




Analysis of the characteristics and changing trends of burn disease burden in the Chinese population based on the GBD 2021 database
-
摘要:
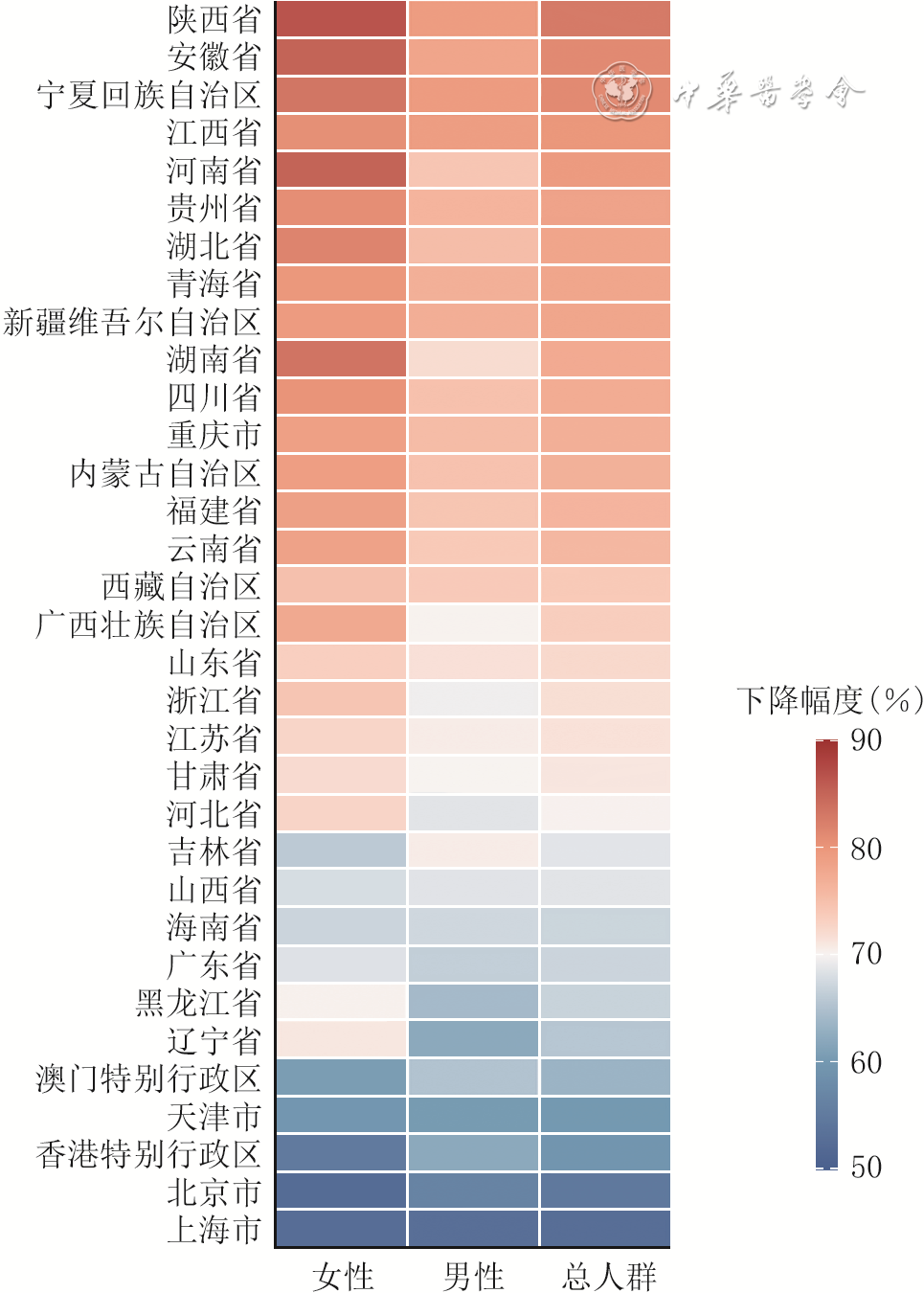
目的 基于全球疾病负担(GBD)2021数据库,分析中国人群烧伤疾病负担特征与变化趋势。 方法 该研究为基于公共数据库的二次研究。提取GBD 2021数据库中1990—2021年除台湾地区外的中国22个省、5个自治区、4个直辖市以及香港特别行政区、澳门特别行政区由“火、高温及热物质”所致烧伤相关数据。按性别、年龄段和省级行政区进行分层,采用伤残调整生命年(DALY)率、早死所致生命年损失(YLL)率、失能所致生命年损失(YLD)率及其年龄标化率评价烧伤疾病负担。比较1990—2021年中国不同性别、年龄段和省级行政区人群的烧伤疾病负担变化趋势,并评价2021年中国不同性别、年龄段和省级行政区人群的烧伤疾病负担情况。 结果 1990—2021年,中国人群烧伤疾病负担整体下降。中国人群总体烧伤年龄标化DALY率(95%UI)由1990年的135.6(109.8~158.4)×10-⁵降至2021年的33.6(27.0~41.8)×10-⁵,下降幅度为75.2%;烧伤年龄标化YLL率和烧伤年龄标化YLD率亦下降,下降幅度分别为81.4%和54.5%。与1990年相比,2021年各省级行政区烧伤年龄标化DALY率均下降,但下降幅度存在差异;25个省级行政区女性烧伤年龄标化DALY率下降幅度较男性更明显,8个省级行政区呈相反特征;1~<2岁低龄儿童烧伤DALY率下降较快,≥80岁高龄人群烧伤DALY率下降相对缓慢。2021年,中国不同性别、年龄段和省级行政区人群的烧伤疾病负担存在差异。各年龄段男性烧伤DALY率均高于女性。年龄段分层中,≥80岁年龄段烧伤DALY率(95%UI)最高,为147.3(114.5~176.3)×10-⁵。2021年,烧伤年龄标化DALY率(95%UI)前3位省级行政区从高到低依次为云南省、贵州省和上海市,分别为45.4(37.2~58.7)×10-⁵、43.8(34.3~55.4)×10-⁵和43.3(29.6~62.2)×10-⁵。 结论 1990—2021年中国烧伤疾病负担总体呈下降趋势。然而,男性、低龄儿童、高龄人群及云南省、贵州省等高烧伤疾病负担省级行政区人群仍应作为烧伤防控的重点对象。 Abstract:Objective To analyze the characteristics and changing trends of burn disease burden in the Chinese population based on the Global Burden of Disease (GBD) 2021 database. Methods This study was a secondary study based on public databases. Data related to burns caused by "fire, heat, and hot substances" in 22 provinces, 5 autonomous regions, 4 municipalities, Hong Kong Special Administrative Region, and Macao Special Administrative Region of China except for the Taiwan region of China from 1990 to 2021 were extracted from the GBD 2021 database. Stratified analyses were conducted by gender, age bracket, and provincial-level administrative region. Disability-adjusted life year (DALY) rate, years of life lost (YLL) rate, years lived with disability (YLD) rate, and their age-standardized rates were used to evaluate the burn disease burden. The changing trends of burn disease burden among populations across different genders, age brackets and provincial-level administrative regions in China from 1990 to 2021 were compared. The burn disease burden among populations across different genders, age brackets and provincial-level administrative regions in China in 2021 was evaluated. Results From 1990 to 2021, the burn disease burden in the Chinese population decreased overall. The overall age-standardized DALY rate (95% UI) of burns in the Chinese population decreased from 135.6 (109.8-158.4)×10-5 in 1990 to 33.6 (27.0-41.8)×10-5 in 2021, with a decline of 75.2%. The age-standardized YLL rate and age-standardized YLD rate of burns also decreased, with declines of 81.4% and 54.5%, respectively. Compared with that in 1990, the age-standardized DALY rates of burns in all provincial-level administrative regions decreased in 2021, but the magnitudes of decline varied. In 25 provincial-level administrative regions, the decline in age-standardized DALY rate of burns was more pronounced in women than in men, whereas the opposite pattern was observed in 8 provincial-level administrative regions. The burn DALY rate decreased relatively rapidly in young children aged 1 to <2 years, while it decreased relatively slowly in the oldest-old population aged ≥80 years. In 2021, differences in burn disease burden were observed among populations across different genders, age brackets and provincial-level administrative regions in China. In all age brackets, burn DALY rates in men were higher than those in women. Among age brackets, the burn DALY rate (95% UI) was the highest in the ≥80 years age bracket, at 147.3 (114.5-176.3)×10-5. In 2021, the top 3 provincial-level administrative regions with relatively high age-standardized DALY rates of burns, in descending order, were Yunnan Province, Guizhou Province, and Shanghai, with values of 45.4 (37.2-58.7)×10-5, 43.8 (34.3-55.4)×10-5, and 43.3 (29.6-62.2)×10-5, respectively. Conclusions From 1990 to 2021, the burn disease burden in China showed an overall downward trend. However, men, young children, the oldest-old population, and population in provincial-level administrative regions with high burn disease burden, such as Yunnan Province and Guizhou Province, should still be regarded as key targets for burn prevention and control. -
Key words:
- Burns /
- China /
- Age factors /
- Sex factors /
- Time factors /
- Global Burden of Disease /
- Disability-adjusted life year
-
参考文献
(38) [1] 吴军, 陈昭宏, 王玉振. 中国烧伤医学领域临床试验现状和思考[J]. 中华烧伤与创面修复杂志, 2022,38(9):799-804.DOI: 10.3760/cma.j.cn501120-20210909-00309. [2] BichCS, KostevK, BausA, et al. Burn injury and incidence of psychiatric disorders: a retrospective cohort study of 18,198 patients from Germany[J]. Burns, 2021,47(5):1110-1117.DOI: 10.1016/j.burns.2020.06.015. [3] World Health Organization Burns 2023 2023-10-13 2024-11-12 https://www.who.int/news-room/fact-sheets/detail/burns World Health Organization. Burns[EB/OL]. 2023(2023-10-13)[2024-11-12]. https://www.who.int/news-room/fact-sheets/detail/burns.
[4] YakupuA,ZhangJ,DongW,et al.The epidemiological characteristic and trends of burns globally[J].BMC Public Health,2022,22(1):1596.DOI: 10.1186/s12889-022-13887-2. [5] KeshriVR. Prioritising burn prevention within Sustainable Development Goals[J/OL]. Inj Prev, 2026:ip-2025-046024(2026-03-30)[2026-05-15]. https://pubmed.ncbi.nlm.nih.gov/41912320/.DOI:10.1136/ip-2025-046024.[published online ahead of print]. [6] ChuaM,Damkat-ThomasL,GabbeBJ,et al.Characteristics and outcomes of patients who discharge against medical advice from Australian and New Zealand burns services[J].Burns,2026,52(3):107850.DOI: 10.1016/j.burns.2026.107850. [7] GarsideT, UdyA, ReadeMC, et al. Variations in outcomes following burn injury and admission to an Australian or New Zealand intensive care unit: a retrospective data linkage cohort study[J]. Burns, 2026,52(5):107992.DOI: 10.1016/j.burns.2026.107992. [8] HongR, PerkinsM, GabbeBJ, et al. Comparing peak burn injury times and characteristics in Australia and New Zealand[J]. Int J Environ Res Public Health, 2022,19(15):9578.DOI: 10.3390/ijerph19159578. [9] HuangS,LinHZ,WeiX.Global, regional and national burden of injuries caused by fire, heat, and hot substances from 1990 to 2021[J].PLoS One,2025,20(5):e0324481.DOI: 10.1371/journal.pone.0324481. [10] ZhangY, ChenQ, WangR, et al. Global trends in thermal burn burden, 1990-2021: a comprehensive analysis for the global burden of disease study 2021[J]. Front Public Health, 2025,13:1631138.DOI: 10.3389/fpubh.2025.1631138. [11] 李丽清,周绪,赵玉兰,等.我国东中西部地区基层医疗资源配置与经济发展耦合协调关系研究[J].中国全科医学,2021,24(22):2777-2784.DOI: 10.12114/j.issn.1007-9572.2021.00.234. [12] LiP,ZhangQ,LiD.Epidemiology and prognosis of burn injuries in China: a meta-analysis[J].Eur J Med Res,2025,30(1):581.DOI: 10.1186/s40001-025-02741-x. [13] YangJ,TianG,LiuJ,et al.Epidemiology and clinical characteristics of burns in mainland China from 2009 to 2018[J/OL].Burns Trauma,2022,10:tkac039[2025-12-08].https://pubmed.ncbi.nlm.nih.gov/36196302/.DOI: 10.1093/burnst/tkac039. [14] ZhangY,SuJ,LiuY,et al.Epidemiological and clinical characteristics of burns in adults: a 6-year retrospective study in a major burn center in Suzhou, China[J].Front Public Health,2024,12:1413986.DOI: 10.3389/fpubh.2024.1413986. [15] 王阳, 赵宇辉, 刘军, 等. 基于GBD 2021数据库的中国中老年人群烧伤疾病负担特征分析与趋势预测[J]. 中华烧伤与创面修复杂志, 2026,42(4):373-382.DOI: 10.3760/cma.j.cn501225-20250710-00296. [16] StevensGA, AlkemaL, BlackRE, et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement[J]. Lancet, 2016,388(10062):e19-e23.DOI: 10.1016/S0140-6736(16)30388-9. [17] GBD 2021 Diseases and Injuries Collaborators.Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021[J].Lancet,2024,403(10440):2133-2161.DOI: 10.1016/S0140-6736(24)00757-8. [18] LiuH, YinP, QiJ, et al. Burden of non-communicable diseases in China and its provinces, 1990-2021: results from the Global Burden of Disease Study 2021[J]. Chin Med J (Engl), 2024,137(19):2325-2333.DOI: 10.1097/CM9.0000000000003270. [19] GBD 2021 Causes of Death Collaborators.Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021[J].Lancet,2024,403(10440):2100-2132.DOI: 10.1016/S0140-6736(24)00367-2. [20] MehtaK,AregaH,SmithNL,et al.Gender-based disparities in burn injuries, care and outcomes: a World Health Organization (WHO) Global Burn Registry cohort study[J].Am J Surg,2022,223(1):157-163.DOI: 10.1016/j.amjsurg.2021.07.041. [21] Bagheri ToolaroudP, AttarchiM, Afshari HaghdoustR, et al. Epidemiology of work-related burn injuries: a ten-year retrospective study of 429 patients at a referral burn centre in the north of Iran[J]. Int Wound J, 2023,20(9):3599-3605.DOI: 10.1111/iwj.14238. [22] ChenZ, ZhangM, XieS, et al. Global burden of thermal burns, 1990-2017: unbalanced distributions and temporal trends assessed from the Global Burden of Disease Study 2017[J]. Burns, 2022,48(4):915-925.DOI: 10.1016/j.burns.2021.08.002. [23] ChenK, LiuJ, WangX, et al. Epidemiological characteristics of paediatric burn patients in China from 2016 to 2019: a retrospective study[J]. BMJ Paediatr Open, 2023,7(1):e001796.DOI: 10.1136/bmjpo-2022-001796. [24] LiuT, QuY, ChaiJ, et al. Epidemiology and first aid measures in pediatric burn patients in northern China during 2016-2020: a single-center retrospective study[J]. Health Sci Rep, 2024,7(7):e2218.DOI: 10.1002/hsr2.2218. [25] WuH,XiM,XieW.Epidemiological and clinical characteristics of older adults with burns: a 15-year retrospective analysis of 2554 cases in Wuhan Institute of Burns[J].BMC Geriatr,2023,23(1):162.DOI: 10.1186/s12877-023-03883-5. [26] FanS, QiuY, GuY, et al. Exploring the experiences of older adults with burn injuries in China: a qualitative study[J]. Geriatr Nurs, 2025,64:103397.DOI: 10.1016/j.gerinurse.2025.103397. [27] CordsCI,van BaarME,PijpeA,et al.Short-term and long-term increased mortality in elderly patients with burn injury: a national longitudinal cohort study[J].BMC Geriatr,2023,23(1):30.DOI: 10.1186/s12877-022-03669-1. [28] ZhangH, WangW, BanQ. Seasonal forest fire risk and key drivers in Yunnan Province: a machine learning approach[J]. NPJ Nat Hazards, 2025,2:59.DOI: 10.1038/s44304-025-00112-4. [29] 王瑶,罗雪纯,向楠,等.贵州省2011~2023年山火时空分布及气象条件影响分析[J].气候变化研究快报,2024,13(5):1138-1146.DOI: 10.12677/ccrl.2024.135129. [30] 王若宇,陈伟,许勋,等.烧伤患儿329例流行病学调查及全身炎症反应综合征危险因素分析[J].昆明医科大学学报,2024,45(5):123-129.DOI: 10.12259/j.issn.2095-610X.S20240519. [31] 王璐瑶,尹勤,朱凯.中国流动人口健康教育现状及其影响因素分析[J].中国公共卫生,2021,37(2):193-197.DOI: 10.11847/zgggws1125696. [32] 郑佳慧,王书平,邹云锋,等.中国重症床位资源配置现状及预测[J].中国卫生资源,2023,26(3):257-263.DOI: 10.13688/j.cnki.chr.2023.220998. [33] 朱碧帆,侯晓慧,覃湫珺,等.2019—2023年上海市外来住院患者情况分析[J].健康发展与政策研究,2025,28(6):613-621.DOI: 10.12458/HDPR.202406061. [34] 郭绍彬, 唐世杰, 张万聪. 1990-2019年中国烧伤发病率及死亡率趋势的年龄-时期-队列模型分析[J]. 中国美容医学, 2023,32(7):9-13.DOI: 10.15909/j.cnki.cn61-1347/r.005773. [35] 国务院. 国务院关于印发中国妇女发展纲要和中国儿童发展纲要的通知:国发〔2021〕16号[A/OL]. (2021-09-08)[2026-05-12]. https://www.gov.cn/gongbao/content/2021/content_5643262.htm. https://www.gov.cn/gongbao/content/2021/content_5643262.htm [36] 国家统计局 2024年《中国儿童发展纲要(2021—2030年)》统计监测报告 2025-12-30 2026-05-12 https://www.stats.gov.cn/sj/zxfb/202512/t20251230_1962182.html 国家统计局. 2024年《中国儿童发展纲要(2021—2030年)》统计监测报告[EB/OL]. (2025-12-30)[2026-05-12]. https://www.stats.gov.cn/sj/zxfb/202512/t20251230_1962182.html.
[37] WangY, WangR, JiangM, et al. Provincial inequality of China's progress towards universal health coverage: an empirical analysis in 2016-21[J]. J Glob Health, 2024,14:04122.DOI: 10.7189/jogh.14.04122. [38] SpronkI,van BaarME,VerheijRA,et al.The burden of disease of fatal and non-fatal burn injuries for the full spectrum of care in the Netherlands[J].Arch Public Health,2023,81(1):3.DOI: 10.1186/s13690-022-01020-z. -

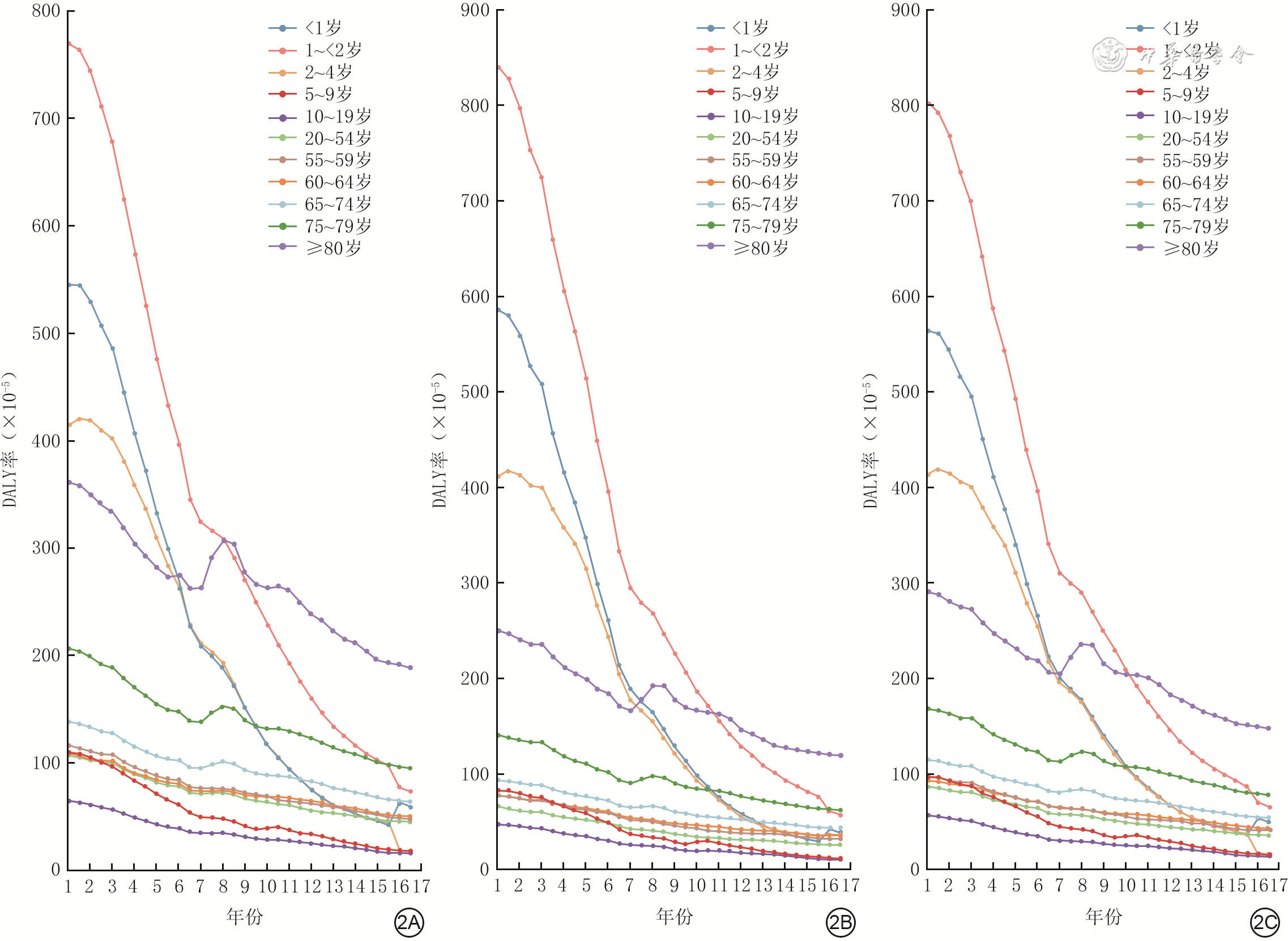
图 2 1990—2021年中国不同年龄段人群烧伤伤残调整生命年率变化趋势。2A.男性;2B.女性;2C.总人群
注:DALY为伤残调整生命年;横坐标中1、2、3、4、5、6、7、8、9、10、11、12、13、14、15、16、17依次为1990、1992、1994、1996、1998、2000、2002、2004、2006、2008、2010、2012、2014、2016、2018、2020、2022年
Table 1. 2021年中国不同省级行政区人群的烧伤疾病负担
省级行政区 年龄标化YLD率 年龄标化YLL率 年龄标化DALY率 数值(95%UI)(×10-⁵) 排序 数值(95%UI)(×10-⁵) 排序 数值(95%UI)(×10-⁵) 排序 云南省 18.4(12.1~27.2) 9 27.0(21.2~38.1) 1 45.4(37.2~58.7) 1 贵州省 20.2(12.9~30.1) 4 23.6(18.4~31.9) 5 43.8(34.3~55.4) 2 上海市 33.1(19.0~52.4) 1 10.2(7.9~13.4) 31 43.3(29.6~62.2) 3 江西省 19.7(11.6~30.5) 6 22.0(16.5~27.1) 8 41.7(32.7~53.6) 4 北京市 30.7(17.8~48.2) 2 11.0(7.6~14.4) 30 41.7(29.1~59.3) 5 浙江省 20.0(11.5~31.4) 5 20.3(10.5~26.2) 12 40.3(27.8~52.5) 6 陕西省 12.6(7.4~19.3) 15 24.4(16.6~30.9) 3 37.0(28.1~46.5) 7 甘肃省 19.7(12.2~29.7) 7 17.2(13.6~26.2) 23 36.9(28.5~48.8) 8 山东省 17.2(9.7~27.2) 10 19.6(12.4~25.3) 15 36.8(27.5~47.9) 9 四川省 15.0(9.1~22.8) 12 21.6(17.2~28.4) 10 36.6(28.6~46.0) 10 湖南省 10.8(6.4~16.7) 20 25.2(15.9~32.3) 2 36.0(26.4~44.2) 11 江苏省 19.6(11.2~31.0) 8 15.3(9.3~19.5) 26 34.9(25.9~47.1) 12 海南省 20.6(12.6~31.3) 3 14.3(9.9~27.6) 28 34.8(25.4~50.5) 13 山西省 14.8(8.7~23.1) 13 19.2(14.7~24.9) 16 34.0(26.7~43.7) 14 天津市 14.5(8.2~22.5) 14 19.1(11.6~24.5) 18 33.6(24.7~43.8) 15 广西壮族自治区 9.8(6.0~14.7) 23 23.4(17.3~29.2) 6 33.2(26.0~40.8) 16 新疆维吾尔自治区 8.8(5.8~12.5) 29 24.2(17.5~33.6) 4 33.0(25.5~43.4) 17 湖北省 8.6(4.9~13.4) 30 22.6(14.8~28.2) 7 31.2(23.2~38.4) 18 河北省 9.3(5.6~14.1) 25 21.8(16.2~28.2) 9 31.1(24.5~39.6) 19 内蒙古自治区 12.4(7.2~19.3) 17 18.2(14.2~23.2) 21 30.6(24.2~39.4) 20 宁夏回族自治区 10.2(6.0~15.6) 22 19.8(15.3~25.6) 14 29.9(23.6~37.7) 21 重庆市 11.2(6.4~17.6) 18 18.7(14.7~24.1) 19 29.9(23.0~38.0) 22 广东省 16.4(9.4~25.6) 11 12.6(9.8~16.5) 29 29.0(21.2~39.2) 23 河南省 9.1(5.2~14.2) 28 18.5(13.4~23.2) 20 27.5(21.6~34.4) 24 辽宁省 6.7(3.8~10.5) 32 20.2(13.7~26.0) 13 27.0(20.0~33.6) 25 青海省 7.7(5.0~10.9) 31 19.2(13.9~36.3) 17 26.9(20.7~44.0) 26 福建省 10.2(5.8~15.8) 21 16.6(12.9~20.7) 25 26.8(21.3~34.4) 27 吉林省 9.2(5.3~14.5) 26 17.4(14.1~23.1) 22 26.6(21.5~34.2) 28 安徽省 6.0(3.4~9.3) 33 20.4(14.8~25.7) 11 26.3(20.5~32.3) 29 黑龙江省 9.1(5.3~14.3) 27 16.8(12.9~24.9) 24 25.9(20.1~35.3) 30 西藏自治区 9.6(6.7~13.1) 24 15.3(8.4~45.1) 27 24.9(16.4~55.3) 31 澳门特别行政区 11.1(6.4~17.3) 19 9.0(5.3~12.1) 32 20.1(14.2~26.7) 32 香港特别行政区 12.5(7.2~19.6) 16 4.6(3.2~7.8) 33 17.1(11.4~25.0) 33 注:YLD为失能所致生命年损失,YLL为早死所致生命年损失,DALY为伤残调整生命年  下载: 导出CSV
下载: 导出CSV
-

 下载:
下载:


图(3) / 表(1)
计量
- 文章访问数: 446
- HTML全文浏览量: 246
- PDF下载量: 17
- 被引次数: 0
