Abstract:
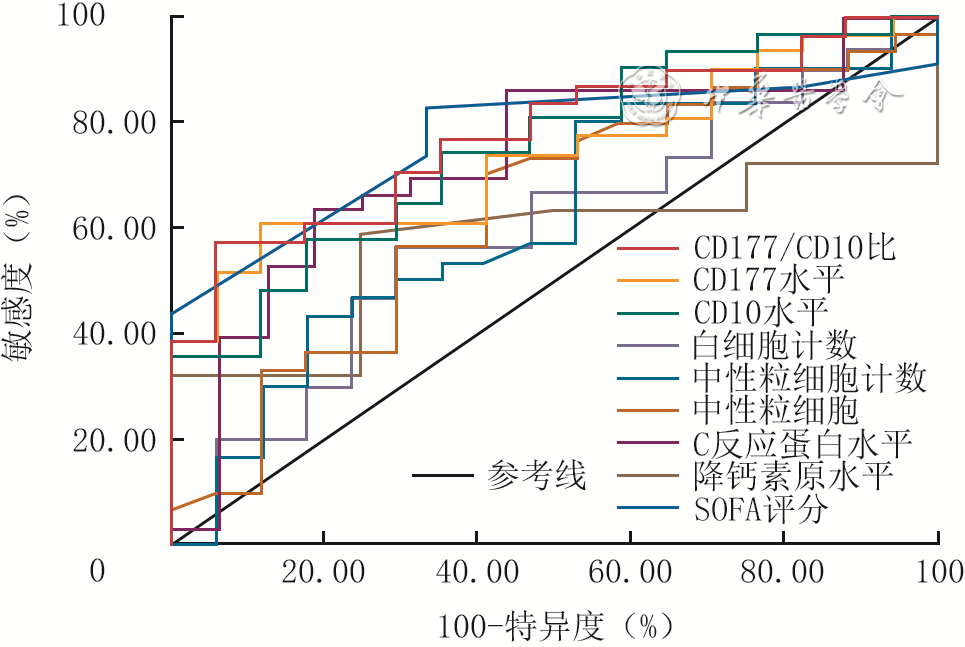
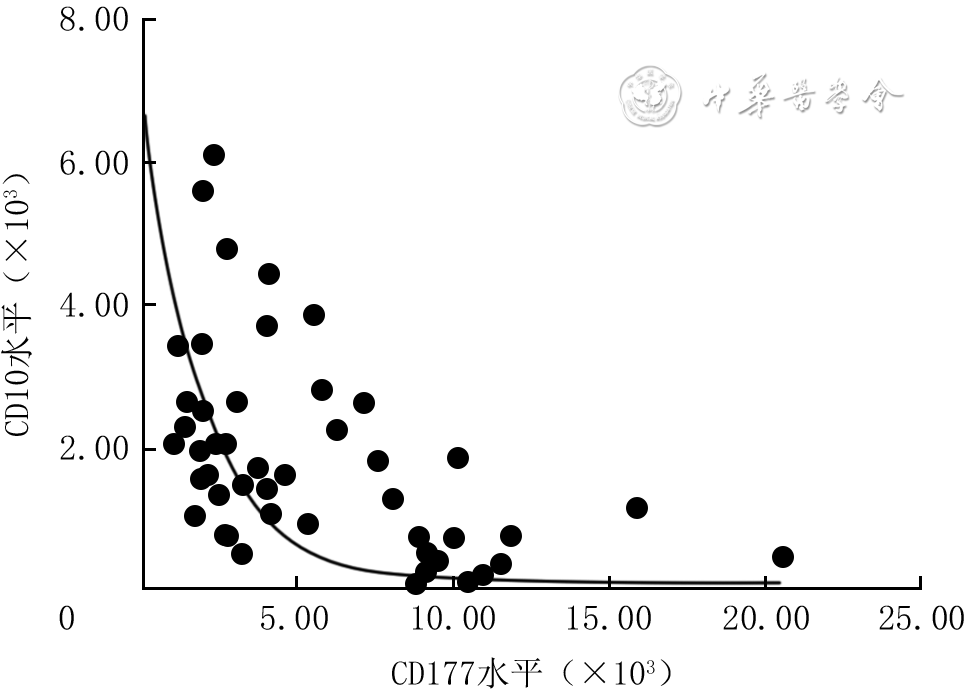
Objective To explore the value of the ratio of CD177 level to CD10 level (hereinafter referred to as CD177/CD10 ratio) in neutrophils in predicting infection risk in burn patients, and to establish its normal reference range. Methods This study was a cross-sectional study. From February 2023 to November 2025, 61 burn patients who met the inclusion criteria were admitted to Affiliated Suzhou Hospital of Nanjing Medical University, including 52 males and 9 females, aged 41.0 (32.0, 55.0) years. Among them, 59 patients underwent inflammatory marker monitoring during the acute stress period on post injury day 1, and 48 patients underwent inflammatory marker monitoring during the high-risk period for infection (hereinafter referred to as high-risk period monitoring) from post injury day 3 to 14. During the same period, 204 healthy volunteers who underwent physical examinations in the physical examination center of the same unit with normal examination results were recruited, including 110 males and 94 females, aged 47.5 (31.0, 67.0) years. Flow cytometry was used to monitor the levels of CD177 and CD10 in the neutrophils from patients on post injury day 1, 3, 5, 7, 10, and 14, as well as from healthy volunteers. According to whether infection occurred, the patients who underwent high-risk period monitoring were divided into infection group (n=31) and non-infection group (n=17). General information such as total burn area at admission, as well as inflammatory markers such as the white blood cell count, neutrophil count, neutrophil, C-reactive protein level, procalcitonin level, CD177 level, CD10 level, and CD177/CD10 ratio, and sequential organ failure assessment (SOFA) scores were compared between the two groups of patients to screen for risk factors affecting the occurrence of infection in patients undergoing high-risk period monitoring. For patients in infection group, the most recent detection data before the confirmed infection was taken for analysis, and for patients in non-infection group, the highest values detected from post injury day 3 to 14 were taken for analysis (the same data selection below). The receiver operating characteristic (ROC) curve was used to evaluate the predictive value of the aforementioned inflammatory markers and SOFA score for the infection risk in patients undergoing high-risk period monitoring. The correlation between CD177 level and CD10 level in patients undergoing high-risk period monitoring was analyzed. The CD177 level, CD10 level, and CD177/CD10 ratio were compared among healthy volunteers, patients during the acute stress period and high-risk period for infection. Based on the data of healthy volunteers, the normal reference range for the CD177/CD10 ratio was established using the non-parametric percentile method. Results There were statistically significant differences between patients in infection group and non-infection group in terms of total burn area, C-reactive protein level, SOFA score, CD177 level, CD10 level, and CD177/CD10 ratio (with Z values of -2.08, -2.58, 0.04, -2.72, -2.86, and -3.20, respectively, P<0.05). The results of univariate logistic regression analysis showed that both total burn area and the lg (CD177/CD10 ratio) were risk factors for infection in patients undergoing high-risk period monitoring (with ORs of 1.03 and 6.91, respectively, 95%CIs of 1.00 to 1.06 and 1.84 to 25.91, respectively, P<0.05). The results of multivariate logistic regression analysis showed that the lg (CD177/CD10 ratio) was an independent risk factor for infection in patients undergoing high-risk period monitoring (OR=5.73, with a 95%CI of 1.11 to 29.60, P<0.05). ROC curve analysis showed that the CD177/CD10 ratio had the largest area under the curve for predicting the infection risk in patients undergoing high-risk period monitoring, which was 0.78 (with a 95%CI of 0.65 to 0.91). Its optimal cut-off value was 3.84, with the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value at the optimal cut-off value being 58.06%, 94.12%, 76.09%, 94.74%, and 55.17%, respectively. In patients undergoing high-risk period monitoring, the CD177 level was significantly negatively correlated with the CD10 level (r=-0.60, P<0.05). Compared with those of healthy volunteers and patients in the acute stress period, the CD10 level of patients in the high-risk period for infection was significantly decreased (with P values both <0.05), while the CD177 level and the CD177/CD10 ratio were significantly increased (P<0.05). The established normal reference range for the CD177/CD10 ratio was 0-0.64. Conclusions The CD177/CD10 ratio in neutrophils has a certain predictive value for the infection risk in burn patients, and its predictive value is higher than that of white blood cell count, neutrophil count, neutrophil, C-reactive protein level, procalcitonin level, and SOFA score. The established normal reference range for the CD177/CD10 ratio is 0-0.64.
Li HY,Huang JM,Mei YW,et al.Value of the CD177/CD10 ratio in neutrophils in predicting infection risk in burn patients and the establishment of its normal reference range[J].Chin J Burns Wounds,2026,42(6):579-588.DOI: 10.3760/cma.j.cn501225-20251118-00473.


 Abstract
Abstract PDF
PDF