Abstract:
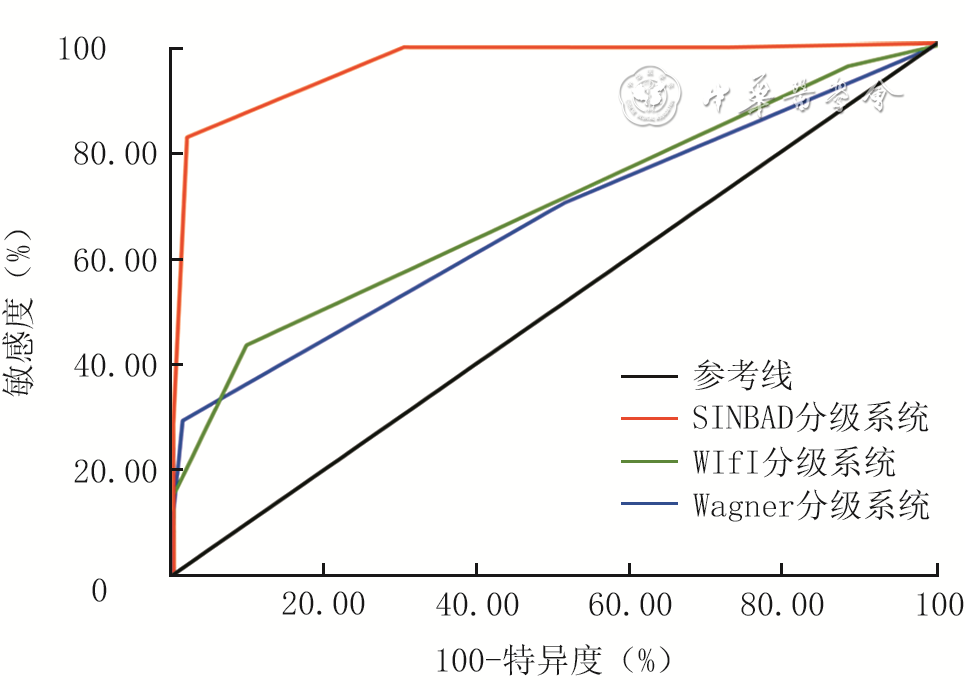
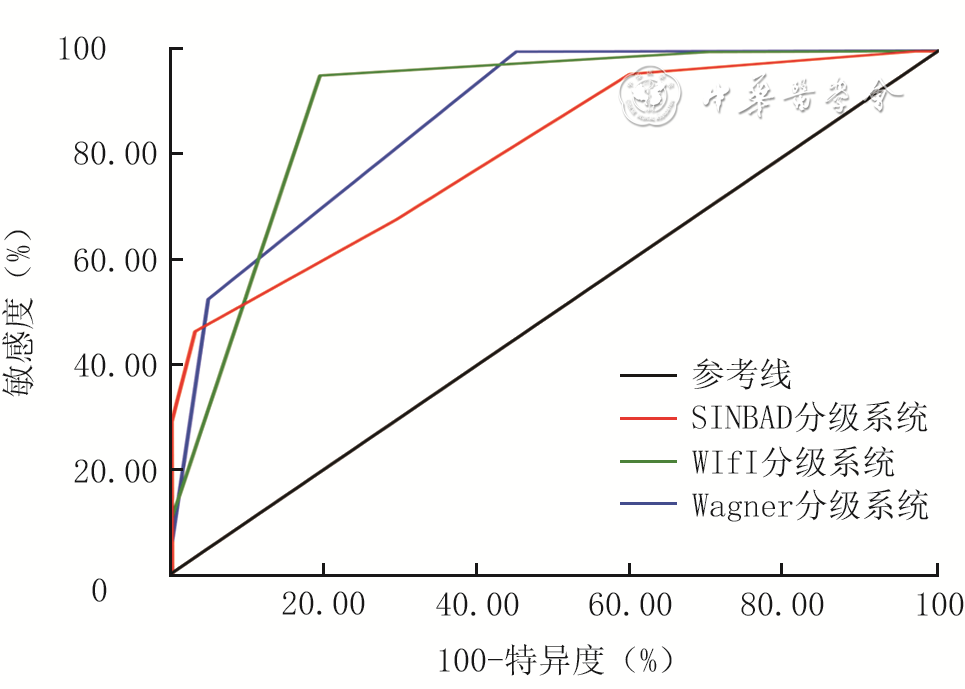
Objective To compare the predictive efficacy of the Wagner grading system, site, ischemia, neuropathy, bacterial infection, area, depth (SINBAD) grading system, and wound, ischemia and foot infection (WIfI) grading system for short-term wound non-healing and amputation in patients with diabetic foot ulcers (DFUs). Methods The study was a retrospective cohort study. From January 2023 to December 2024, 400 patients with DFUs who met the inclusion criteria were admitted to the Diabetic Foot Center of the Central Hospital of Wuhan of Tongji Medical College of Huazhong University of Science and Technology. All patients were assessed with Wagner grade, SINBAD score, and WIfI stage within 48 hours of admission. There were 232 males and 168 females, aged 44 to 83 years. Based on whether the wound had healed at 3 months after initial admission, patients were divided into healing group (194 cases) and non-healing group (206 cases); based on amputation, patients who underwent major or minor amputation were included in amputation group (255 cases), while the remaining patients were included in non-amputation group (145 cases); the Wagner grades, SINBAD scores, and WIfI stages of patients in each group were recorded. The amputation and non-healing wound at 3 months after initial admission in patients with different Wagner grades, SINBAD scores, and WIfI stages were compared. Spearman correlation analysis was used to assess the correlation between the Wagner grades, SINBAD scores, WIfI stages and the wound healing time in patients with DFUs. The receiver operating characteristic curves were plotted to evaluate the predictive efficacy of each grading system for non-healing wound at 3 months after initial admission (i.e., short-term wound non-healing) and amputation in patients with DFUs, and the DeLong test was used to compare the differences in the area under the receiver operating characteristic curve (AUROC) among the grading systems. Results The patients in non-healing group and amputation group had significantly higher Wagner grades, SINBAD scores, and WIfI stages than those in healing group and non-amputation group, respectively (with t values of 8.25, 19.78, and 9.87, 14.05, 11.73, and 16.45, respectively, P<0.05). Among patients with different Wagner grades, SINBAD scores, and WIfI stages, the proportion of amputees and the proportion of patients with non-healing wounds at 3 months after initial admission showed statistically significant differences (with χ2 values of 150.35 and 73.97, 133.84 and 221.10, 187.63 and 83.37, respectively, P<0.05). The Wagner grades, SINBAD scores, and WIfI stages were all significantly positively correlated with the wound healing time in patients with DFUs (with rs values of 0.52, 0.70, and 0.52, respectively, P<0.05). With wounds unhealed at 3 months after initial admission as the prognostic outcome, the SINBAD grading system had the highest AUROC of 0.96 (with 95% CI of 0.94-0.98) and a maximum Youden index of 0.80; the Wagner grading system showed an AUROC of 0.66 (with 95% CI of 0.61-0.72) and a maximum Youden index of 0.28; the WIfI grading system showed an AUROC of 0.69 (with 95% CI of 0.64-0.74) and a maximum Youden index of 0.33. The DeLong test indicated that the predictive efficacy of the SINBAD grading system for short-term wound non-healing in patients with DFUs was significantly superior to that of the Wagner grading system and WIfI grading system, respectively (with Z values of 12.52 and 12.97, respectively, P values both <0.05). With amputation as the prognostic outcome, the WIfI grading system had the highest AUROC of 0.89 (with 95% CI of 0.85-0.93) and a maximum Youden index of 0.75; the Wagner grading system showed an AUROC of 0.87 (with 95% CI of 0.83-0.91) and a maximum Youden index of 0.55; the SINBAD grading system showed an AUROC of 0.80 (with 95% CI of 0.76-0.84) and a maximum Youden index of 0.43. The DeLong test showed that the predictive efficacy of both the WIfI grading system and Wagner grading system for amputation in patients with DFUs was significantly superior to that of the SINBAD grading system, respectively (with Z values of 3.76 and 2.96, respectively, P<0.05). Conclusions The Wagner grading system, SINBAD grading system, and WIfI grading system can all effectively predict the risk of short-term wound non-healing and amputation in patients with DFUs. The SINBAD grading system performs the best in predicting short-term wound non-healing, while the WIfI grading system has an advantage in predicting amputation. Although the Wagner grading system has poorer predictive efficacy for short-term wound non-healing, it still demonstrates good predictive efficacy for amputation. In clinical practice, different grading systems can be used in combination based on the focus of assessment.
Xu ZH,Duan WZ,Xie WG,et al.Comparison of the predictive efficacy of the Wagner, SINBAD, and WIfI grading systems for short-term wound non-healing and amputation in patients with DFUs[J].Chin J Burns Wounds,2026,42(3):234-243.DOI: 10.3760/cma.j.cn501225-20251129-00494.


 Abstract
Abstract PDF
PDF