




Construction and validation of a predictive model for the risk of ARDS in severely burned patients
-
摘要:
目的 构建并验证用于预测严重烧伤患者发生急性呼吸窘迫综合征(ARDS)风险的列线图模型。 方法 该研究为回顾性队列研究。2015年1月—2025年8月,解放军总医院第四医学中心收治372例符合入选标准的严重烧伤患者,其中男279例、女93例,年龄18~78岁。按照伤后7 d内是否发生ARDS,将患者分为ARDS组及非ARDS组。采用分层随机抽样法,按照7∶3的比例将患者划分为训练集和验证集。训练集中,ARDS组患者35例、非ARDS组患者227例;验证集中,ARDS组患者14例、非ARDS组患者96例。收集患者一般临床资料,包括烧伤总面积、改良Baux指数、烧伤指数、Ⅱ度烧伤面积、Ⅲ度烧伤面积、吸入性损伤程度、入院时是否行机械通气或高流量氧疗、气管切开天数、住院天数、病危病重天数及病死率等;以及入院24 h内与伤后发生ARDS相关的资料,包括白细胞计数、中性粒细胞计数、凝血酶时间及血红蛋白、肌酐、氯、降钙素原、白蛋白、纤维蛋白原(FIB)水平等。筛选训练集患者组间比较差异有统计学意义的变量,并基于最小绝对值压缩和选择算法(LASSO)回归结合权重调整策略进一步筛选特征性变量。进行多因素logistic回归分析确定患者发生ARDS风险的独立预测因子,并据此构建列线图模型。在训练集和验证集中对该模型效能进行验证。 结果 训练集一般临床资料中,ARDS组患者的烧伤总面积、Ⅲ度烧伤面积均显著大于非ARDS组(P<0.05),改良Baux指数、烧伤指数、入院时行机械通气或高流量氧疗比例及病死率均显著高于非ARDS组(P<0.05),吸入性损伤程度显著重于非ARDS组(P<0.05),气管切开天数、住院天数及病危病重天数均显著多于非ARDS组(P<0.05),Ⅱ度烧伤面积显著小于非ARDS组(P<0.05);与伤后发生ARDS相关的资料中,ARDS组患者入院24 h内的白细胞计数、中性粒细胞计数及血红蛋白、肌酐、氯、降钙素原水平均显著高于非ARDS组(P<0.05),凝血酶时间显著长于非ARDS组(P<0.05),而白蛋白、FIB水平均显著低于非ARDS组(P<0.05)。LASSO回归分析显示,改良Baux指数、中性粒细胞计数、白蛋白及FIB水平为训练集中262例严重烧伤患者发生ARDS的特征性变量。多因素logistic回归分析显示,改良Baux指数、中性粒细胞计数、白蛋白及FIB水平为训练集中262例严重烧伤患者发生ARDS的独立预测因子(OR分别为1.058、1.147、0.752、0.615,95%CI分别为1.045~1.072、1.092~1.206、0.694~0.814、0.500~0.757,P值均<0.05)。基于前述4个独立预测因子构建了训练集中262例严重烧伤患者发生ARDS风险的列线图模型。受试者操作特征曲线分析显示,该模型在训练集的曲线下面积(AUC)为0.960(95%CI为0.934~0.986),在验证集的AUC为0.914(95%CI为0.837~0.991)。校准曲线显示,该模型预测的ARDS发生风险与实际观察值高度一致。临床决策曲线分析显示,在阈值概率为17%~78%的范围内,应用该模型进行临床决策所能获得的临床净收益均显著高于对所有患者均干预或对所有患者均不干预的策略。 结论 构建的包含改良Baux指数、中性粒细胞计数、白蛋白及FIB水平的列线图模型,对严重烧伤患者发生ARDS风险具有良好的预测效能,具备潜在临床辅助决策价值。 -
关键词:
- 烧伤 /
- 呼吸窘迫综合征,成人 /
- 回顾性研究 /
- 危险因素 /
- Logistic模型 /
- 列线图
Abstract:Objective To construct and validate a nomogram model for predicting the risk of acute respiratory distress syndrome (ARDS) in severely burned patients. Methods This study was a retrospective cohort study. From January 2015 to August 2025, 372 severely burned patients who met the inclusion criteria were admitted to the Fourth Medical Center of Chinese PLA General Hospital, including 279 males and 93 females, aged 18 to 78 years. According to whether ARDS occurred within 7 days post-injury, patients were divided into ARDS group and non-ARDS group. Stratified random sampling was used to allocate patients into training set and validation set in a ratio of 7∶3. In training set, there were 35 patients in ARDS group and 227 patients in non-ARDS group; in validation set, there were 14 patients in ARDS group and 96 patients in non-ARDS group. General clinical data of the patients were collected, including total burn area, modified Baux score, burn index, partial-thickness burn area, full-thickness burn area, severity of inhalation injury, whether mechanical ventilation or high-flow oxygen therapy performed upon admission, number of days after tracheostomy, length of hospital stay, duration in critical illness, and mortality rate, as well as data related to post-burn ARDS development within 24 hours of admission, including white blood cell count, neutrophil count, thrombin time, and levels of hemoglobin, creatinine, chloride, procalcitonin, albumin, and fibrinogen (FIB). Variables with statistically significant differences between two groups in training set were screened, and characteristic variables were further selected using least absolute shrinkage and selection operator (LASSO) regression combined with a weight adjustment strategy. Multivariate logistic regression analysis was performed to identify independent predictors, based on which a nomogram model was constructed. The performance of the model was validated in both training set and validation set. Results In the general clinical data of training set, patients in ARDS group had significantly larger total burn area and full-thickness burn area (P<0.05), significantly higher modified Baux score, burn index, proportion of patients receiving mechanical ventilation or high-flow oxygen therapy upon admission, and mortality rate (P<0.05), significantly more severe degree of inhalation injury (P<0.05), significantly greater number of days after tracheostomy, length of hospital stay, and duration in critical illness (P<0.05), and significantly smaller partial-thickness burn area (P<0.05) than those in non-ARDS group. With the data related to post-burn ARDS development, patients in ARDS group had significantly higher white blood cell count, neutrophil count, and levels of hemoglobin, creatinine, chloride, and procalcitonin (P<0.05), significantly longer thrombin time (P<0.05), and significantly lower levels of albumin and FIB (P<0.05) than those in non-ARDS group within 24 hours of admission. LASSO regression analysis showed that modified Baux score, neutrophil count, albumin level, and FIB level were the characteristic variables for the development of ARDS in 262 severely burned patients in training set. Multivariate logistic regression analysis revealed that modified Baux score, neutrophil count, albumin level, and FIB level were independent predictors of ARDS in 262 severely burned patients in training set (with ORs of 1.058, 1.147, 0.752, and 0.615, respectively, 95%CIs of 1.045-1.072, 1.092-1.206, 0.694-0.814, and 0.500-0.757, respectively, P values all <0.05). A nomogram model for predicting the risk of ARDS in 262 severely burned patients in training set was constructed based on the above four independent predictors. Receiver operating characteristic curve analysis showed that the model had an area under the curve (AUC) of 0.960 (with 95%CI of 0.934-0.986) in training set and an AUC of 0.914 (with 95%CI of 0.837-0.991) in validation set. The calibration curve showed that the risk of ARDS predicted by the model was in high agreement with the actual observed values. Clinical decision curve analysis showed that within the threshold probability range of 17% to 78%, the clinical net benefit obtained by applying this model for clinical decision-making was significantly higher than that of the strategies of intervening in all patients or intervening in none. Conclusions The constructed nomogram model incorporating the modified Baux score, neutrophil count, albumin level, and FIB level demonstrates good predictive performance for the risk of ARDS in severely burned patients and holds potential value for clinical decision-making. -
Key words:
- Burns /
- Respiratory distress syndrome, adult /
- Retrospective studies /
- Risk factors /
- Logistic models /
- Nomograms
-
参考文献
(40) [1] BosL, WareLB. Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes[J]. Lancet, 2022,400(10358):1145-1156. DOI: 10.1016/S0140-6736(22)01485-4. [2] YıldırımF, Karamanİ, KayaA. Current situation in ARDS in the light of recent studies: Classification, epidemiology and pharmacotherapeutics[J]. Tuberk Toraks, 2021,69(4):535-546. DOI: 10.5578/tt.20219611. [3] BittnerE, SheridanR. Acute respiratory distress syndrome, mechanical ventilation, and inhalation injury in burn patients[J]. Surg Clin North Am, 2023,103(3):439-451. DOI: 10.1016/j.suc.2023.01.006. [4] 刘有芳, 詹庆元, 黄絮, 等. 急性呼吸窘迫综合征患者保护性肺通气策略依从性现况调查[J].中华结核和呼吸杂志,2024,47(5):419-429. DOI: 10.3760/cma.j.cn112147-20230808-00054. [5] 杨姗, 杨婧, 康焰. 经鼻高流量氧疗和无创通气在急性呼吸窘迫综合征治疗中的价值[J].中华医学杂志,2024,104(15):1230-1235. DOI: 10.3760/cma.j.cn112137-20231023-00865. [6] ShaoS, KangH, TongZ. Early neuromuscular blocking agents for adults with acute respiratory distress syndrome: a systematic review, meta-analysis and meta-regression[J]. BMJ Open, 2020,10(11):e037737. DOI: 10.1136/bmjopen-2020-037737. [7] 马娟娟, 陈雪玲, 王蕾. ARDS患者救治中有创呼吸机辅助呼吸的临床干预及疗效分析[J/OL].中华肺部疾病杂志(电子版),2022,15(6):876-878[2026-02-04]. https://rs.yiigle.com/cmaid/1558751.DOI: 10.3877/cma.j.issn.1674-6902.2022.06.030. [8] MatthayMA, ArabiY, ArroligaAC, et al. A new global definition of acute respiratory distress syndrome[J]. Am J Respir Crit Care Med, 2024,209(1):37-47. DOI: 10.1164/rccm.202303-0558WS. [9] NielsonCB, DuethmanNC, HowardJM, et al. Burns: pathophysiology of systemic complications and current management[J]. J Burn Care Res, 2017,38(1):e469-e481. DOI: 10.1097/BCR.0000000000000355. [10] WangB, ChenruW, JiangY, et al. Incidence and mortality of acute respiratory distress syndrome in patients with burns: a systematic review and meta-analysis[J]. Front Med (Lausanne), 2021,8:709642. DOI: 10.3389/fmed.2021.709642. [11] BelenkiySM, BuelAR, CannonJW, et al. Acute respiratory distress syndrome in wartime military burns: application of the Berlin criteria[J]. J Trauma Acute Care Surg, 2014,76(3):821-827. DOI: 10.1097/TA.0b013e3182aa2d21. [12] 朱峰, 郭光华. 烧伤相关肺损伤的呼吸治疗任重道远[J].中华烧伤与创面修复杂志,2024,40(11):1016-1023. DOI: 10.3760/cma.j.cn501225-20240802-00291. [13] SilvaL, GarciaL, OliveiraB, et al. Acute respiratory distress syndrome in burn patients: incidence and risk factor analysis[J]. Ann Burns Fire Disasters, 2016,29(3):178-182. [14] WeiS, ZhangH, LiH, et al. Establishment and validation of predictive model of ARDS in critically ill patients[J]. J Transl Med, 2025,23(1):64. DOI: 10.1186/s12967-024-06054-1. [15] 邓兆凯, 刘晟辰, 黎毅敏, 等. 急性呼吸窘迫综合征并发急性肾损伤风险预测研究:进展与挑战[J].中华医学杂志,2025,105(33):2820-2826. DOI: 10.3760/cma.j.cn112137-20250424-01024. [16] 王琦, 马宏炜, 刘皓, 等. 基于LASSO-logistic回归模型构建脓毒症相关性脑病的风险预测模型[J].解放军医学杂志,2026,51(1):38-48. DOI: 10.11855/j.issn.0577-7402.1570.2025.1124. [17] 白鹭, 何涛, 吴建祥, 等. 血清降钙素原、C反应蛋白、高迁移率族蛋白B1及白细胞介素-6水平对创伤性肺损伤患者预后的预测价值[J].中华实验外科杂志,2024,41(11):2613-2616. DOI: 10.3760/cma.j.cn421213-20240427-01081. [18] 余淼, 孟岩, 朱科明, 等. 中性粒细胞胞外陷阱在急性呼吸窘迫综合征中的研究进展[J].国际麻醉学与复苏杂志,2024,45(10):1105-1110. DOI: 10.3760/cma.j.cn321761-20230815-01142. [19] 尚游, 张红玲, 刘玲, 等. 急性呼吸窘迫综合征全球新定义中S/F的中文命名[J].中华医学杂志,2025,105(9):647-649. DOI: 10.3760/cma.j.cn112137-20241128-02671. [20] TranTK, TranMC, JosephA, et al. A systematic review of machine learning models for management, prediction and classification of ARDS[J]. Respir Res, 2024, 25(1):232. DOI: 10.1186/s12931-024-02834-x. [21] JeschkeMG, van BaarME, ChoudhryMA, et al. Burn injury[J]. Nat Rev Dis Primers, 2020,6(1):11. DOI: 10.1038/s41572-020-0145-5. [22] LamNN, HungTD. ARDS among cutaneous burn patients combined with inhalation injury: early onset and bad outcome[J]. Ann Burns Fire Disasters, 2019,32(1):37-42. [23] 沈凯凯, 魏雨晴, 金佳佳, 等. 肺泡巨噬细胞TRIM21表达水平对重症肺炎合并ARDS患者病情严重程度和预后的评估价值[J].解放军医学杂志,2025,50(7):817-823. DOI: 10.11855/j.issn.0577-7402.1625.2025.0226. [24] JonesSW, WilliamsFN, CairnsBA, et al. Inhalation injury: pathophysiology, diagnosis, and treatment[J]. Clin Plast Surg, 2017,44(3):505-511. DOI: 10.1016/j.cps.2017.02.009. [25] WickKD, WareLB, MatthayMA. Acute respiratory distress syndrome[J]. BMJ, 2024,387:e076612. DOI: 10.1136/bmj-2023-076612. [26] 许呢妹, 张爽, 刘志锋. 急性呼吸窘迫综合征的分型及个体化治疗研究进展[J].解放军医学杂志,2023,48(5):615-620. DOI: 10.11855/j.issn.0577-7402.2023.05.0615. [27] 李待兮, 张孝斌, 朱子锐, 等. 急性呼吸窘迫综合征的亚型与精准治疗[J].中华结核和呼吸杂志,2024,47(6):560-566. DOI: 10.3760/cma.j.cn112147-20231126-00341. [28] TanitaMT, CapelettiMM, MoreiraTA, et al. Risk factors for acute respiratory distress syndrome in severe burns: prospective cohort study[J]. Int J Burns Trauma, 2020,10(1):1-14. [29] WeiT, PengS, LiX, et al. Critical evaluation of established risk prediction models for acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis[J]. J Evid Based Med, 2023,16(4):465-476. DOI: 10.1111/jebm.12565. [30] ŻwierełłoW, PiorunK, Skórka-MajewiczM, et al. Burns: classification, pathophysiology, and treatment: a review[J]. Int J Mol Sci, 2023,24(4):3749. DOI: 10.3390/ijms24043749. [31] 刘双庆, 祝筱梅, 姚咏明. 严重烧创伤脓毒症免疫功能障碍的诊疗策略[J].中华创伤杂志,2025,41(5):433-439. DOI: 10.3760/cma.j.cn501098-20250407-00197. [32] BurgessM, ValderaF, VaronD, et al. The immune and regenerative response to burn injury[J]. Cells, 2022,11(19):3073. DOI: 10.3390/cells11193073. [33] SierawskaO, MałkowskaP, TaskinC, et al. Innate immune system response to burn damage-focus on cytokine alteration[J]. Int J Mol Sci, 2022,23(2):716. DOI: 10.3390/ijms23020716. [34] YoonJ, KymD, ChoYS, et al. Longitudinal analysis of ARDS variability and biomarker predictive power in burn patients[J]. Sci Rep, 2024,14(1):26376. DOI: 10.1038/s41598-024-77188-x. [35] MeyerNJ, GattinoniL, CalfeeCS. Acute respiratory distress syndrome[J]. Lancet, 2021,398(10300):622-637. DOI: 10.1016/S0140-6736(21)00439-6. [36] ToyP, LooneyMR, PopovskyM, et al. Transfusion-related acute lung injury: 36 years of progress (1985-2021)[J]. Ann Am Thorac Soc, 2022,19(5):705-712. DOI: 10.1513/AnnalsATS.202108-963CME. [37] 罗延年, 席振创, 王锐, 等. 乳酸/白蛋白比值联合NLR构建的列线图对急性呼吸窘迫综合征患者早期预后的预测价值[J].解放军医学杂志,2023,48(10):1194-1200. DOI: 10.11855/j.issn.0577-7402.2364.2023.0718. [38] 袁雪燕, 刘玲, 邱海波. 2023急性呼吸窘迫综合征全球新标准:进步与局限[J].中华医学杂志,2024,104(15):1216-1220. DOI: 10.3760/cma.j.cn112137-20231016-00770. [39] ARDSDefinition Task Force, RanieriVM, RubenfeldGD, et al. Acute respiratory distress syndrome: the Berlin Definition[J]. JAMA, 2012,307(23):2526-2533. DOI: 10.1001/jama.2012.5669. [40] 冯云爱, 李海潮. 急性呼吸窘迫综合征的定义演变、争议及本质探讨[J].中华结核和呼吸杂志,2024,47(1):87-90. DOI: 10.3760/cma.j.cn112147-20230713-00005. -

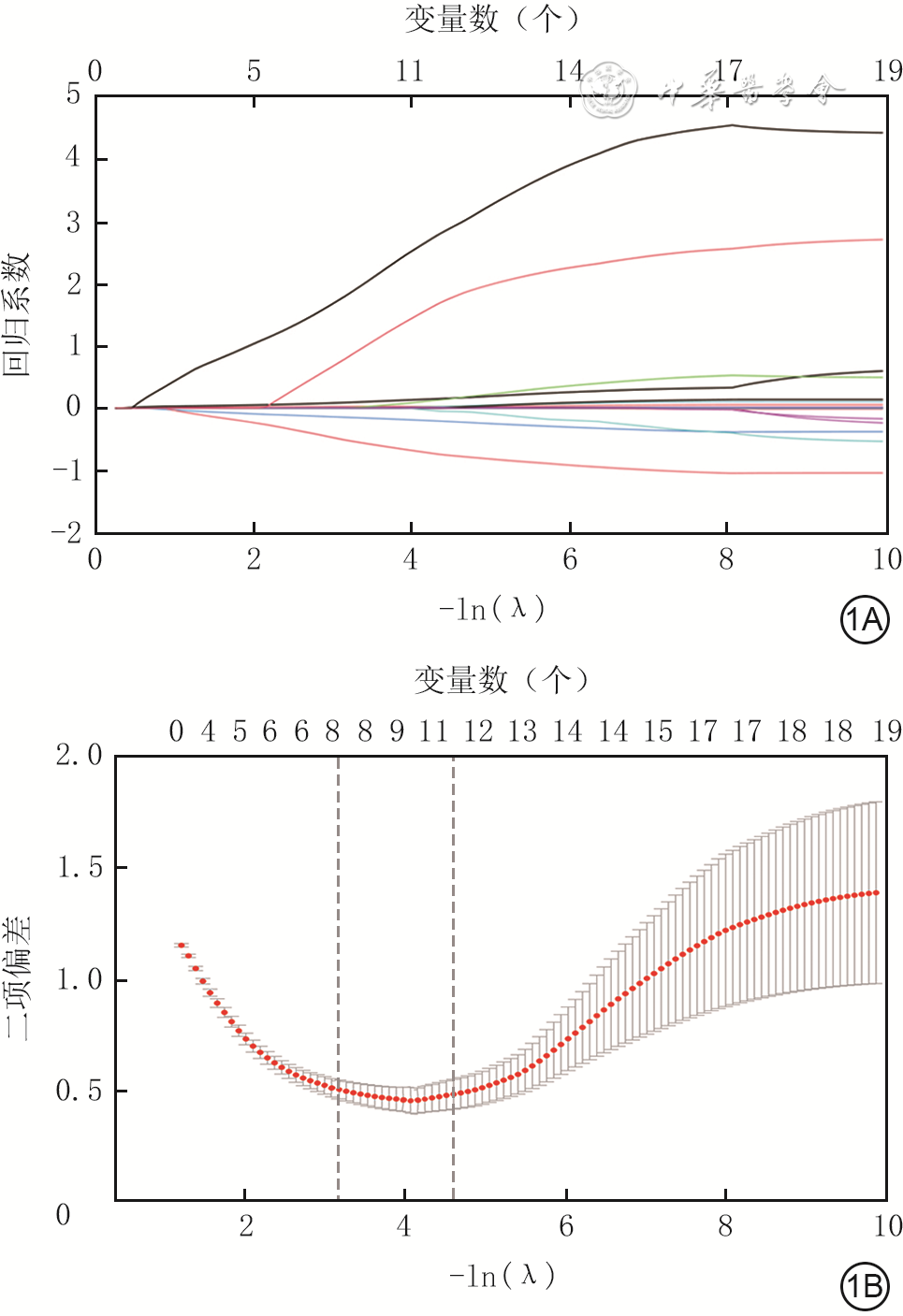
图 1 训练集中262例严重烧伤患者各变量的最小绝对值压缩和选择算法的系数路径图及交叉验证图。1A.路径图;1B.交叉验证图
注:图1A中λ为调优参数,随着正则化参数λ增大,各变量回归系数被压缩直至归零并最终被剔除;不同颜色线条代表不同变量的压缩轨迹,在变量数收缩到4时,从上至下的曲线依次代表改良Baux指数、中性粒细胞计数、纤维蛋白原及白蛋白水平;图1B中实线表示交叉验证误差(二项偏差)随正则化参数λ(对数尺度)的变化,用于平衡模型拟合优度与复杂度,阴影区域表示交叉验证误差的一个标准差范围;右侧虚线对应最小交叉验证误差λ_min,左侧虚线对应最小误差在一个标准差范围内的最大λ值λ_1se;本研究采用λ_1se以获得更简约的模型

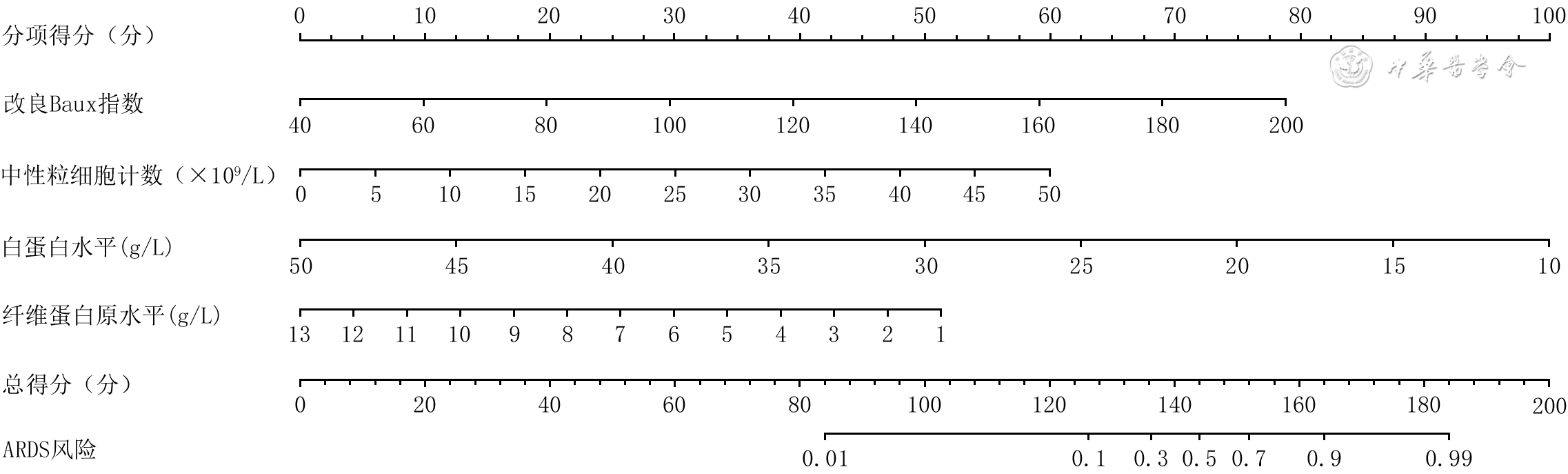
图 2 训练集中262例严重烧伤患者发生ARDS风险的列线图模型
注:ARDS为急性呼吸窘迫综合征;使用该列线图模型时,首先在相应变量的刻度轴上确定每例患者各指标取值所对应的分值,然后将各项分值相加得到总得分,最后在总得分轴上找到对应的ARDS发生风险

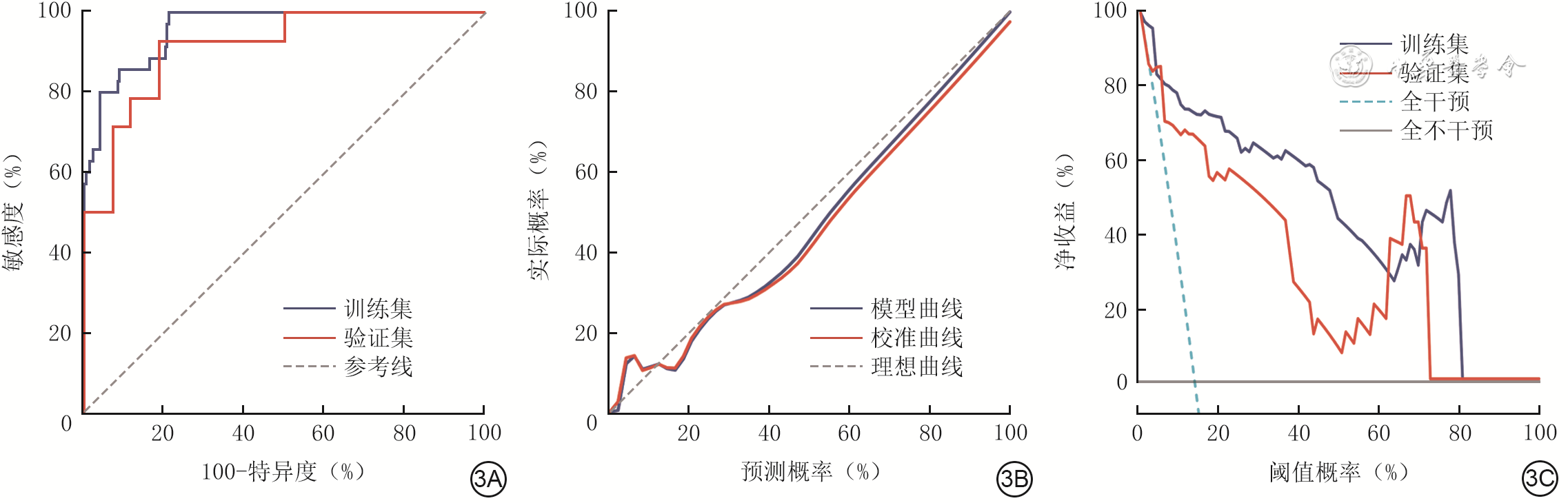
图 3 训练集中262例严重烧伤患者发生急性呼吸窘迫综合征风险的列线图模型验证与评估。3A.训练集与验证集的受试者操作特征曲线;3B.训练集的校准曲线;3C.训练集与验证集的临床决策曲线
Table 1. 训练集中2组严重烧伤患者基线资料比较
组别 例数 性别(例) 年龄[岁, M(Q1 , Q3)]身高[m, M(Q1 , Q3)]体重[kg, M(Q1 , Q3)]身体质量指数[kg/m2,M(Q1 , Q3)]男 女 ARDS组 35 6 29 44.0(34.0,54.0) 1.7(1.7,1.7) 75.0(68.0,80.0) 26.0(23.0,28.4) 非ARDS组 227 52 175 41.0(31.0,51.0) 1.7(1.7,1.8) 72.0(61.0,80.0) 24.7(22.2,27.5) 统计量值 χ2=0.298 Z=-1.317 Z=0.079 Z=-0.678 Z=-1.059 P值 0.585 0.188 0.938 0.498 0.290 注:ARDS为急性呼吸窘迫综合征  下载: 导出CSV
下载: 导出CSV
Table 2. 训练集中2组严重烧伤患者一般临床资料比较
组别 例数 致伤环境(例) 吸入性损伤程度(例) 入院时行机械通气或高流量氧疗(例) 死亡(例) Ⅱ度烧伤面积[%TBSA,M(Q1,Q3)] Ⅲ度烧伤面积[%TBSA,M(Q1,Q3)] 密闭 开放 无 轻度 中度 重度 是 否 是 否 ARDS组 35 18 17 2 6 9 18 12 23 11 24 10.0(5.0,30.0) 45.0(22.0,85.0) 非ARDS组 227 122 105 104 86 31 6 4 223 4 223 23.0(15.0,30.0) 20.0(10.0,40.0) 统计量值 χ2=0.005 — — — Z=3.623 Z=-4.427 P值 0.941 <0.001 <0.001 <0.001 0.001 <0.001 注:ARDS为急性呼吸窘迫综合征,TBSA为体表总面积;“—”表示无此统计量值
下载: 导出CSV
Table 3. 训练集中2组严重烧伤患者血常规、凝血指标、血生化指标比较[M(Q1,Q3)]
组别 例数 血常规 凝血指标 白细胞计数(×10⁹/L) 淋巴细胞计数(×10⁹/L) 中性粒细胞计数(×10⁹/L) 血红蛋白水平(g/L) INR 纤维蛋白原水平(g/L) 凝血酶时间(s) ARDS组 35 26.6(15.8,33.6) 1.0(0.7,1.7) 22.3(13.4,30.3) 170.0(139.0,190.0) 1.1(1.0,1.4) 2.9(2.3,3.6) 14.6(13.6,15.7) 非ARDS组 227 11.2(8.4,16.0) 1.1(0.8,1.4) 9.2(6.8,13.4) 129.0(112.0,153.0) 1.1(1.0,1.2) 4.5(3.3,6.2) 13.0(12.4,13.9) Z值 -6.154 -0.866 -6.277 -4.302 -1.786 5.291 -5.272 P值 <0.001 0.387 <0.001 <0.001 0.074 <0.001 <0.001 注:ARDS为急性呼吸窘迫综合征,INR为国际标准化比值,ALT为丙氨酸氨基转移酶,NT-proBNP为N末端B型利钠肽前体;血常规、凝血指标和血生化指标均为入院24 h内的首次检验结果或记录值
下载: 导出CSV
Table 4. 2组严重烧伤患者中训练集与验证集患者的改良Baux指数、中性粒细胞计数、白蛋白与纤维蛋白原水平比较[M(Q1,Q3)]
组别与分类 例数 改良Baux指数 中性粒细胞计数(×10⁹/L) 白蛋白水平(g/L) 纤维蛋白原水平(g/L) ARDS组 训练集 35 146.0(124.0,159.0) 22.3(13.4,30.3) 27.5(24.0,30.8) 2.9(2.3,3.6) 验证集 14 143.0(128.0,157.0) 16.4(11.4,28.0) 27.2(20.6,32.5) 2.9(2.4,4.5) 非ARDS组 训练集 227 101.0(79.0,124.0) 9.2(6.8,13.4) 33.4(30.3,37.1) 4.5(3.3,6.2) 验证集 96 94.5(80.5,119.5) 9.9(6.8,13.6) 35.5(31.3,37.9) 4.4(3.1,6.3) P1值 0.825 0.424 0.938 0.757 P2值 0.630 0.509 0.054 0.342 注:P1值为ARDS组2个子集各指标比较所得,P2值为非ARDS组2个子集各指标比较所得
下载: 导出CSV
-
 姚颐 6月9日.mp4
姚颐 6月9日.mp4

-

 下载:
下载:



计量
- 文章访问数: 363
- HTML全文浏览量: 184
- PDF下载量: 18
- 被引次数: 0
