




Construction of a topographic map assessment system for hand burn wounds and scars based on the Delphi method
-
摘要:
目的 构建一套适用于手部烧伤创面与瘢痕的地形图评估系统。 方法 该研究采用文献分析和调查研究相结合的方法,以手部功能解剖和美学为基础,以手部烧伤创面、瘢痕、畸形与活动度评估为中心,初步形成手部烧伤创面与瘢痕地形图评估系统。采取现场汇报的方式进行预函询,根据专家意见修订后于2024年12月—2025年3月,运用德尔菲法对符合入选标准的16名来自广州市、深圳市的烧伤与康复相关领域专家开展了1轮正式函询,其中男6人、女10人,年龄(43±9)岁,工作年限9~39年,副高级及以上职称者7人。统计正式函询问卷有效回收比例、所有条目的专家权威系数均值,所有三级条目的重要性专家评分的均值、变异系数均值、满分率均值以及肯德尔和谐系数、变异系数。根据正式函询结果最终确定手部烧伤创面与瘢痕地形图评估系统的条目。 结果 正式函询问卷有效回收比例为16/16,所有条目的专家权威系数均值为0.84。所有三级条目的重要性专家评分的均值为4.76,变异系数均值为0.10,满分率均值为80.32%。所有三级条目重要性专家评分的肯德尔和谐系数为0.18,结果有统计学意义(χ2=15.83,P<0.05);所有三级条目重要性专家评分的变异系数均<0.25。正式函询后无删除或增添条目,最后形成手部烧伤创面与瘢痕地形图评估系统。该评估系统由手部烧伤创面与瘢痕地形图结合创面、瘢痕、畸形与活动度评估表构成,包含6个一级条目、16个二级条目、44个三级条目。 结论 构建了一套涵盖面广、可用性强的手部烧伤创面与瘢痕地形图评估系统,可精准评估手部烧伤后的创面、瘢痕、畸形和活动度。 Abstract:Objective To construct a topographic map assessment system for hand burn wounds and scars. Methods A combination of literature analysis and survey research was adopted in this study. Based on the functional anatomy and aesthetics of hands, and focusing on the assessment of the wounds, scars, deformities, and range of motion after hand burns, a topographic map assessment system for hand burn wounds and scars was preliminarily developed. A pre-consultation was conducted in the form of on-site presentations. After revision based on expert opinions, the Delphi method was used to conduct a round of formal consultation from December 2024 to March 2025 with 16 experts from Guangzhou and Shenzhen in burns, rehabilitation, and relevant fields who met the selection criteria. Among the consultation experts, 6 were male and 10 were female, aged (43±9) years, with working experience ranging from 9 to 39 years, and 7 experts held the title of associate senior or higher. The effective recovery ratio of the formal consultation questionnaires and the mean expert authority coefficient of all items were calculated. The mean value, the mean coefficient of variation, and the mean full-score rate, as well as the Kendall's coefficient of concordance and the coefficient of variation of the expert importance score of all the third-level items were calculated. Based on the formal consultation results, the items for the topographic map assessment system for hand burn wounds and scars were ultimately determined. Results The effective recovery ratio of the formal consultation questionnaires was 16/16, and the mean expert authority coefficient of all items was 0.84. For the expert importance scores of all the third-level items, the mean value was 4.76, the mean coefficient of variation was 0.10, and the mean full-score rate was 80.32%. For all the third-level items, the Kendall's coefficient of concordance of expert importance scores was 0.18, with statistically significance (χ2=15.83, P<0.05), and the coefficient of variation of expert importance scores was <0.25. After the formal consultation, no items were deleted or added, and finally a topographic map assessment system for hand burn wounds and scars was formed. The evaluation system consists of a combination of hand burn wounds and scars topographic map and an evaluation table for wounds, scars, deformities, and range of motion, including 6 first-level items, 16 second-level items, and 44 third-level items. Conclusions A comprehensive and highly usable topographic map assessment system for hand burn wounds and scars was constructed, which enables precise assessment of the wounds, scars, deformities, and range of motion after hand burns. -
Key words:
- Hand /
- Burns /
- Cicatrix /
- Delphi technique /
- Wounds /
- Assessment system
-
参考文献
(41) [1] Mata-RibeiroL,VieiraL,VilelaM.Epidemiology and outcome assessment of hand burns: a 3-year retrospective analysis in a burn unit[J].Ann Burns Fire Disasters,2022,35(1):18-25. [2] WangKA,SunY,WuGS,et al.Epidemiology and outcome analysis of hand burns: a 5-year retrospective review of 378 cases in a burn center in Eastern China[J].Burns,2015,41(7):1550-1555.DOI: 10.1016/j.burns.2015.04.004. [3] ZikajG,BelbaG,XhepaG.Epidemiology of hand burn in Albania 2011-2016[J].Open Access Maced J Med Sci,2018,6(5):931-933.DOI: 10.3889/oamjms.2018.202. [4] MurtaughB,WarthmanR,BoulterT.Rehabilitation management of the burned hand[J].Phys Med Rehabil Clin N Am,2023,34(4):767-782.DOI: 10.1016/j.pmr.2023.05.001. [5] JohnsonSP,ChungKC.Outcomes assessment after hand burns[J].Hand Clin,2017,33(2):389-397.DOI: 10.1016/j.hcl.2016.12.011. [6] EdwardsJ,MasonS.Hand burn management: minimising pain and trauma at dressing change[J].Br J Nurs,2013,22(20):S46, S48-50.DOI: 10.12968/bjon.2013.22.Sup20.S46. [7] 卞瑞豪,黄诗欣,朱家源,等. 基于德尔菲法构建烧伤患者面颈部创面与瘢痕地形图评估系统[J]. 中华烧伤与创面修复杂志,2023,39(12):1115-1121. DOI: 10.3760/cma.j.cn501225-20230905-00075. [8] DalkeyN, HelmerO. An experimental application of the Delphi method to the use of experts[J]. Manage Sci, 1963,9(3):458-467. [9] von der GrachtHA. Consensus measurement in Delphi studies: review and implications for future quality assurance[J]. Technol Forecast Soc Change, 2012,79(8):1525-1536. DOI: 10.1016/j.techfore.2012.04.013. [10] DiamondIR,GrantRC,FeldmanBM,et al.Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies[J].J Clin Epidemiol,2014,67(4):401-409.DOI: 10.1016/j.jclinepi.2013.12.002. [11] NasaP,JainR,JunejaD.Delphi methodology in healthcare research: how to decide its appropriateness[J].World J Methodol,2021,11(4):116-129.DOI: 10.5662/wjm.v11.i4.116. [12] NiederbergerM,KöberichS,members of the DeWiss Network.Coming to consensus: the Delphi technique[J].Eur J Cardiovasc Nurs,2021,20(7):692-695.DOI: 10.1093/eurjcn/zvab059. [13] JaamM,AwaisuA,El-AwaisiA,et al.Use of the Delphi technique in pharmacy practice research[J].Res Social Adm Pharm,2022,18(1):2237-2248.DOI: 10.1016/j.sapharm.2021.06.028. [14] NiederbergerM,SprangerJ.Delphi technique in health sciences: a map[J].Front Public Health,2020,8:457.DOI: 10.3389/fpubh.2020.00457. [15] ZarnowitzV, LambrosLA. Consensus and uncertainty in economic prediction[J]. J Polit Econ, 1987,95(3):591-621. [16] LinstoneHA, TuroffM. The delphi method[M]. Massachusetts: Addison-Wesley, 1975. [17] HassonF,KeeneyS,McKennaH.Research guidelines for the Delphi survey technique[J].J Adv Nurs,2000,32(4):1008-1015. [18] 陆树良.把握创面修复的规律和特征促进创面愈合[J].中华烧伤杂志,2021,37(5):401-403.DOI: 10.3760/cma.j.cn501120-20210322-00100. [19] BaronJM,GlatzM,ProkschE.Optimal support of wound healing: new insights[J].Dermatology,2020,236(6):593-600.DOI: 10.1159/000505291. [20] 沈余明.复杂性创面的修复与功能重建[J/CD].中华损伤与修复杂志(电子版),2015,10(1):9-12.DOI: 10.3877/cma.j.issn.1673-9450.2015.01.004. [21] 黄书润,刘江涛,张勇,等.手部烧创伤后复杂创面的修复[J].中华烧伤杂志,2019,35(5):362-366.DOI: 10.3760/cma.j.issn.1009-2587.2019.05.007. [22] KumarS,KhanFAA,AliH,et al.Surgical management of post burn hand deformities[J].Pak J Med Sci,2020,36(6):1387-1391.DOI: 10.12669/pjms.36.6.2206. [23] KowalskeK.Outcome assessment after hand burns[J].Hand Clin,2009,25(4):557-561.DOI: 10.1016/j.hcl.2009.06.003. [24] KnightA,WasiakJ,SalwayJ,et al.Factors predicting health status and recovery of hand function after hand burns in the second year after hospital discharge[J].Burns,2017,43(1):100-106.DOI: 10.1016/j.burns.2016.07.025. [25] AntonopulosD, DanikasD, DotsikasR, et al. The treatment of early and late hand contractures following burn injury (1978–1991)[J].Ann MBC, 1992,30:100-101. [26] SchneiderJC,HolavanahalliR,HelmP,et al.Contractures in burn injury part II: investigating joints of the hand[J].J Burn Care Res,2008,29(4):606-613.DOI: 10.1097/BCR.0b013e31817db8e1. [27] KantS,van den KerckhoveE,CollaC,et al.Duration of scar maturation: retrospective analyses of 361 hypertrophic scars over 5 years[J].Adv Skin Wound Care,2019,32(1):26-34.DOI: 10.1097/01.ASW.0000547415.38888.c4. [28] 刘毅.瘢痕非手术治疗中几个值得关注的问题[J].中华烧伤杂志,2021,37(12):1194-1198.DOI: 10.3760/cma.j.cn501120-20210705-00235. [29] 中国整形美容协会瘢痕医学分会.瘢痕早期治疗全国专家共识(2020版)[J].中华烧伤杂志,2021,37(2):113-125.DOI: 10.3760/cma.j.cn501120-20200609-00300. [30] BacheSE,Fitzgerald O'ConnorE,TheodorakopoulouE,et al.The hand burn severity (HABS) score: a simple tool for stratifying severity of hand burns[J].Burns,2017,43(1):93-99.DOI: 10.1016/j.burns.2016.07.011. [31] 张娟,蔡娟,李海芬,等.手部烧伤严重程度评估工具的汉化及初步临床应用研究[J].中华急危重症护理杂志,2023,4(5):399-404.DOI: 10.3761/j.issn.2096-7446.2023.05.003. [32] 皋文君,袁长蓉.患者自我报告结局测量信息系统在国外的应用进展[J].中华护理杂志,2018,53(11):1401-1405.DOI: 10.3761/j.issn.0254-1769.2018.11.026. [33] ZiolkowskiNI,PusicAL,FishJS,et al.Psychometric findings for the SCAR-Q patient-reported outcome measure based on 731 children and adults with surgical, traumatic, and burn scars from four countries[J].Plast Reconstr Surg,2020,146(3):331e-338e.DOI: 10.1097/PRS.0000000000007078. [34] 邹颖,张慧琳,陈偶英,等.国内患者报告结局研究热点可视化分析[J].护士进修杂志,2024,39(5):552-557.DOI: 10.16821/j.cnki.hsjx.2024.05.020. [35] BroderickJE,MayM,SchwartzJE,et al.Patient reported outcomes can improve performance status assessment: a pilot study[J].J Patient Rep Outcomes,2019,3(1):41.DOI: 10.1186/s41687-019-0136-z. [36] BacheSE,Fitzgerald O'ConnorE,DrakePJH,et al.Development and validation of the Burnt Hand Outcome Tool (BHOT): a patient-led questionnaire for adults with hand burns[J].Burns,2018,44(8):2087-2098.DOI: 10.1016/j.burns.2018.07.014. [37] 张娟,柴雪珺,关立锋,等. 手部烧伤结局评估工具的汉化和跨文化调试及信效度检验[J]. 中华烧伤杂志,2021,37(10):978-986. DOI: 10.3760/cma.j.cn501120-20210201-00042. [38] Mc KittrickA,GustafssonL,MarshallK.A systematic review to investigate outcome tools currently in use for those with hand burns, and mapping psychometric properties of outcome measures[J].Burns,2021,47(2):295-314.DOI: 10.1016/j.burns.2020.07.009. [39] MathersJ,MoiemenN,BamfordA,et al.Ensuring that the outcome domains proposed for use in burns research are relevant to adult burn patients: a systematic review of qualitative research evidence[J/OL].Burns Trauma,2020,8:tkaa030[2025-08-30].https://pubmed.ncbi.nlm.nih.gov/33163540/.DOI: 10.1093/burnst/tkaa030. [40] FinlayV,BurrowsS,BurmazM,et al.Increased burn healing time is associated with higher Vancouver Scar Scale score[J].Scars Burn Heal,2017,3:2059513117696324.DOI: 10.1177/2059513117696324. [41] 郑民华,马君俊,戴可帆,等.智慧医学时代微创外科的进展与展望[J].中华消化外科杂志,2024,23(4):543-547.DOI: 10.3760/cma.j.cn115610-20240318-00162. -

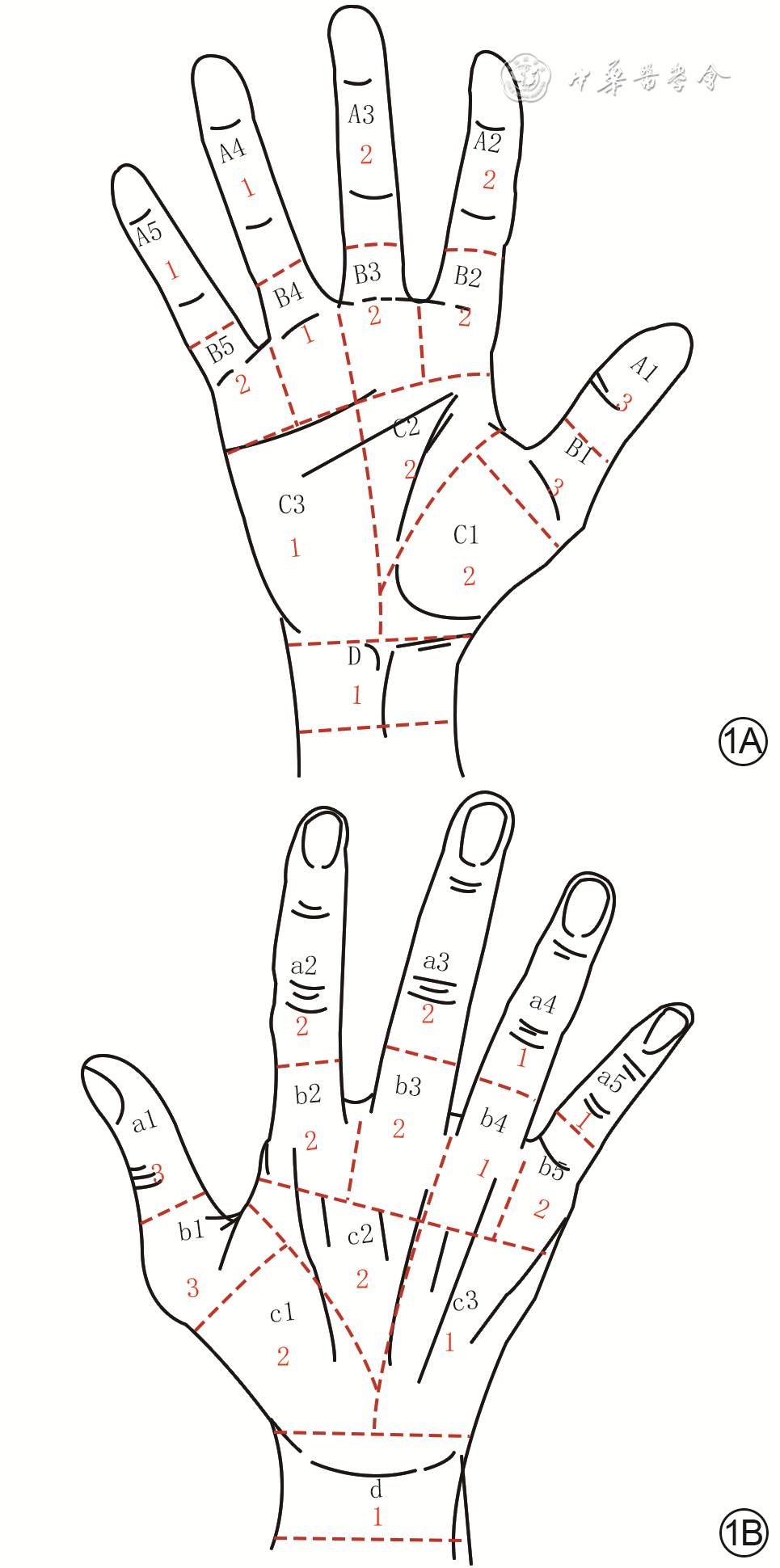
图 1 手部烧伤创面与瘢痕地形图评估系统。1A.手掌侧;1B.手背侧
注:手部由解剖标志线和水平线、垂直线共同分割为各区及各亚区;大写字母A、B、C、D分别代表手掌侧的指间关节区、掌指关节区、手掌区、腕关节区,小写字母a、b、c、d分别代表手背侧的指间关节区、掌指关节区、手背区、腕关节区;亚区标记由黑色字母或黑色字母与黑色数字的组合表示,红色数字代表各亚区权重

图 2 使用手部烧伤创面与瘢痕地形图评估系统评估1例右手烧伤患者创面情况。2A.手掌侧;2B.手背侧
注:手部表面的手形图及所有标记为手部烧伤创面与瘢痕地形图评估系统;手部由解剖标志线和水平线、垂直线共同分割为各区及各亚区;大写字母A、B、C、D分别代表手掌侧的指间关节区、掌指关节区、手掌区、腕关节区,小写字母a、b、c、d分别代表手背侧的指间关节区、掌指关节区、手背区、腕关节区;亚区标记由黑色字母或黑色字母与黑色数字的组合表示
Table 1. 手部烧伤创面与瘢痕地形图评估系统
一级条目 二级条目 三级条目 手部分区 整体分区原则 根据解剖和功能对手部进行分区 把手分为掌侧和背侧 手掌侧分区 手掌侧分为指间关节区(A)、掌指关节区(B)、手掌区(C)、腕关节区(D) 分界线:A区与B区分界线为近端指节中间线,B区与C区分界线为掌横纹,C区与D区分界线为腕横纹,腕横纹上3 cm为D区近端边界 亚区分界线1:以指蹼中间线为分界线将A区和B区各分为5个亚区(由拇指至小指依次为A1~A5、B1~B5) 亚区分界线2:以中环指指蹼中间线近侧延长线、虎口中点与第3掌骨基底部的连线为分界线将C区分为3个亚区,即大鱼际掌侧亚区(C1)、虎口掌侧亚区(C2)、小鱼际掌侧亚区(C3) 腕关节掌侧单独为1个区(D) 手背侧分区 手背侧分为指间关节区(a)、掌指关节区(b)、手背区(c)、腕关节区(d) 分界线:a区与b区分界线为近端指节背面中间线,b区与c区分界线为掌横纹手背对应线,c区与d区分界线为腕横纹手背对应线,腕横纹上3 cm手背对应线为d区近端边界 亚区分界线1:以指蹼背面中间线为分界线将a区和b区各分为5个亚区(由拇指至小指依次为a1~a5、b1~b5) 亚区分界线2:以中环指指蹼中间线近侧延长线、虎口中点与第3掌骨基底部的连线为分界线将c区分为3个亚区,即大鱼际背侧亚区(c1)、虎口背侧亚区(c2)、小鱼际背侧亚区(c3) 腕关节背侧单独为1个区(d) 亚区权重 手掌侧亚区 A1=3、A2=2、A3=2、A4=1、A5=1 B1=3、B2=2、B3=2、B4=1、B5=2 C1=2、C2=2、C3=1 D=1 手背侧亚区 a1=3、a2=2、a3=2、a4=1、a5=1 b1=3、b2=2、b3=2、b4=1、b5=2 c1=2、c2=2、c3=1 d=1 亚区系数 面积系数 若亚区内创面或瘢痕面积≥该亚区面积的1/3,则该亚区面积系数为1,否则面积系数为0 连续系数 若某亚区与2个或多个亚区创面或瘢痕连接在一起,则该亚区连续系数为2,否则连续系数为1 创面评估 深度评分 创面深度:Ⅰ度为1分,浅Ⅱ度为2分,深Ⅱ度为4分,Ⅲ度为5分,伤及肌肉或骨骼为6分 标准分计算方法 亚区粗分=亚区权重×创面深度评分×亚区连续系数×亚区面积系数,总粗分为各个亚区粗分之和 标准分=总粗分÷6(单手标准分最高为100分) 瘢痕评估 瘢痕血供与厚度评分 血供:正常为0分;轻度充血,粉红或暗红,按之轻微变色,放开后颜色恢复时间≥2.0 s为1分;中度充血,色红,按之变白较明显,放开后颜色恢复时间≥1.0 s且<2.0 s为2分;充血明显,鲜红,按之变白明显,放开后颜色恢复时间≥0.5 s且<1.0 s为3分;充血非常明显,按之变白非常明显,放开后颜色恢复时间<0.5 s为4分 厚度:无增厚为0分,<1 mm为1分,≥1 mm且<2 mm为2分,≥2 mm且<4 mm为3分,≥4 mm为4分 标准分计算方法 亚区粗分=亚区权重×(瘢痕厚度分值+瘢痕血供分值)×亚区连续系数×亚区面积系数,总粗分为各个亚区粗分之和 标准分=总粗分÷8(单手标准分最高为100分) 畸形与活动度评估 指蹼粘连 评估内容:虎口、示中指指蹼、中环指指蹼、环小指指蹼和拇小指掌指纹之间贯穿手掌的粘连情况 评估方法:手半握拳,通过观察指蹼下缘到达各节指骨的不同位置来确定分数 评分标准:指蹼下缘未达近节指骨中点为1分;指蹼下缘达近节指骨1/2,但未达3/4为2分;指蹼下缘达近节指骨3/4,但未达近端指间关节为3分;指蹼下缘达近端指间关节,但未达中节指骨(拇指末节)中点为4分;指蹼下缘达到或超过中节指骨中点为5分 手指主动活动度评估 评估内容:拇指主动屈伸、外展内收情况,其余手指主动屈伸情况 评估方法:使用直尺测量拇指主动外展内收时掌横纹桡侧端与拇指指间横纹尺侧端的距离较健侧下降幅度,手指主动屈伸时手指尖与掌横纹的距离较健侧下降幅度 评分标准:下降幅度<20%为1分,20%~40%为2分,41%~60%为3分,61%~80%为4分,≥81%为5分 手指畸形评估 评估内容:手指侧偏和旋转畸形 评估方法:使用量角器测量手指在自然状态下的侧偏角度,并观察手指旋转对功能的影响 评分标准:侧偏<10°,轻微旋转但不影响功能为1分;侧偏10~19°,旋转导致手指功能轻微受影响或在握拳时与其他手指产生摩擦为2分;侧偏20~40°,旋转明显影响对指功能或与其他手指交叠明显为3分;关节半脱位为4分;关节脱位为5分 腕关节屈伸畸形评估 评估内容:腕关节在自然状态下的屈曲或背伸角度 评估方法:使用量角器测量腕关节屈曲或背伸角度 评分标准:背伸角度50~69°或屈曲角度<20°为1分,背伸角度70~89°或屈曲角度20~29°为2分,背伸角度90~109°或屈曲角度30~59°为3分,背伸角度110~119°或屈曲角度60~89°为4分,背伸角度≥120°或屈曲角度≥90°为5分 腕关节侧偏畸形评估 评估内容:腕关节在自然状态下的侧偏角度 评估方法:使用量角器测量腕关节侧偏角度 评分标准:侧偏角度<20°为1分,20~39°为2分,40~59°为3分,60~79°为4分,≥80°为5分  下载: 导出CSV
下载: 导出CSV
-

 下载:
下载:


图(3) / 表(1)
计量
- 文章访问数: 2962
- HTML全文浏览量: 827
- PDF下载量: 16
- 被引次数: 0
