- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
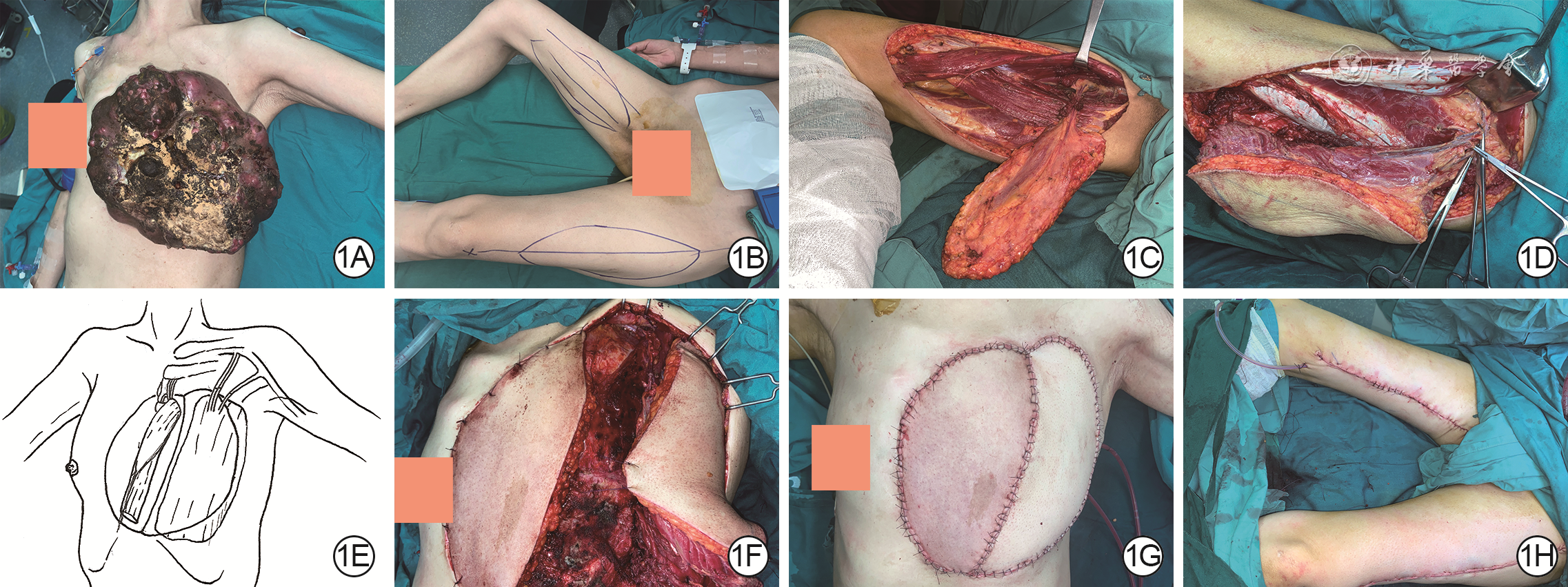
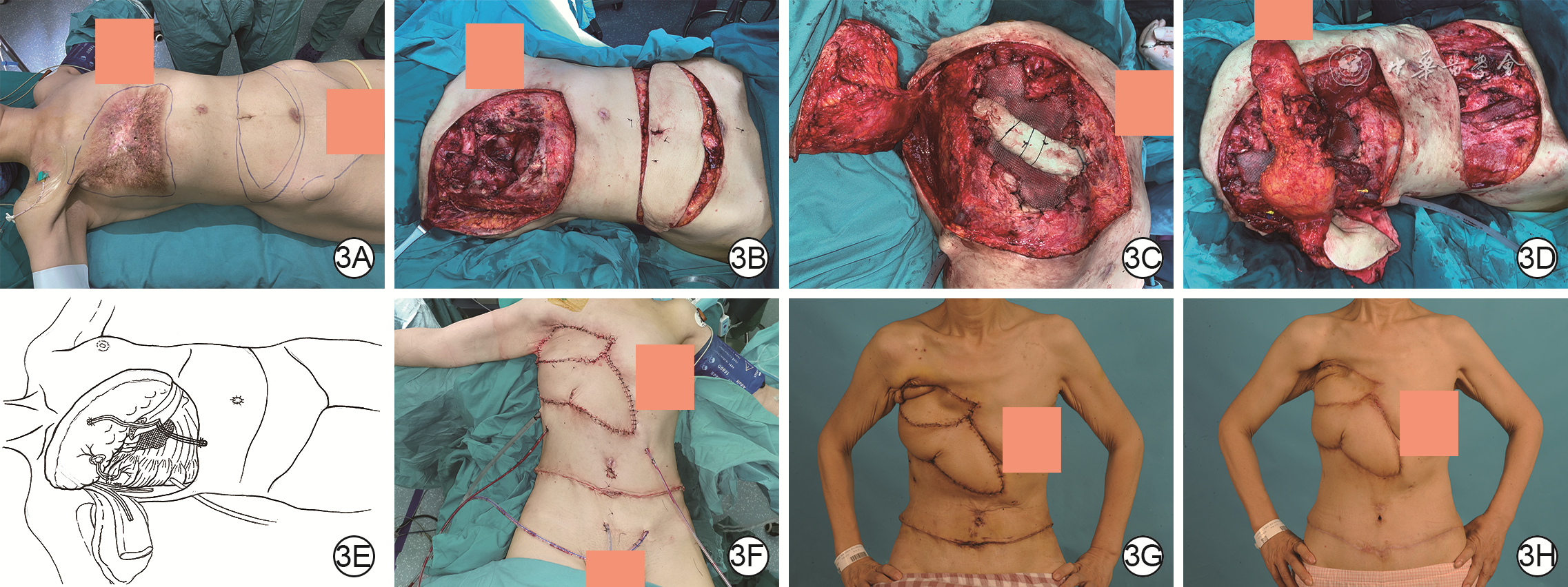
| Citation: | Yu JY,Song DJ,Liu X,et al.Clinical effects of combined tissue flap transplantation for repairing
|

| [1] |
SongD,LiuD,PafitanisG,et al.Extensive microsurgical reconstruction of chest wall defects for locally advanced breast cancer: a 10-year single-unit experience[J].Ann Plast Surg,2020,84(3):293-299.DOI: 10.1097/SAP.0000000000002000.
|
| [2] |
宋达疆,李赞,周晓,等.局部晚期乳腺癌切除术后巨大复杂创面的整形外科修复[J].中华整形外科杂志,2018,34(8):630-635.DOI: 10.3760/cma.j.issn.1009-4598.2018.08.011.
|
| [3] |
MillerDL,DurdenFL.Chest wall reconstruction utilizing ovine-derived reinforced tissue matrix[J].Ann Thorac Surg,2023,115(5):1266-1272.DOI: 10.1016/j.athoracsur.2021.12.062.
|
| [4] |
YoshiokaN.Versatility of the latissimus dorsi free flap during the treatment of complex postcraniotomy surgical site infections[J].Plast Reconstr Surg Glob Open,2017,5(6):e1355.DOI: 10.1097/GOX.0000000000001355.
|
| [5] |
HaratiK,KolbenschlagJ,BehrB,et al.Thoracic wall reconstruction after tumor resection[J].Front Oncol,2015,5:247.DOI: 10.3389/fonc.2015.00247.
|
| [6] |
CorkumJP,GarveyPB,BaumannDP,et al.Reconstruction of massive chest wall defects: a 20-year experience[J].J Plast Reconstr Aesthet Surg,2020,73(6):1091-1098.DOI: 10.1016/j.bjps.2020.02.010.
|
| [7] |
VanstraelenS,BainsMS,DycocoJ,et al.Biologic versus synthetic prosthesis for chest wall reconstruction: a matched analysis[J].Eur J Cardiothorac Surg,2023,64(6):ezad348.DOI: 10.1093/ejcts/ezad348.
|
| [8] |
WangCM,ZhangR,LuoP,et al.Reconstruction of extensive thoracic wall defect using the external oblique myocutaneous flap: an analysis on 20 Chinese patients with locally advanced soft tissue sarcoma[J].J Surg Oncol,2018,117(2):130-136.DOI: 10.1002/jso.24823.
|
| [9] |
ZhaoZQ,ZhuXQ,ZhuMR,et al.Chest wall reconstruction of male: latissimus dorsi Kiss flap, rectus abdominis flap and titanium-mesh[J].Asian J Surg,2022,45(7):1443-1444.DOI: 10.1016/j.asjsur.2022.02.041.
|
| [10] |
NaoumGE,SalamaL,HoA,et al.The impact of chest wall boost on reconstruction complications and local control in patients treated for breast cancer[J].Int J Radiat Oncol Biol Phys,2019,105(1):155-164.DOI: 10.1016/j.ijrobp.2019.04.027.
|
| [11] |
SaloJ,TukiainenEJ.Oncologic resection and reconstruction of the chest wall: a 19-year experience in a single center[J].Plast Reconstr Surg,2018,142(2):536-547.DOI: 10.1097/PRS.0000000000004597.
|
| [12] |
SongD,LiJ,PafitanisG,et al.Bilateral anterolateral thigh myocutaneous flaps for giant complex chest wall reconstruction[J].Ann Plast Surg,2021,87(3):298-309.DOI: 10.1097/SAP.0000000000002860.
|
| [13] |
AlsharkawyK,YoussifS,MalahiasM,et al.Acromiothoracic venous supercharge for abdominal-based free flaps in breast and chest wall reconstruction[J].Ann Plast Surg,2023,91(6):734-739.DOI: 10.1097/SAP.0000000000003704.
|
| [14] |
VanstraelenS,AliB,BainsMS,et al.The contribution of microvascular free flaps and pedicled flaps to successful chest wall surgery[J].J Thorac Cardiovasc Surg,2023,166(4):1262-1272.e2.DOI: 10.1016/j.jtcvs.2023.05.018.
|
| [15] |
KimWJ,KimWS,KimHK,et al.Reconstruction of small chest wall defects caused by tubercular abscesses using two different flaps[J].Ann Thorac Surg,2018,106(5):e249-e251.DOI: 10.1016/j.athoracsur.2018.04.019.
|
| [16] |
LinYN,Ou-YangF,HsiehMC,et al.Use of extended pedicled transverse rectus abdominis myocutaneous flap for extensive chest wall defect reconstruction after mastectomy for locally advanced breast cancer[J].Ann Plast Surg,2020,84(1S Suppl 1):S34-39.DOI: 10.1097/SAP.0000000000002188.
|
| [17] |
KimJ,LeeKT.Microsurgical reconstruction using thoracoacromial vessels as recipients for complicated chest wall defects[J].Microsurgery,2024,44(4):e31164.DOI: 10.1002/micr.31164.
|
| [18] |
FreyJD,MotoskoCC,MooreK,et al.A novel periareolar approach to chest wall reconstruction using a nipple-areola complex transposition flap[J].Plast Reconstr Surg,2019,144(3):528e-530e.DOI: 10.1097/PRS.0000000000005926.
|
| [19] |
KhalilHH, KalkatM. Therapeutic mammoplasty and dermal flap: a novel hybrid approach for chest wall reconstruction[J]. Plast Reconstr Surg Glob Open, 2020,8(3):e2593. DOI: 10.1097/GOX.0000000000002593.
|
| [20] |
OuyangY,XuB,LuanJ,et al.Chest wall reconstruction in male poland syndrome patients with endoscopic-assisted latissimus dorsi muscle flap transfer[J].J Plast Reconstr Aesthet Surg,2021,74(11):3141-3149.DOI: 10.1016/j.bjps.2021.03.117.
|
| [21] |
MericliAF,MurariuD,NemirS,et al.Soft-tissue reconstruction after composite vertebrectomy and chest wall resection for spinal tumors[J].Plast Reconstr Surg,2020,145(5):1275-1286.DOI: 10.1097/PRS.0000000000006792.
|
| [22] |
ZhouB,LongY,LiS,et al.Reconstruction of chronic radiation-induced ulcers in the chest wall using free and pedicle flaps[J].Front Surg,2022,9:1010990.DOI: 10.3389/fsurg.2022.1010990.
|
| [23] |
MarshDJ,ChanaJS.Reconstruction of very large defects: a novel application of the double skin paddle anterolateral thigh flap design provides for primary donor-site closure[J].J Plast Reconstr Aesthet Surg,2010,63(1):120-125.DOI: 10.1016/j.bjps.2008.08.022.
|
| [24] |
DurganDM,De La Cruz Ku G,ThomasM,et al.Chest wall resection for breast cancer: 21st century Mayo clinic experience[J].J Surg Oncol,2022,126(6):962-969.DOI: 10.1002/jso.27014.
|
| [25] |
ZhangYX,HayakawaTJ,LevinLS,et al.The economy in autologous tissue transfer: part 1. The kiss flap technique[J].Plast Reconstr Surg,2016,137(3):1018-1030.DOI: 10.1097/01.prs.0000479971.99309.21.
|
| [26] |
Russell PintoT,MoraH,PeleteiroB,et al.Chest wall perforator flaps for partial breast reconstruction after conservative surgery: prospective analysis of safety and reliability[J].Surg Oncol,2023,51:102015.DOI: 10.1016/j.suronc.2023.102015.
|
| [27] |
HashemiA,GimenezA,YimN,et al.Anterior chest wall reconstruction after separation of thoraco-omphalopagus conjoined twins with cadaveric rib grafts and omental flap[J].Ann Plast Surg,2023,91(6):753-757.DOI: 10.1097/SAP.0000000000003645.
|
| [28] |
LeeS, JungY, BaeY. Immediate chest wall reconstruction using an external oblique myocutaneous flap for large skin defects after mastectomy in advanced or recurrent breast cancer patients: a single center experience[J]. J Surg Oncol, 2018,117(2):124-129.DOI: 10.1002/jso.24830.
|
| [29] |
李鹏程,贾赤宇,李东杰,等.部分去表皮局部皮瓣修复结核性胸壁缺损创面的临床效果[J].中华烧伤杂志,2021,37(12):1110-1115.DOI: 10.3760/cma.j.cn501120-20210929-00337.
|
| [30] |
陈斓,张伟,谢卫国,等. 扩张髂腹股沟皮瓣游离移植整复大面积烧伤后严重瘢痕挛缩畸形的临床效果[J]. 中华烧伤与创面修复杂志,2022,38(4):321-327. DOI: 10.3760/cma.j.cn501225-20220210-00021.
|

Figures(4)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: