- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
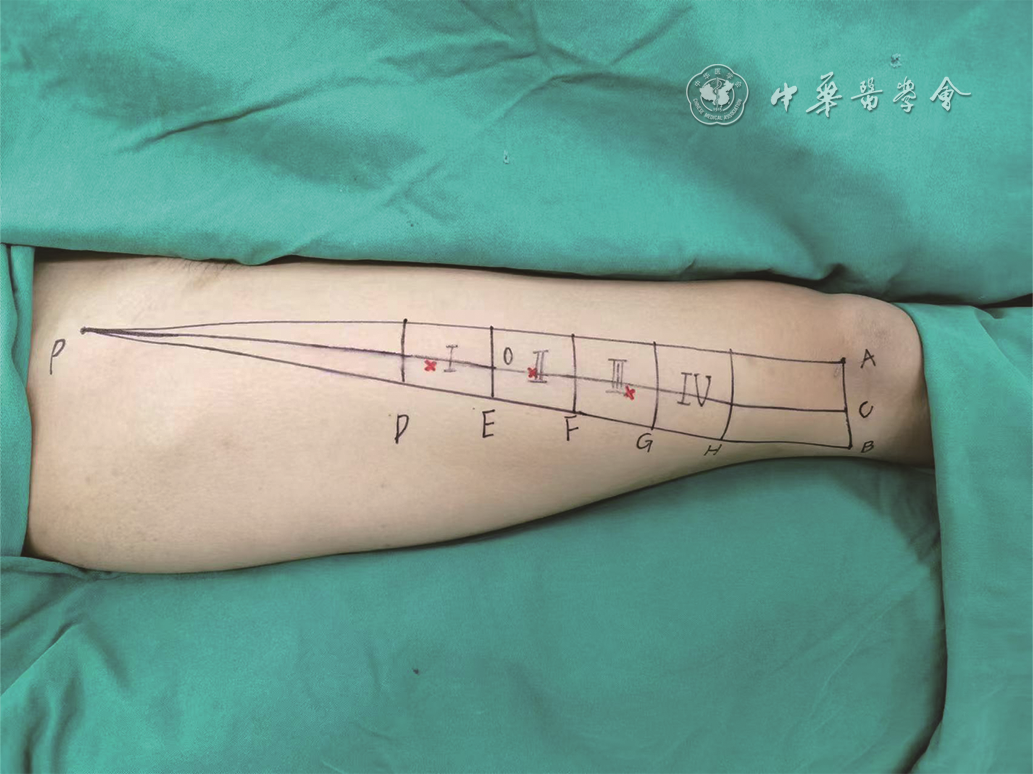
| Citation: | Wu XK,Li H,Wu BH,et al.Clinical application effects of the "novel three-longitude and five-transverse method" for perforator localization of anterolateral thigh chimeric flaps[J].Chin J Burns Wounds,2026,42(3):244-251.DOI: 10.3760/cma.j.cn501225-20240520-00188.

|

| [1] |
杨亮,周荣,巨积辉,等.游离双侧股前外侧内增压型串联皮瓣修复足踝部大面积创面的临床疗效[J].中华烧伤与创面修复杂志,2025,41(1):61-69.DOI: 10.3760/cma.j.cn501225-20240508-00164.
|
| [2] |
周耀,唐林峰,杨林,等.以旋股外侧动脉斜支和降支为蒂的股前外侧穿支皮瓣修复四肢创面效果的对比[J].中华显微外科杂志,2025,48(4):373-381.DOI: 10.3760/cma.j.cn441206-20241119-00251.
|
| [3] |
韩飞,张万福,佟琳,等.阔筋膜-股前外侧皮瓣复合移植修复颌面部根治性肿瘤切除术后复杂缺损的临床效果[J].中华烧伤与创面修复杂志,2025,41(5):440-446.DOI: 10.3760/cma.j.cn501225-20240801-00290.
|
| [4] |
AliRS,Bluebond-LangnerR,RodriguezED,et al.The versatility of the anterolateral thigh flap[J].Plast Reconstr Surg,2009,124(6Suppl):Se395-Se407.DOI: 10.1097/PRS.0b013e3181bcf05c.
|
| [5] |
ChaHG,HurJ,AhnC,et al.Ultrathin anterolateral thigh free flap: an adipocutaneous flap with the most superficial elevation plane[J].Plast Reconstr Surg,2023,152(4):718e-723e.DOI: 10.1097/PRS.0000000000010295.
|
| [6] |
MelecaJB, KerrRP, PrendesBL, et al. Anterolateral thigh fascia lata rescue flap: a new weapon in the battle against osteoradionecrosis[J].Laryngoscope, 2021, 131(12): 2688-2693. DOI: 10.1002/lary.29709.
|
| [7] |
徐永清,唐举玉,刘元波,等.股前外侧皮瓣穿支解剖学特征与定位方法的专家共识(2024版)[J].中国临床解剖学杂志,2024,42(5):489-499.DOI: 10.13418/j.issn.1001-165x.2024.5.01.
|
| [8] |
IllgC, KraussS, LauerH, et al. Precision of dynamic infrared thermography in anterolateral thigh flap planning: identification of the perforator fascia passage[J]. J Reconstr Microsurg, 2023, 39(6): 413-418. DOI: 10.1055/s-0042-1758183.
|
| [9] |
ViscontiG, BianchiA, HayashiA, et al. Designing an anterolateral thigh flap using ultrasound[J]. J Reconstr Microsurg, 2022, 38(3): 206-216. DOI: 10.1055/s-0041-1740126.
|
| [10] |
HuY, WangY, CaoS, et al. Customizing anterolateral thigh flap with magnetic resonance angiography differential subsampling with cartesian ordering imaging for individualized reconstruction of extremity defects[J]. J Surg Res, 2023, 283: 733-742. DOI: 10.1016/j.jss.2022.11.036.
|
| [11] |
KimS,LeeHR,YunJH,et al.Preoperative perforator localization in anterolateral thigh free flap using acoustic Doppler and computed tomography angiography[J].Laryngoscope Investig Otolaryngol,2022,7(6):1790-1797.DOI: 10.1002/lio2.958.
|
| [12] |
YuXX,YangSF,JiCS,et al.A novel computed tomography angiography technique: guided preoperative localization and design of anterolateral thigh perforator flap[J].Insights Imaging,2022,13(1):190.DOI: 10.1186/s13244-022-01318-0.
|
| [13] |
李贤海,周建东,郑杰,等.红外热成像结合高频彩色多普勒超声定位浅筋膜穿支在超薄股前外侧皮瓣切取中的应用[J].中华显微外科杂志,2024,47(6):635-640.DOI: 10.3760/cma.j.cn441206-20240205-00041.
|
| [14] |
张宇轩,许亚军,周建东,等.宽频线阵容积探头引导下三维超声技术在股前外侧穿支皮瓣术前穿支定位中的应用[J].中华显微外科杂志,2024,47(1):17-21.DOI: 10.3760/cma.j.cn441206-20230815-00015.
|
| [15] |
周飞亚,张弦,蔡乐益,等.精准定位的微型股前外侧穿支皮瓣修复手指中等面积皮肤软组织缺损的效果[J].中华烧伤与创面修复杂志,2024,40(2):165-171.DOI: 10.3760/cma.j.cn501225-20231030-00150.
|
| [16] |
董帅,王石,滕志成,等.吲哚菁绿血管造影联合彩色多普勒超声在股前外侧穿支皮瓣穿支定位中的临床应用效果[J].中华烧伤与创面修复杂志,2025,41(11):1091-1100.DOI: 10.3760/cma.j.cn501225-20240629-00254.
|
| [17] |
XuDC,ZhongSZ,KongJM,et al.Applied anatomy of the anterolateral femoral flap[J].Plast Reconstr Surg,1988,82(2):305-310.
|
| [18] |
YuP,YoussefA.Efficacy of the handheld Doppler in preoperative identification of the cutaneous perforators in the anterolateral thigh flap[J].Plast Reconstr Surg,2006,118(4):928-933.DOI: 10.1097/01.prs.0000232216.34854.63.
|
| [19] |
DengC, ChangS, WeiZ, et al. Alternative design for anterolateral thigh multi-paddled flaps: the 3-5 system[J]. Med Sci Monit, 2018, 24: 9102-9109. DOI: 10.12659/MSM.911883.
|
| [20] |
常树森,魏在荣,金文虎,等.股前外侧皮瓣三纵五横法设计方案的临床研究[J].中华整形外科杂志,2019,35(6):571-576.DOI: 10.3760/cma.j.issn.1009-4598.2019.06.011.
|
| [21] |
胡涛涛,常树森,魏在荣,等.改良三纵五横法在股前外侧穿支皮瓣修复术前穿支定位中的应用研究[J].中国修复重建外科杂志,2021,35(8):1027-1032.DOI: 10.7507/1002-1892.202103074.
|
| [22] |
常树森,莫小金,魏在荣,等. 遵义缝合法在股前外侧皮瓣供区缝合中的应用研究[J]. 中国修复重建外科杂志,2021,35(4):477-482. DOI: 10.7507/1002-1892.202008101.
|
| [23] |
魏在荣,王达利,黄广涛.毁损性创面的治疗进展[J/OL].中华损伤与修复杂志(电子版),2019,14(2):85-90[2024-05-20]. https://rs.yiigle.com/cmaid/1129420.DOI: 10.3877/cma.j.issn.1673-9450.2019.02.002.
|
| [24] |
胡大海,张月.毁损性创面修复重建技术及策略探索[J].中华烧伤与创面修复杂志,2024,40(9):812-817.DOI: 10.3760/cma.j.cn501225-20240807-00296.
|
| [25] |
MarttilaE, SalliM, MesimäkiK, et al. The combined anterolateral thigh-partial iliac crest minihybrid free flap for mandibular reconstruction[J]. Microsurgery, 2022, 42(4): 312-318. DOI: 10.1002/micr.30854.
|
| [26] |
DI SummaPG, WatfaW, CampisiC, et al. Free versus pedicled anterolateral thigh flap for abdominal wall reconstruction[J]. Anticancer Res, 2019, 39(12): 6759-6768. DOI: 10.21873/anticanres.13891.
|
| [27] |
SơnTT, NghĩaPT, DungPTV, et al. Facial reconstruction with thinned anterolateral thigh free flap[J]. BMC Surg, 2024, 24(1): 296. DOI: 10.1186/s12893-024-02587-w.
|
| [28] |
YangZ, XuC, ZhuY, et al. Flow-through free anterolateral thigh flap in reconstruction of severe limb injury[J]. Ann Plast Surg, 2020, 84(5S Suppl 3): S165-S170. DOI: 10.1097/SAP.0000000000002372.
|
| [29] |
吴育煜,胡朝波,陈绵川,等.股前内侧穿支内增压技术在股前外侧穿支皮瓣修复大面积缺损中的应用[J].组织工程与重建外科杂志,2023,19(2):141-145.DOI: 10.3969/j.issn.1673-0364.2023.02.007.
|
| [30] |
赵铭,李涛.联体形式的股前外侧穿支皮瓣修复特殊类型创面的临床应用[J].中华显微外科杂志,2018,41(2):181-184.DOI: 10.3760/cma.j.issn.1001-2036.2018.02.022.
|
| [31] |
巨积辉,李雷,徐磊,等.双血供来源的超长胸脐联体穿支皮瓣修复前臂大面积皮肤缺损[J].中华显微外科杂志,2018,41(2):137-141.DOI: 10.3760/cma.j.issn.1001-2036.2018.02.009.
|
| [32] |
杨锐,高伟航,张子阳,等.静脉超引流技术在逆行旋股外侧动脉降支穿支皮瓣修复膝关节软组织缺损中的应用效果[J].中华创伤杂志,2025,41(4):387-390.DOI: 10.3760/cma.j.cn501098-20241127-00672.
|
| [33] |
MatsuiC,EscandónJM,MohammadA,et al.Clinical applications of the chimeric anterolateral thigh (ALT) flap in head and neck reconstruction[J].Acta Chir Belg,2023,123(5):473-480.DOI: 10.1080/00015458.2022.2073016.
|
| [34] |
WangKC, HungKS, ChangTY, et al. Temporary ectopic implantation of an amputated leg using the distal runoff vessel of the anterolateral thigh flap followed by subsequent prefabricated chimeric replantation[J]. Ann Plast Surg, 2019, 82(1): 71-75. DOI: 10.1097/SAP.0000000000001630.
|
| [35] |
ChenX, ZhangC, ChengL, et al. Survival and versatility of the flow-through lateral-thigh free flap in severe electrical injuries to the wrist[J]. Ann Plast Surg, 2020, 85(6): 612-617. DOI: 10.1097/SAP.0000000000002355.
|
| [36] |
尹善青,竺枫,黄耀鹏,等.修薄的股前外侧穿支皮瓣联合分指及指蹼成形术序贯治疗全手脱套毁损性创面的效果[J].中华烧伤与创面修复杂志,2024,40(11):1052-1058.DOI: 10.3760/cma.j.cn501225-20240723-00275.
|
| [37] |
HsiehF, LeowOQY, CheongCF, et al. Musculoseptocutaneous perforator of anterolateral thigh flap: a clinical study[J]. Plast Reconstr Surg, 2021, 147(1): 103e-110e. DOI: 10.1097/PRS.0000000000007471.
|
| [38] |
孙浩然,欧阳阳钢,刘璐,等.接合神经的游离股前外侧穿支皮瓣修复前足缺损的疗效[J].实用手外科杂志,2024,38(4):435-438.DOI: 10.3969/j.issn.1671-2722.2024.04.003.
|
| [39] |
陈占斌,曹广超,杨龙,等.带阔筋膜游离股前外侧皮瓣修复伴肌腱缺损的创面[J].实用手外科杂志,2021,35(3):320-323.DOI: 10.3969/j.issn.1671-2722.2021.03.015.
|
| [40] |
GraboyesEM,HornigJD.Evolution of the anterolateral thigh free flap[J].Curr Opin Otolaryngol Head Neck Surg,2017,25(5):416-421.DOI: 10.1097/MOO.0000000000000394.
|
 吴祥奎 3月9日.mp4
吴祥奎 3月9日.mp4
|

|

Figures(4) / Tables(1)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: