
- Focal wounds /
- Chronic wounds /
- Refractory wounds /
- Wound grading
-
参考文献
(38) [1] SenCK.Human wound and its burden: updated 2020 compendium of estimates[J].Adv Wound Care (New Rochelle),2021,10(5):281-292.DOI: 10.1089/wound.2021.0026. [2] 国家卫生健康委员会办公厅 国家卫生健康委办公厅关于加强体表慢性难愈合创面(溃疡)诊疗管理工作的通知 2019-12-02 2025-08-09 http://www.nhc.gov.cn/yzygj/s7659/201912/602716f0471944b8b63b0adabe4546df.shtml 国家卫生健康委员会办公厅. 国家卫生健康委办公厅关于加强体表慢性难愈合创面(溃疡)诊疗管理工作的通知 [EB/OL].(2019-12-02) [2025-08-09]. http://www.nhc.gov.cn/yzygj/s7659/201912/602716f0471944b8b63b0adabe4546df.shtml.
[3] 付小兵.建设规范化和标准化创面修复科在中国的实践[J].中华创伤杂志,2020,36(1):3-5.DOI: 10.3760/cma.j.issn.1001-8050.2020.01.002. [4] BowersS,FrancoE.Chronic wounds: evaluation and management[J].Am Fam Physician,2020,101(3):159-166. [5] SilvaJLG, Oliveira KumakuraARS, ZanchettaFC, et al. Clinical simulation for teaching of wound evaluation and treatment[J]. Clin Simul Nurs, 2020, 38:5-13.DOI: 10.1016/j.ecns.2019.09.003. [6] MortonLM,PhillipsTJ.Wound healing and treating wounds: differential diagnosis and evaluation of chronic wounds[J].J Am Acad Dermatol,2016,74(4):589-605; quiz 605-606.DOI: 10.1016/j.jaad.2015.08.068. [7] HøylandSA,HolteKA,IslamK,et al.A cross-sector systematic review and synthesis of knowledge on telemedicine interventions in chronic wound management-implications from a system perspective[J].Int Wound J,2023,20(5):1712-1724.DOI: 10.1111/iwj.13986. [8] DissemondJ,BültemannA,GerberV,et al.The term mixed leg ulcer should no longer be used today[J].Dermatologie (Heidelb),2023,74(7):555-559.DOI: 10.1007/s00105-023-05129-2. [9] RayalaBZ.Skin ulcers: prevention and diagnosis of pressure, venous leg, and arterial ulcers[J].FP Essent,2020,499:11-18. [10] KimuraS,TsujiT.Mechanical and immunological regulation in wound healing and skin reconstruction[J].Int J Mol Sci,2021,22(11):5474.DOI: 10.3390/ijms22115474. [11] PutriIL,AdzalikaLB,PramanasariR,et al.Negative pressure wound therapy versus conventional wound care in cancer surgical wounds: a meta-analysis of observational studies and randomised controlled trials[J].Int Wound J,2022,19(6):1578-1593.DOI: 10.1111/iwj.13756. [12] 姚泽欣,付小兵,程飚. 慢性创面愈合新理念:姑息性创面治疗的研究进展[J]. 中华烧伤杂志,2020,36(8):754-757. DOI: 10.3760/cma.j.cn501120-20190929-00388. [13] TangX,ShiW,QianY,et al.Effect of suture closure and staple closure on postoperative wound complications in patients undergoing knee replacement surgery: a meta-analysis[J].Int Wound J,2024,21(1):e14372.DOI: 10.1111/iwj.14372. [14] MendemS, FarazMAA, RaoKL. A case report on necrotizing fasciitis in a hemiplegic patient following an intra-muscular injection[J]. Int J Community Med Public Health, 2020,7(9):3689. DOI: 10.18203/2394-6040.ijcmph20203945. [15] AllawF,WehbeS,KanjSS.Necrotizing fasciitis: an update on epidemiology, diagnostic methods, and treatment[J].Curr Opin Infect Dis,2024,37(2):105-111.DOI: 10.1097/QCO.0000000000000988. [16] 曾帅丹,杨磊.各种组学分析在体表慢性难愈合创面中的研究进展[J].中华烧伤与创面修复杂志,2023,39(1):75-80.DOI: 10.3760/cma.j.cn501225-20220216-00030. [17] 中华医学会内分泌学分会,中国内分泌代谢病专科联盟.糖尿病足溃疡创面治疗专家共识(2024)[J].中华内分泌代谢杂志,2024,40(7):565-569.DOI: 10.3760/cma.j.cn311282-20240625-00281. [18] SyautaD, Mulawardi, Prihantono, et al. Risk factors affecting the degree of diabetic foot ulcers according to Wagner classification in diabetic foot patients[J]. Medicina Clínica Práctica, 2021, 4Suppl 1: 100231. DOI: 10.1016/j.mcpsp.2021.100231. [19] Vera-CruzPN,PalmesPP,TonoganL,et al.Comparison of WIFi, University of Texas and Wagner classification systems as major amputation predictors for admitted diabetic foot patients: a prospective cohort study[J].Malays Orthop J,2020,14(3):114-123.DOI: 10.5704/MOJ.2011.018. [20] SantemaTB,LenselinkEA,BalmR,et al.Comparing the Meggitt-Wagner and the University of Texas wound classification systems for diabetic foot ulcers: inter-observer analyses[J].Int Wound J,2016,13(6):1137-1141.DOI: 10.1111/iwj.12429. [21] JalilianM,Ahmadi SarbarzehP,OubariS.Factors related to severity of diabetic foot ulcer: a systematic review[J].Diabetes Metab Syndr Obes,2020,13:1835-1842.DOI: 10.2147/DMSO.S256243. [22] BrocklehurstJD.The validity and reliability of the SINBAD classification system for diabetic foot ulcers[J].Adv Skin Wound Care,2023,36(11):1-5.DOI: 10.1097/ASW.0000000000000050. [23] JesusFRM, IbrahimA, Rodriguez-RamirezN, et al. The Latin American Saint Elian Wound Score System (SEWSS) for the triage of the diabetic foot attack[J]. Cir Cir, 2021, 89(5): 679-685. DOI: 10.24875/CIRU.20000283. [24] GandhiC, KadamP, KamepalliV, et al. PEDIS grading and its role in diabetic foot ulcer management[J]. Int Surg J, 2019, 6(7): 2548-2552. DOI: 10.18203/2349-2902.isj20192990. [25] BeckertS,WitteM,WickeC,et al.A new wound-based severity score for diabetic foot ulcers: a prospective analysis of 1,000 patients[J].Diabetes Care,2006,29(5):988-992.DOI: 10.2337/diacare.295988. [26] HalászBG,AlvesPJP,O'ConnorT,et al.EPUAP pressure ulcer curriculum[J].J Wound Care,2023,32(9):598-606.DOI: 10.12968/jowc.2023.32.9.598. [27] National pressure ulcer advisory panel. NPUAP pressure ulcer stages/categories[J]. Ostomy Wound Manage, 2007:53. [28] LurieF,PassmanM,MeisnerM,et al.The 2020 update of the CEAP classification system and reporting standards[J].J Vasc Surg Venous Lymphat Disord,2020,8(3):342-352.DOI: 10.1016/j.jvsv.2019.12.075. [29] PassmanMA,McLaffertyRB,LentzMF,et al.Validation of Venous Clinical Severity Score (VCSS) with other venous severity assessment tools from the American Venous Forum, National Venous Screening Program[J].J Vasc Surg,2011,54(6Suppl):2S-9S.DOI: 10.1016/j.jvs.2011.05.117. [30] 中国老年医学学会烧创伤分会,中华医学会组织修复与再生分会,中国康复医学会再生医学与康复专业委员会,等.放射性皮肤损伤的诊断和治疗专家共识(2024版)[J].中华烧伤与创面修复杂志,2024,40(8):701-712.DOI: 10.3760/cma.j.cn501225-20240126-00033. [31] Becerro-RecioD,SerratJ,López-GarcíaM,et al.Study of the cross-talk between Fasciola hepatica juveniles and the intestinal epithelial cells of the host by transcriptomics in an in vitro model[J].Vet Parasitol,2023,320:109981.DOI: 10.1016/j.vetpar.2023.109981. [32] SimpsonKJ,SelforsLM,BuiJ,et al.Identification of genes that regulate epithelial cell migration using an siRNA screening approach[J].Nat Cell Biol,2008,10(9):1027-1038.DOI: 10.1038/ncb1762. [33] 蔡程浩,韩春茂,王新刚.创面外部微环境因素对创面愈合影响的研究进展[J].中华烧伤与创面修复杂志,2024,40(5):489-494.DOI: 10.3760/cma.j.cn501225-20230827-00067. [34] AlsabekMB,Abdul AzizAR.Diabetic foot ulcer, the effect of resource-poor environments on healing time and direct cost: a cohort study during Syrian crisis[J].Int Wound J,2022,19(3):531-537.DOI: 10.1111/iwj.13651. [35] GuptaS,AndersenC,BlackJ,et al.Management of chronic wounds: diagnosis, preparation, treatment, and follow-up[J].Wounds,2017,29(9):S19-S36. [36] 马先,唐佳俊,吴敏洁,等.内镜技术治疗慢性窦道(腔)创面诊疗规范(试行版)[J].中华烧伤杂志,2019,35(12):833-838.DOI: 10.3760/cma.j.issn.1009-2587.2019.12.001. [37] 赵陈雨瑶,张玉珅,杨占杰,等.肠瘘继发坏死性筋膜炎病例的临床资料分析及死亡危险因素筛查[J].中华烧伤与创面修复杂志,2024,40(2):141-150.DOI: 10.3760/cma.j.cn501225-20230923-00088. [38] KanadashviliO,BelykhE,SoborovM,et al.Necrotic fasciitis as a complication of acute destructive appendicitis[J].Georgian Med News,2021(311):21-27. -

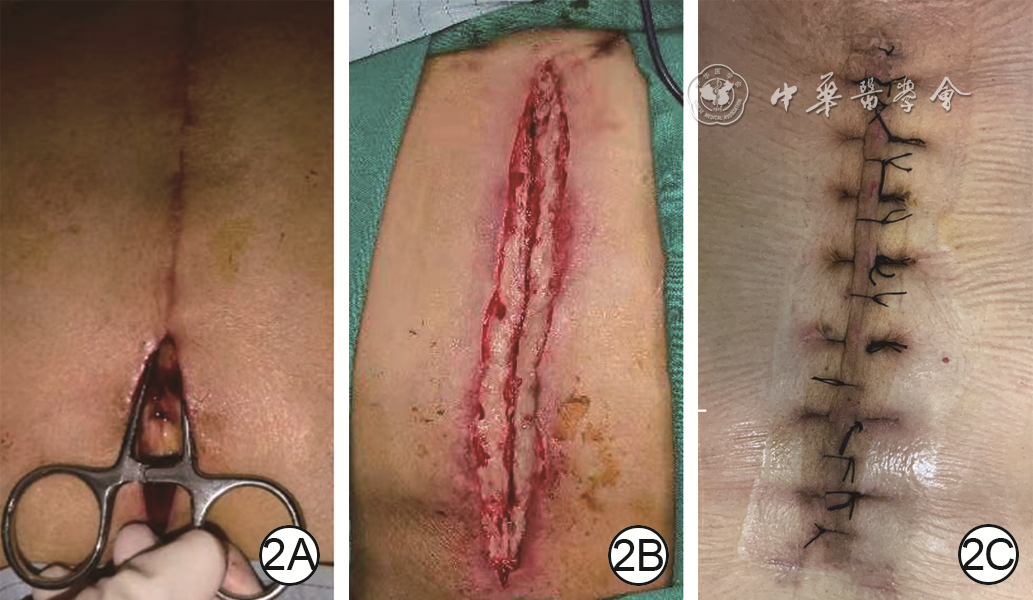
图 2 胸部正中切口不愈创面的诊断(感染性,W1D2S2R0,5分Ⅱ级)。2A.入院时,切口下段裂开并探及切口下腔隙;2B.清创术中,可见脂肪层组织感染坏死,无深部组织外露;2C.出院时,切口愈合良好

图 3 左坐骨结节压力性损伤的诊断(失神经性,W1D2S3R1,7分Ⅲ级)和右坐骨结节压力性损伤的诊断(失神经性,W2D2S3R1,8分Ⅲ级)。3A.入院时左侧创面内可见坏死组织和腔隙;3B.入院时右侧创面内可见坏死组织和腔隙;3C.术中清创后,可见深部坐骨结节骨膜部分坏死;3D.左侧复合皮瓣转移术后即刻,可见皮瓣血运良好;3E.右侧复合皮瓣转移术后即刻,可见皮瓣血运良好;3F.出院时,可见双侧创面愈合

图 4 左糖尿病足溃疡的诊断(感染性,W2D3S2R1,8分Ⅲ级)。4A.入院时足内侧创面,见皮肤全层缺损,肌肉组织部分坏死;4B.入院时第2足趾区创面,见第2跖骨外露;4C.足内侧创面清创手术后,见大范围窦腔;4D.第2足趾区创面清创手术后,见第2跖骨部分被咬除;4E.出院时,左足内侧创面愈合;4F.出院时,第2足趾区创面愈合
Table 1. 适用于多类型局灶性创面的WDSR计分系统
评分(分) 宽度 深度 窦腔 复发情况 0 无皮损 无皮损 无窦腔 首发且病程≤3个月 1 0~3 cm 创面基底为皮肤层(表皮层或真皮层) 整个窦腔结构在深筋膜以浅 复发或病程>3个月 2 >3 cm且≤10 cm 创面基底为软组织层(脂肪层或肌肉层) 窦腔结构涉及深筋膜以深 — 3 >10 cm 创面基底可见肌腱、骨膜等深部组织 有瘘管连通关节腔、胸腔、腹腔、肠道等自然腔隙 — 注:WDSR指宽度、深度、窦腔、复发情况;宽度指创面愈合过程中上皮组织需要迁移的最远距离(cm);深度指在体外直视下活性基底组织的层次;窦腔指创面基底存在的直视不可见,但探查可及的脓肿、窦道、腔隙和瘘管等所有窦腔类结构;复发情况指创面病程和是否出现复发;应将部位、病因和性质均相同的多个创面视为一个大创面进行计分,否则应分别计分;“—”表示无此项  下载: 导出CSV
下载: 导出CSV
Table 2. 适用于多类型局灶性创面的WDSR分级系统和治疗建议
分级 WDSR总分(分) 治疗建议 Ⅰ级 1~3 保守治疗促进愈合 Ⅱ级 4~6 简单手术封闭创面 Ⅲ级 7或8 复杂手术修复创面 Ⅳ级 9或10 联合治疗控制创面 注:WDSR指宽度、深度、窦腔、复发情况
下载: 导出CSV
-

 下载:
下载:




计量
- 文章访问数: 1135
- HTML全文浏览量: 510
- PDF下载量: 37
- 被引次数: 0
