




Value of the CD177/CD10 ratio in neutrophils in predicting infection risk in burn patients and the establishment of its normal reference range
-
摘要:
目的 探讨中性粒细胞中CD177水平与CD10水平的比值(以下简称CD177/CD10比)在烧伤患者感染风险预测中的价值,并建立其正常参考值范围。 方法 该研究为横断面研究。2023年2月—2025年11月,南京医科大学附属苏州医院收治61例符合入选标准的烧伤患者,其中男52例、女9例,年龄41.0(32.0,55.0)岁,其中59例患者进行了伤后1 d急性应激期炎症指标监测,48例患者进行了伤后3~14 d感染高风险期炎症指标监测(以下简称高风险期监测);同期招募于该单位体检中心体检且结果正常的204名健康志愿者,其中男110人、女94人,年龄47.5(31.0,67.0)岁。利用流式细胞术监测患者伤后1、3、5、7、10、14 d和健康志愿者的中性粒细胞中CD177和CD10的水平。根据是否发生感染,将行高风险期监测的患者分为感染组(31例)和非感染组(17例),比较2组患者入院时烧伤总面积等一般资料,白细胞计数、中性粒细胞计数、中性粒细胞、C反应蛋白水平、降钙素原水平、CD177水平、CD10水平、CD177/CD10比等炎症指标,以及序贯器官衰竭评估(SOFA)评分,筛选影响行高风险期监测的患者发生感染的危险因素,其中感染组患者取确诊感染前最近一次的检测数据,非感染组患者取伤后3~14 d检测的最高值进行分析(选取数据后同)。采用受试者操作特征(ROC)曲线,评估前述炎症指标及SOFA评分对行高风险期监测的患者感染风险的预测价值。分析行高风险期监测的患者CD177水平与CD10水平的相关性,比较健康志愿者、患者急性应激期及感染高风险期CD177水平、CD10水平与CD177/CD10比。基于健康志愿者数据,采用非参数百分位数法建立CD177/CD10比的正常参考值范围。 结果 感染组与非感染组患者在烧伤总面积、C反应蛋白水平、SOFA评分、CD177水平、CD10水平、CD177/CD10比方面比较,差异均有统计学意义(Z值分别为-2.08、-2.58、0.04、-2.72、-2.86、-3.20,P<0.05)。单因素logistic回归分析结果显示,烧伤总面积和lg(CD177/CD10比)均是行高风险期监测的患者发生感染的危险因素(OR分别为1.03、6.91,95%CI分别为1.00~1.06、1.84~25.91,P<0.05);多因素logistic回归分析结果显示,lg(CD177/CD10比)是行高风险期监测的患者发生感染的独立危险因素(OR=5.73,95%CI为1.11~29.60,P<0.05)。ROC曲线分析显示,CD177/CD10比预测行高风险期监测的患者感染风险的曲线下面积最大,为0.78(95%CI为0.65~0.91),其最佳截断值为3.84,最佳截断值下的敏感度、特异度、准确度、阳性预测值、阴性预测值分别为58.06%、94.12%、76.09%、94.74%、55.17%。在行高风险期监测的患者中,CD177水平与CD10水平呈显著负相关(r=-0.60,P<0.05)。与健康志愿者、患者急性应激期比较,患者感染高风险期CD10水平显著降低(P值均<0.05),CD177水平与CD177/CD10比均显著升高(P<0.05)。建立的CD177/CD10比的正常参考值范围为0~0.64。 结论 中性粒细胞中CD177/CD10比对烧伤患者感染风险具有一定的预测价值,预测价值高于白细胞计数、中性粒细胞计数、中性粒细胞、C反应蛋白水平、降钙素原水平和SOFA评分。建立的CD177/CD10比的正常参考值范围为0~0.64。 Abstract:Objective To explore the value of the ratio of CD177 level to CD10 level (hereinafter referred to as CD177/CD10 ratio) in neutrophils in predicting infection risk in burn patients, and to establish its normal reference range. Methods This study was a cross-sectional study. From February 2023 to November 2025, 61 burn patients who met the inclusion criteria were admitted to Affiliated Suzhou Hospital of Nanjing Medical University, including 52 males and 9 females, aged 41.0 (32.0, 55.0) years. Among them, 59 patients underwent inflammatory marker monitoring during the acute stress period on post injury day 1, and 48 patients underwent inflammatory marker monitoring during the high-risk period for infection (hereinafter referred to as high-risk period monitoring) from post injury day 3 to 14. During the same period, 204 healthy volunteers who underwent physical examinations in the physical examination center of the same unit with normal examination results were recruited, including 110 males and 94 females, aged 47.5 (31.0, 67.0) years. Flow cytometry was used to monitor the levels of CD177 and CD10 in the neutrophils from patients on post injury day 1, 3, 5, 7, 10, and 14, as well as from healthy volunteers. According to whether infection occurred, the patients who underwent high-risk period monitoring were divided into infection group (n=31) and non-infection group (n=17). General information such as total burn area at admission, as well as inflammatory markers such as the white blood cell count, neutrophil count, neutrophil, C-reactive protein level, procalcitonin level, CD177 level, CD10 level, and CD177/CD10 ratio, and sequential organ failure assessment (SOFA) scores were compared between the two groups of patients to screen for risk factors affecting the occurrence of infection in patients undergoing high-risk period monitoring. For patients in infection group, the most recent detection data before the confirmed infection was taken for analysis, and for patients in non-infection group, the highest values detected from post injury day 3 to 14 were taken for analysis (the same data selection below). The receiver operating characteristic (ROC) curve was used to evaluate the predictive value of the aforementioned inflammatory markers and SOFA score for the infection risk in patients undergoing high-risk period monitoring. The correlation between CD177 level and CD10 level in patients undergoing high-risk period monitoring was analyzed. The CD177 level, CD10 level, and CD177/CD10 ratio were compared among healthy volunteers, patients during the acute stress period and high-risk period for infection. Based on the data of healthy volunteers, the normal reference range for the CD177/CD10 ratio was established using the non-parametric percentile method. Results There were statistically significant differences between patients in infection group and non-infection group in terms of total burn area, C-reactive protein level, SOFA score, CD177 level, CD10 level, and CD177/CD10 ratio (with Z values of -2.08, -2.58, 0.04, -2.72, -2.86, and -3.20, respectively, P<0.05). The results of univariate logistic regression analysis showed that both total burn area and the lg (CD177/CD10 ratio) were risk factors for infection in patients undergoing high-risk period monitoring (with ORs of 1.03 and 6.91, respectively, 95%CIs of 1.00 to 1.06 and 1.84 to 25.91, respectively, P<0.05). The results of multivariate logistic regression analysis showed that the lg (CD177/CD10 ratio) was an independent risk factor for infection in patients undergoing high-risk period monitoring (OR=5.73, with a 95%CI of 1.11 to 29.60, P<0.05). ROC curve analysis showed that the CD177/CD10 ratio had the largest area under the curve for predicting the infection risk in patients undergoing high-risk period monitoring, which was 0.78 (with a 95%CI of 0.65 to 0.91). Its optimal cut-off value was 3.84, with the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value at the optimal cut-off value being 58.06%, 94.12%, 76.09%, 94.74%, and 55.17%, respectively. In patients undergoing high-risk period monitoring, the CD177 level was significantly negatively correlated with the CD10 level (r=-0.60, P<0.05). Compared with those of healthy volunteers and patients in the acute stress period, the CD10 level of patients in the high-risk period for infection was significantly decreased (with P values both <0.05), while the CD177 level and the CD177/CD10 ratio were significantly increased (P<0.05). The established normal reference range for the CD177/CD10 ratio was 0-0.64. Conclusions The CD177/CD10 ratio in neutrophils has a certain predictive value for the infection risk in burn patients, and its predictive value is higher than that of white blood cell count, neutrophil count, neutrophil, C-reactive protein level, procalcitonin level, and SOFA score. The established normal reference range for the CD177/CD10 ratio is 0-0.64. -
Key words:
- Burns /
- Infection /
- Forecasting /
- Neutrophils /
- Ratio of CD177 level to CD10 level /
- Risk assessment
-
参考文献
(41) [1] 罗高兴,詹日兴,袁志强,等.浅谈烧伤感染的分类与诊断命名[J].中华烧伤与创面修复杂志,2023,39(4):301-304.DOI: 10.3760/cma.j.cn501225-20221206-00528. [2] ŻwierełłoW,PiorunK,Skórka-MajewiczM,et al.Burns: classification, pathophysiology, and treatment: a review[J].Int J Mol Sci,2023,24(4):3749.DOI: 10.3390/ijms24043749. [3] Radzikowska-BüchnerE,ŁopuszyńskaI,FliegerW,et al.An overview of recent developments in the management of burn injuries[J].Int J Mol Sci,2023,24(22):16357.DOI: 10.3390/ijms242216357. [4] BurgessM,ValderaF,VaronD,et al.The immune and regenerative response to burn injury[J].Cells,2022,11(19):3073.DOI: 10.3390/cells11193073. [5] SikoraJP,KarawaniJ,SobczakJ.Neutrophils and the systemic inflammatory response syndrome (SIRS)[J].Int J Mol Sci,2023,24(17):13469.DOI: 10.3390/ijms241713469. [6] KimHS,KimJH,YimH,et al.Changes in the levels of interleukins 6, 8, and 10, tumor necrosis factor alpha, and granulocyte-colony stimulating factor in Korean burn patients: relation to burn size and postburn time[J].Ann Lab Med,2012,32(5):339-344.DOI: 10.3343/alm.2012.32.5.339. [7] SierawskaO,MałkowskaP,TaskinC,et al.Innate immune system response to burn damage-focus on cytokine alteration[J].Int J Mol Sci,2022,23(2):716.DOI: 10.3390/ijms23020716. [8] ZhangP,ZouB,LiouYC,et al.The pathogenesis and diagnosis of sepsis post burn injury[J/OL].Burns Trauma,2021,9:tkaa047[2025-11-18].https://pubmed.ncbi.nlm.nih.gov/33654698/.DOI: 10.1093/burnst/tkaa047. [9] KorkmazHI,FlokstraG,WaasdorpM,et al.The complexity of the post-burn immune response: an overview of the associated local and systemic complications[J].Cells,2023,12(3):345.DOI: 10.3390/cells12030345. [10] DobsonGP,MorrisJL,LetsonHL.Pathophysiology of severe burn injuries: new therapeutic opportunities from a systems perspective[J].J Burn Care Res,2024,45(4):1041-1050.DOI: 10.1093/jbcr/irae049. [11] SprostonNR,AshworthJJ.Role of C-reactive protein at sites of inflammation and infection[J].Front Immunol,2018,9:754.DOI: 10.3389/fimmu.2018.00754. [12] CabralL,AfreixoV,SantosF,et al.Procalcitonin for the early diagnosis of sepsis in burn patients: a retrospective study[J].Burns,2017,43(7):1427-1434.DOI: 10.1016/j.burns.2017.03.026. [13] ChuangCL,YehHT,NiuKY,et al.Diagnostic performances of procalcitonin and C-reactive protein for sepsis: a systematic review and meta-analysis[J].Eur J Emerg Med,2025,32(4):248-258.DOI: 10.1097/MEJ.0000000000001235. [14] PalmieriTL,HeardJ.Biomarkers of sepsis in burn injury: an update[J/OL].Burns Trauma,2025,13:tkae080[2025-11-18].https://pubmed.ncbi.nlm.nih.gov/39822649/.DOI: 10.1093/burnst/tkae080. [15] HuangJ,ChenY,GuoZ,et al.Prospective study and validation of early warning marker discovery based on integrating multi-omics analysis in severe burn patients with sepsis[J/OL].Burns Trauma,2023,11:tkac050[2025-11-18].https://pubmed.ncbi.nlm.nih.gov/36659877/.DOI: 10.1093/burnst/tkac050. [16] HuangJ,XieK,LiH,et al.Dynamic CD177/CD10 ratio for infection diagnosis and mortality risk stratification in critically ill patients: a prospective cohort study[J].EBioMedicine,2026,123:106100.DOI: 10.1016/j.ebiom.2025.106100. [17] ZhengC,LiJ,ChenH,et al.Dual role of CD177 + neutrophils in inflammatory bowel disease: a review[J].J Transl Med,2024,22(1):813.DOI: 10.1186/s12967-024-05539-3. [18] KaiserR,GoldC,JoppichM,et al.Peripheral priming induces plastic transcriptomic and proteomic responses in circulating neutrophils required for pathogen containment[J].Sci Adv,2024,10(12):eadl1710.DOI: 10.1126/sciadv.adl1710. [19] MariniO,CostaS,BevilacquaD,et al.Mature CD10+ and immature CD10- neutrophils present in G-CSF-treated donors display opposite effects on T cells[J].Blood,2017,129(10):1343-1356.DOI: 10.1182/blood-2016-04-713206. [20] LiuM,WangG,WangL,et al.Immunoregulatory functions of mature CD10+ and immature CD10- neutrophils in sepsis patients[J].Front Med (Lausanne),2023,9:1100756.DOI: 10.3389/fmed.2022.1100756. [21] 中华医学会烧伤外科学分会,海峡两岸医药卫生交流协会暨烧创伤组织修复专委会.Ⅱ度烧伤创面治疗专家共识(2024版)Ⅰ:院前急救和非手术治疗[J].中华烧伤与创面修复杂志,2024,40(1):1-18.DOI: 10.3760/cmaj.cn501225-20231019-00120. [22] 中国医师协会烧伤医师分会《烧伤感染诊治指南》编辑委员会.烧伤感染的诊断标准与治疗指南(2012版)[J].中华烧伤杂志,2012,28(6):401-403.DOI: 10.3760/cma.j.issn.1009-2587.2012.06.001. [23] 朱伟,彭毅志,罗高兴,等.2023版国际烧伤学会《拯救烧伤脓毒症运动指南》解读[J].中华烧伤与创面修复杂志,2025,41(8):803-810.DOI: 10.3760/cma.j.cn501225-20250403-00164. [24] TsolakidisS,FreytagDL,DovernE,et al.Infections in burn patients: a retrospective view over seven years[J].Medicina (Kaunas),2022,58(8):1066.DOI: 10.3390/medicina58081066. [25] JeschkeMG,van BaarME,ChoudhryMA,et al.Burn injury[J].Nat Rev Dis Primers,2020,6(1):11.DOI: 10.1038/s41572-020-0145-5. [26] LadhaniHA,YowlerCJ,ClaridgeJA.Burn wound colonization, infection, and sepsis[J].Surg Infect (Larchmt),2021,22(1):44-48.DOI: 10.1089/sur.2020.346. [27] ChenWA,BoskovicDS.Neutrophil extracellular DNA traps in response to infection or inflammation, and the roles of platelet interactions[J].Int J Mol Sci,2024,25(5):3025.DOI: 10.3390/ijms25053025. [28] BurnGL,FotiA,MarsmanG,et al.The neutrophil[J].Immunity,2021,54(7):1377-1391.DOI: 10.1016/j.immuni.2021.06.006. [29] Marsile-MedunS,SouchardM,Abba MoussaD,et al.Fc receptors are key discriminatory markers of granulocytes subsets in people living with HIV-1[J].Front Immunol,2024,15:1345422.DOI: 10.3389/fimmu.2024.1345422. [30] GaoH,PengK,ShiY,et al.Development and validation of a novel criterion of histologic healing in ulcerative colitis defined by inflammatory cell enumeration in lamina propria mucosa: a multicenter retrospective cohort in China[J].Chin Med J (Engl),2024,137(11):1316-1323.DOI: 10.1097/CM9.0000000000003154. [31] JeffreyM,DennyKJ,LipmanJ,et al.Differentiating infection, colonisation, and sterile inflammation in critical illness: the emerging role of host-response profiling[J].Intensive Care Med,2023,49(7):760-771.DOI: 10.1007/s00134-023-07108-6. [32] NourigheimasiS,YazdaniE,GhaediA,et al.Association of inflammatory biomarkers with overall survival in burn patients: a systematic review and meta-analysis[J].BMC Emerg Med,2024,24(1):76.DOI: 10.1186/s12873-024-00988-x. [33] ZhiL,WangX,PanX,et al.The asynchronous dynamic changes and interrelationships between leukocyte composition and inflammatory markers and potential clinical significance in the early stage and sepsis stage in severe burns[J].Burns,2024,50(7):1752-1761.DOI: 10.1016/j.burns.2024.04.006. [34] LiAT,MoussaA,GusE,et al.Biomarkers for the early diagnosis of sepsis in burns: systematic review and meta-analysis[J].Ann Surg,2022,275(4):654-662.DOI: 10.1097/SLA.0000000000005198. [35] 李晓明,吴桂新,李蕊,等.中性粒细胞CD64在细菌感染诊疗及评估检测中的临床应用价值[J].中华消化外科杂志,2025,24(11):1496-1500.DOI: 10.3760/cma.j.cn115610-20251021-00645. [36] 姚咏明,栾樱译.严重烧创伤感染及其并发症的免疫新认识[J].中华烧伤杂志,2021,37(6):519-523.DOI: 10.3760/cma.j.cn501120-20210118-00025. [37] YuanY,XiaoY,ZhaoJ,et al.Exosomes as novel biomarkers in sepsis and sepsis related organ failure[J].J Transl Med,2024,22(1):1078.DOI: 10.1186/s12967-024-05817-0. [38] DemaretJ,VenetF,PlassaisJ,et al.Identification of CD177 as the most dysregulated parameter in a microarray study of purified neutrophils from septic shock patients[J].Immunol Lett,2016,178:122-130.DOI: 10.1016/j.imlet.2016.08.011. [39] ZhuJ,ZhouJ,LiangX,et al.Elevated CD10- neutrophils correlate with non-response and poor prognosis of CD19 CAR T-cell therapy for B-cell acute lymphoblastic leukemia[J].BMC Med,2025,23(1):138.DOI: 10.1186/s12916-025-03968-5. [40] LiD,WeiY,ZhangC,et al.Value of SOFA score, APACHE II score, and WBC count for mortality risk assessment in septic patients: a retrospective study[J].Medicine (Baltimore),2025,104(20):e42464.DOI: 10.1097/MD.0000000000042464. [41] Padarabinda TripathyK,ChaitanyaY,BeheraPK,et al.Correlation between platelet indices and severity of sepsis: a hospital-based prospective study[J].Cureus,2025,17(4):e82816.DOI: 10.7759/cureus.82816. -

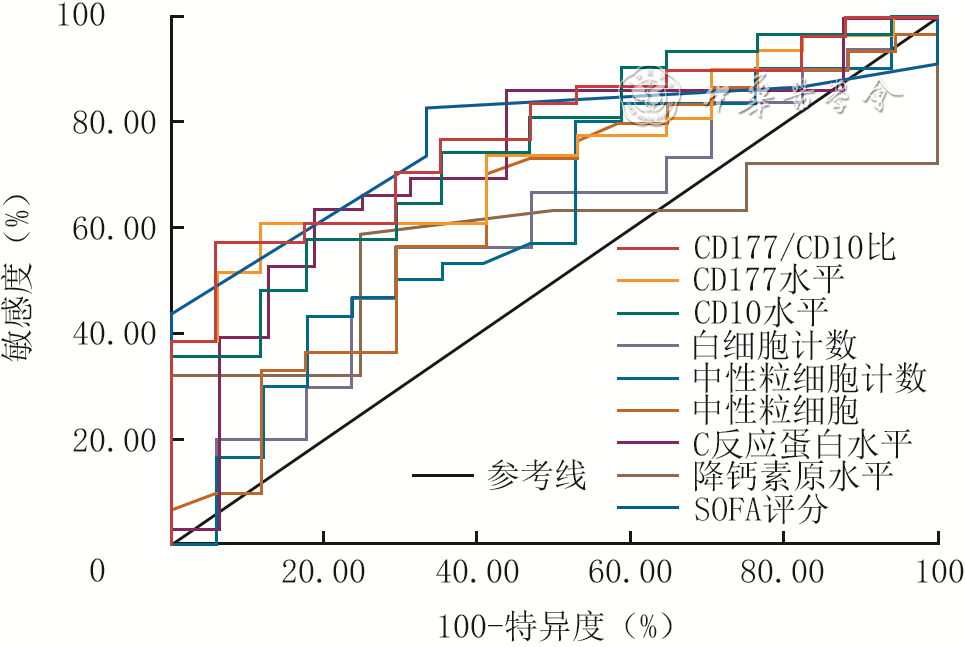
图 1 炎症指标及SOFA评分预测48例行感染高风险期炎症指标监测烧伤患者感染风险的受试者操作特征曲线
注:CD177/CD10比为CD177水平与CD10水平的比值,SOFA为序贯器官衰竭评估;感染患者取确诊感染前最近一次的检测数据,非感染患者取伤后3~14 d检测的最高值进行分析

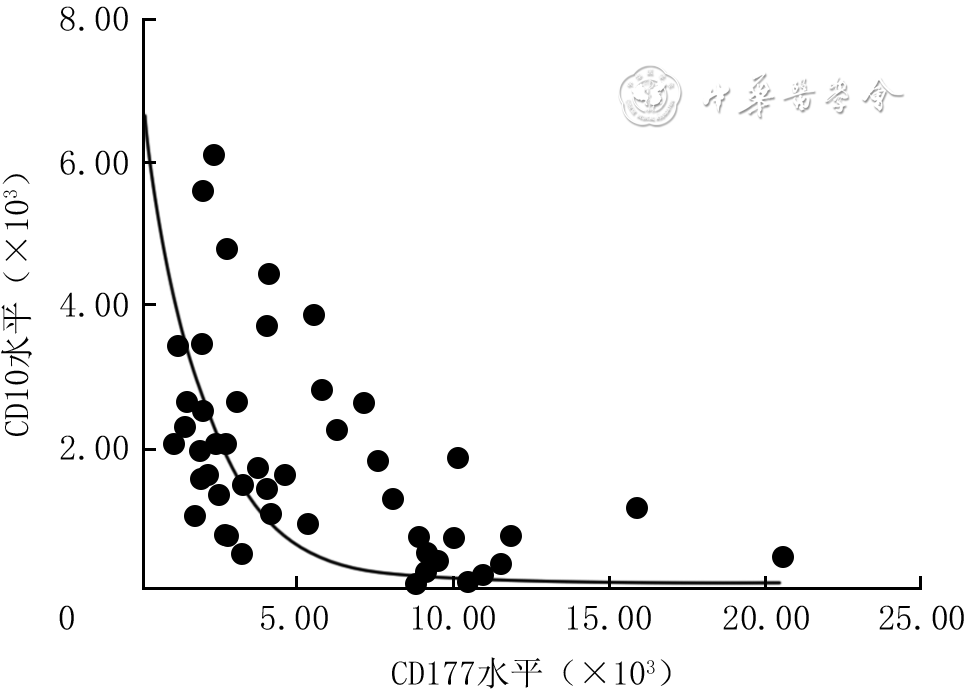
图 2 48例行感染高风险期炎症指标监测烧伤患者CD177水平与CD10水平的相关性
注:感染患者取确诊感染前最近一次的检测数据,非感染患者取伤后3~14 d检测的最高值进行分析;CD177水平与CD10水平呈显著负相关,r=-0.60,P<0.001
Table 1. 2组烧伤患者的临床和实验室检测指标比较
组别 例数 性别(例) 年龄[岁,M(Q1,Q3)] 烧伤总面积[%TBSA,M(Q1,Q3)] 早期手术情况(例) 白细胞计数[×109/L,M(Q1,Q3)] 中性粒细胞计数[×109/L,M(Q1,Q3)] 男 女 是 否 感染组 31 28 3 44.0(34.0,57.0) 38.0(10.0,70.0) 24 7 12.53(10.65,15.46) 10.91(9.24,13.61) 非感染组 17 12 5 36.0(32.0,54.5) 25.0(2.0,35.0) 13 4 11.54(9.61,13.78) 9.79(7.54,11.43) 统计量值 χ2=0.31 Z=-0.69 Z=-2.08 χ2=0.01 Z=-1.06 Z=-1.34 P值 0.079 0.490 0.037 0.940 0.288 0.180 注:TBSA为体表总面积,SOFA为序贯器官衰竭评估,CD177/CD10比为CD177水平与CD10水平的比值;性别、年龄、烧伤总面积为入院时数据,早期手术情况为首次采血前数据;其余指标中,感染组患者为确诊感染前最近一次的检测数据,非感染组患者为伤后3~14 d检测的最高值  下载: 导出CSV
下载: 导出CSV
Table 2. 48例行感染高风险期炎症指标监测烧伤患者感染风险影响因素的单因素及多因素logistic回归分析结果
分类及变量 β值 标准误 Wald值 OR 95%CI P值 单因素logistic回归分析 lg(CD177/CD10比) 1.93 0.68 8.21 6.91 1.84~25.91 0.004 早期手术情况 -0.05 0.72 0.01 0.95 0.23~3.86 0.940 烧伤总面积(%TBSA) 0.03 0.01 5.03 1.03 1.00~1.06 0.025 年龄(岁) 0.01 0.02 0.45 1.01 0.98~1.05 0.505 多因素logistic回归分析 lg(CD177/CD10比) 1.75 0.84 4.34 5.73 1.11~29.60 0.037 烧伤总面积(%TBSA) 0.01 0.02 0.13 1.01 0.97~1.05 0.723 注:TBSA为体表总面积;分析时,早期手术情况取首次采血前数据,年龄、烧伤总面积取入院时数据;CD177水平与CD10水平的比值(CD177/CD10比)中,感染患者取确诊感染前最近一次的检测数据,非感染患者取伤后3~14 d检测的最高值
下载: 导出CSV
Table 3. 炎症指标及SOFA评分对48例行感染高风险期炎症指标监测烧伤患者感染风险的预测价值比较
指标 AUC 95%CI 最佳截断值 约登指数 敏感度(%) 特异度(%) 准确度(%) 阳性预测值(%) 阴性预测值(%) CD177/CD10比 0.78 0.65~0.91 3.84 0.52 58.06 94.12 76.09 94.74 55.17 CD177水平 0.74 0.60~0.88 4 384.00 0.50 61.29 88.24 74.77 90.48 55.56 CD10水平 0.75 0.61~0.89 1 298.00 0.40 58.06 82.35 70.21 85.71 51.85 白细胞计数(×109/L) 0.59 0.42~0.76 12.03 0.27 56.67 70.59 63.63 77.85 47.18 中性粒细胞计数(×109/L) 0.62 0.45~0.79 9.08 0.27 80.00 47.06 63.53 73.37 56.34 中性粒细胞 0.64 0.47~0.80 81.85 0.29 70.00 58.82 64.41 75.61 51.81 C反应蛋白水平(mg/L) 0.73 0.58~0.89 103.10 0.45 63.33 81.25 72.29 86.03 54.85 降钙素原水平(ng/mL) 0.57 0.34~0.81 0.31 0.34 59.09 75.00 67.05 81.17 50.13 SOFA评分(分) 0.77 0.59~0.95 2.50 0.49 82.61 66.67 74.64 81.88 67.77 注:CD177/CD10比为CD177水平与CD10水平的比值,SOFA为序贯器官衰竭评估,AUC为曲线下面积;感染患者取确诊感染前最近一次的检测数据,非感染患者取伤后3~14 d检测的最高值进行分析
下载: 导出CSV
Table 4. 健康志愿者、烧伤患者急性应激期及感染高风险期CD177水平、CD10水平与CD177/CD10比的比较[M(Q1,Q3)]
分类与分期 人数/例数 CD177水平 CD10水平 CD177/CD10比 健康志愿者 204 1 529.00(1 018.75,2 182.00) 5 114.25(4 008.75,6 320.25) 0.31(0.20,0.45) 烧伤患者 急性应激期 59 1 904.50(1 261.75,2 432.50) 3 145.50(2 250.50,4 688.75) 0.53(0.30,0.98) 感染高风险期 48 4 019.00(2 321.50,9 047.25) 1 574.75(736.38,2 597.50) 2.72(1.10,13.36) H值 67.71 109.85 114.45 P值 <0.001 <0.001 <0.001 P1值 0.073 <0.001 <0.001 P2值 <0.001 <0.001 <0.001 P3值 <0.001 0.001 <0.001 注:急性应激期取伤后1 d的检测数据;感染高风险期中感染患者取确诊感染前最近一次的检测数据,非感染患者取伤后3~14 d检测的最高值;CD177/CD10比为CD177水平与CD10水平的比值;H值、P值为健康志愿者与烧伤患者2个时期各指标总体比较所得,P1值、P2值分别为健康志愿者与烧伤患者急性应激期、感染高风险期各指标比较所得,P3值为烧伤患者急性应激期与感染高风险期各指标比较所得
下载: 导出CSV
Table 5. 不同性别健康志愿者CD177水平、CD10水平和CD177/CD10比的比较[M(Q1,Q3)]
性别 人数 CD177水平 CD10水平 CD177/CD10比 男 110 1 508.00(948.75,2 211.50) 5 053.25(3 660.00,6 305.75) 0.30(0.20,0.45) 女 94 1 580.75(1 118.88,2 142.38) 5 242.25(4 401.38,6 379.63) 0.33(0.20,0.45) Z值 -1.00 -1.08 -0.42 P值 0.316 0.281 0.675 注:CD177/CD10比为CD177水平与CD10水平的比值
下载: 导出CSV
Table 6. 不同年龄段健康志愿者CD177水平、CD10水平和CD177/CD10比的比较[M(Q1,Q3)]
年龄段(岁) 人数 CD177水平 CD10水平 CD177/CD10比 20~29 45 1 441.50(948.25,2 060.50) 5 577.50(4 545.25,6 261.25) 0.24(0.18,0.40) 30~39 39 1 665.00(1 230.50,2 323.50) 5 441.00(4 149.00,6 683.00) 0.24(0.21,0.50) 40~49 28 1 475.25(986.75,2 169.75) 4 515.25(3 336.13,6 283.88) 0.32(0.23,0.45) 50~59 33 1 374.00(1 010.75,2 031.75) 5 384.67(3 698.25,6 687.50) 0.26(0.18,0.40) ≥60 59 1 728.50(1 052.00,2 230.00) 5 031.00(3 550.00,6 135.50) 0.36(0.23,0.49) H值 6.85 5.16 8.71 P值 0.144 0.271 0.069 注:CD177/CD10比为CD177水平与CD10水平的比值
下载: 导出CSV
-
 李和玥 6月3日.mp4
李和玥 6月3日.mp4

-

 下载:
下载:




计量
- 文章访问数: 306
- HTML全文浏览量: 175
- PDF下载量: 28
- 被引次数: 0
