- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
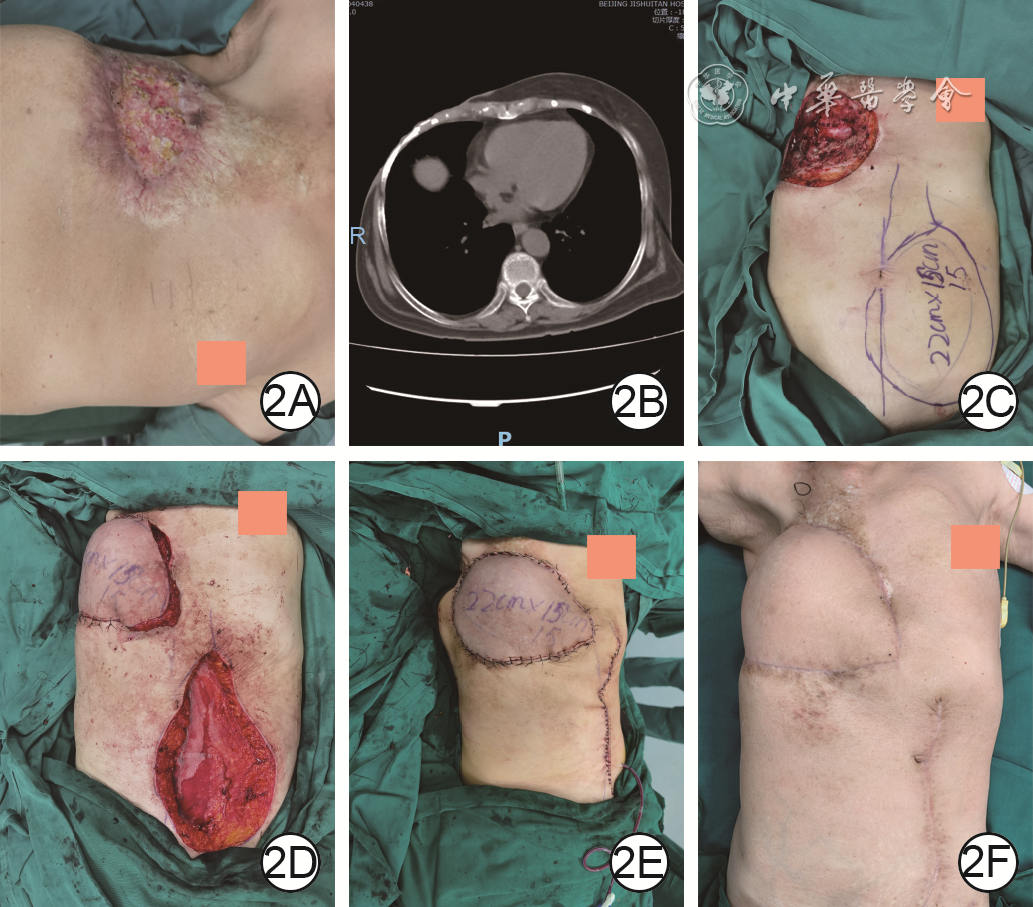
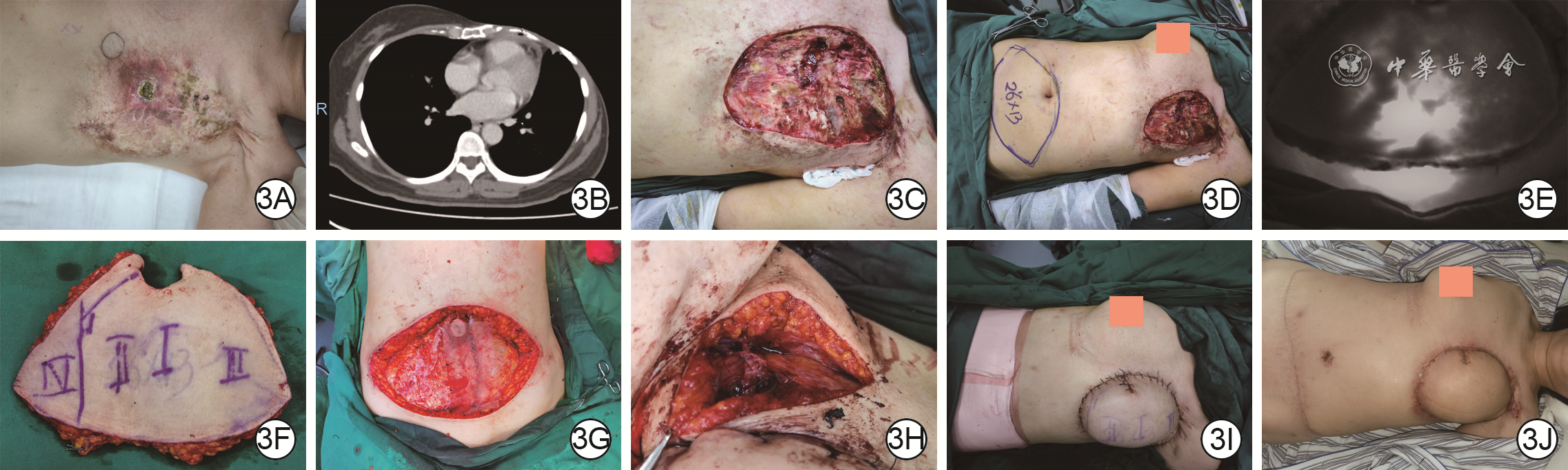
| Citation: | Du WL,Shen YM,Cheng L,et al.Repair strategy of chest radiation ulcer after radical mastectomy for breast cancer and its clinical effect[J].Chin J Burns Wounds,2024,40(6):521-528.DOI: 10.3760/cma.j.cn501225-20240315-00099.

|

| [1] |
程琳,杜伟力,张颖,等.骶尾部慢性放射性溃疡的分期修复策略[J].中华烧伤杂志,2021,37(3):225-231.DOI: 10.3760/cma.j.cn501120-20210104-00003.
|
| [2] |
李罡,张志,李叶扬,等.颈横动脉颈段皮支皮瓣修复颈部放射性溃疡的临床效果[J].中华烧伤杂志,2021,37(12):1116-1121.DOI: 10.3760/cma.j.cn501120-20200807-00371.
|
| [3] |
杨飞,谢卫国,张伟,等.放射性溃疡严重程度分型及临床治疗分析[J].组织工程与重建外科杂志,2022,18(1):62-66.DOI: 10.3969/j.issn.1673-0364.2022.01.015.
|
| [4] |
SpałekM.Chronic radiation-induced dermatitis: challenges and solutions[J].Clin Cosmet Investig Dermatol,2016,9:473-482.DOI: 10.2147/CCID.S94320.
|
| [5] |
BorrelliMR,ShenAH,LeeGK,et al.Radiation-induced skin fibrosis: pathogenesis, current treatment options, and emerging therapeutics[J].Ann Plast Surg,2019,83(4S Suppl 1):S59-64.DOI: 10.1097/SAP.0000000000002098.
|
| [6] |
覃凤均,宁方刚,陈欣,等.26例慢性放射性溃疡的治疗分析[J].中国全科医学,2018,21(z1):232-234.DOI: 10.3969/j.issn.1007-9572.2018.z1.099.
|
| [7] |
MaX,JinZ,LiG,et al.Classification of chronic radiation-induced ulcers in the chest wall after surgery in breast cancers[J].Radiat Oncol,2017,12(1):135.DOI: 10.1186/s13014-017-0876-y.
|
| [8] |
WaghmareCM.Radiation burn--from mechanism to management[J].Burns,2013,39(2):212-219.DOI: 10.1016/j.burns.2012.09.012.
|
| [9] |
李翌,刘会攀,王姊,等.68Ga-枸橼酸PET/CT在炎症及感染疾病中的应用进展[J].国际医学放射学杂志,2020,43(2):219-223.DOI: 10.19300/j.2020.Z17466.
|
| [10] |
郁步惠,苏洪星,孙娜,等.放射性核素显像在肌肉骨骼感染中的研究进展[J].中华核医学与分子影像杂志,2021,41(9):566-573.DOI: 10.3760/cma.j.cn32182-20210713-00233.
|
| [11] |
LiuS,ZhangJ,YinH,et al.The value of 18F-FDG PET/CT in diagnosing and localising deep sternal wound infection to guide surgical debridement[J].Int Wound J,2020,17(4):1019-1027.DOI: 10.1111/iwj.13368.
|
| [12] |
HamadaM,NakaharaT,YazawaM,et al.Radiation-induced osteomyelitis/osteonecrosis of the rib: SPECT/CT imaging for successful surgical management[J].Plast Reconstr Surg Glob Open,2019,7(12):e2536.DOI: 10.1097/GOX.0000000000002536.
|
| [13] |
ZhouB,LongY,LiS,et al.Reconstruction of chronic radiation-induced ulcers in the chest wall using free and pedicle flaps[J].Front Surg,2022,9:1010990.DOI: 10.3389/fsurg.2022.1010990.
|
| [14] |
WangC,ZhangJ,LiuZ.Vacuum-assisted closure therapy combined with bi-pectoral muscle flap for the treatment of deep sternal wound infections[J].Int Wound J,2020,17(2):332-338.DOI: 10.1111/iwj.13277.
|
| [15] |
张龙城,林文彪,韦干观,等.创面准备原则在采用胸大肌皮瓣修复颈部放射性溃疡中的应用[J].中华耳鼻咽喉头颈外科杂志,2014,49(6):509-510.DOI: 10.3760/cma.j.issn.1673-0860.2014.06.015.
|
| [16] |
ChenL,ZhangS,DaJ,et al.A systematic review and meta-analysis of efficacy and safety of negative pressure wound therapy in the treatment of diabetic foot ulcer[J].Ann Palliat Med,2021,10(10):10830-10839.DOI: 10.21037/apm-21-2476.
|
| [17] |
LiX,ZhangF,LiuX,et al.Staged treatment of chest wall radiation-induced ulcer with negative pressure wound therapy and latissimus dorsi myocutaneous flap transplantation[J].J Craniofac Surg,2019,30(5):e450-e453.DOI: 10.1097/SCS.0000000000005514.
|
| [18] |
SteenvoordeP,van EngelandA,OskamJ.Vacuum-assisted closure therapy and oral anticoagulation therapy[J].Plast Reconstr Surg,2004,113(7):2220-2221.DOI: 10.1097/01.prs.0000123603.32963.11.
|
| [19] |
ZhouY,ZhangY.Single- versus 2-stage reconstruction for chronic post-radiation chest wall ulcer: a 10-year retrospective study of chronic radiation-induced ulcers[J].Medicine (Baltimore),2019,98(8):e14567.DOI: 10.1097/MD.0000000000014567.
|
| [20] |
Fernández CanedoI,Padilla EspañaL,Francisco Millán CayetanoJ,et al.Hyperbaric oxygen therapy: an alternative treatment for radiation-induced cutaneous ulcers[J].Australas J Dermatol,2018,59(3):e203-e207.DOI: 10.1111/ajd.12763.
|
| [21] |
RyanJL.Ionizing radiation: the good, the bad, and the ugly[J].J Invest Dermatol,2012,132(3 Pt 2):985-993.DOI: 10.1038/jid.2011.411.
|
| [22] |
张鲜英,刘毅,肖斌,等.慢性放射性溃疡创面的综合治疗[J].中国美容医学,2017,26(12):13-16.
|
| [23] |
宋达疆,李赞,周晓,等.不同形式横行腹直肌肌皮瓣在乳房再造和胸壁溃疡修复中的应用经验教训及对策[J].中国医师杂志,2018,20(4):511-516.DOI: 10.3760/cma.j.issn.1008-1372.2018.04.009.
|
| [24] |
王欣.带蒂腹直肌肌皮瓣修复胸壁深度放射性溃疡[J].组织工程与重建外科杂志,2020,16(4):295-297.DOI: 10.3969/j.issn.1673-0364.2020.04.008.
|
| [25] |
赵奎.背阔肌、腹直肌肌皮瓣修复乳腺癌术后胸壁放射性溃疡的临床疗效对比分析[D].南宁:广西医科大学,2019. |
| [26] |
陈保国,宋慧锋,许明火,等.应用对侧胸廓内动脉穿支皮瓣修复乳腺癌术后高位放射性溃疡[J].中国美容整形外科杂志,2016,27(8):452-454.DOI: 10.3969/j.issn.1673-7040.2016.08.002.
|
| [27] |
LeppardW,PomposelliT,ChangEI,et al.Internal mammary usability as recipient vessels in DIEP breast reconstruction in the setting of previous radiation[J].J Plast Reconstr Aesthet Surg,2018,71(8):1123-1128.DOI: 10.1016/j.bjps.2018.05.041.
|
| [28] |
YamamotoT,KageyamaT,SakaiH,et al.Thoracoacromial artery and vein as main recipient vessels in deep inferior epigastric artery perforator (DIEP) flap transfer for breast reconstruction[J].J Surg Oncol,2021,123(5):1232-1237.DOI: 10.1002/jso.26421.
|
| [29] |
NaraparajuV,MoslehW,AlmnajamM,et al.The utility of radiographic assessment of the internal mammary arteries in chest wall irradiated patients[J].Front Biosci (Landmark Ed),2022,27(1):30.DOI: 10.31083/j.fbl2701030.
|
| [30] |
武雷,丁英状,郝敏如,等.两种下腹部组织瓣修复四肢大面积皮肤软组织缺损后患者的腹部功能与外形[J].中华烧伤与创面修复杂志,2023,39(10):959-967.DOI: 10.3760/cma.j.cn501225-20230428-00145.
|

Figures(4)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: