- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
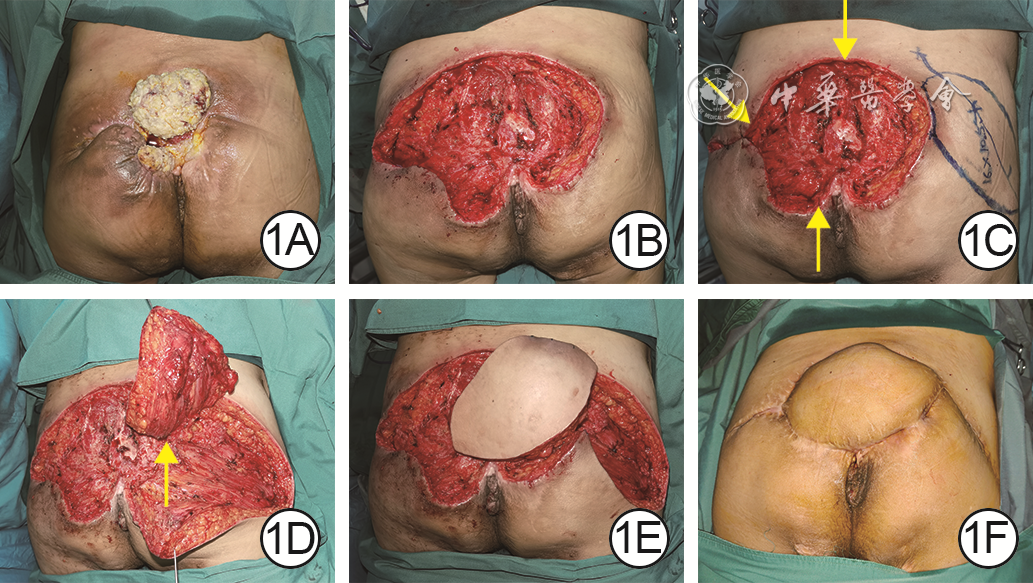
| Citation: | Li J,Liu MD,Zhu L,et al.Clinical effect of unilateral superior gluteal artery perforator propeller flap combined with contralateral centripetal advancement flap in repairing huge pressure ulcers in the sacrococcygeal region[J].Chin J Burns Wounds,2024,40(6):551-556.DOI: 10.3760/cma.j.cn501225-20231031-00158.

|

| [1] |
MervisJS, PhillipsTJ. Pressure ulcers: prevention and management[J]. J Am Acad Dermatol, 2019,81(4):893-902. DOI: 10.1016/j.jaad.2018.12.068.
|
| [2] |
HeadlamJ, IllsleyA. Pressure ulcers: an overview[J]. Br J Hosp Med (Lond), 2020,81(12):1-9. DOI: 10.12968/hmed.2020.0074.
|
| [3] |
MervisJS, PhillipsTJ. Pressure ulcers: pathophysiology, epidemiology, risk factors, and presentation[J]. J Am Acad Dermatol, 2019,81(4):881-890. DOI: 10.1016/j.jaad.2018.12.069.
|
| [4] |
JiaoX, CuiC, NgSK, et al. The modified bilobed flap for reconstructing sacral decubitus ulcers[J/OL]. Burns Trauma, 2020,8:tkaa012[2023-10-31]. https://pubmed.ncbi.nlm.nih.gov/33335930/. DOI: 10.1093/burnst/tkaa012.
|
| [5] |
黄啟云, 林红华. 改良全臀大肌旋转肌皮瓣治疗骶尾部压疮的疗效观察[J].实用骨科杂志,2019,25(8):746-748.
|
| [6] |
夏卫东, 屠卓隆, 赵胜, 等. 负压封闭引流联合保留臀上动脉浅支的臀大肌肌皮瓣修复骶尾部Ⅳ期压疮的临床效果[J]. 温州医科大学学报, 2024,54(4):318-322.
|
| [7] |
钟泉, 古仲航, 候思政. 带部分臀大肌肌皮瓣旋转修复联合简易负压封闭引流治疗骶尾部难治性压疮的临床应用[J].医药前沿,2023,13(25):72-74.
|
| [8] |
丁云林, 王少根, 姜金珠. 负压封闭引流联合臀上动脉穿支皮瓣修复骶尾部压疮[J]. 中国美容医学, 2022,31(11):16-19.
|
| [9] |
史宸硕, 唐修俊, 王达利, 等. 臀上动脉穿支岛状皮瓣修复骶尾部压疮的临床效果[J].中华烧伤杂志,2019,35(5):367-370. DOI: 10.3760/cma.j.issn.1009-2587.2019.05.008.
|
| [10] |
陈黎明, 王刚, 刘宏, 等. 臀部自由穿支螺旋桨肌皮瓣修复合并深部死腔的臀部复杂性创面的临床效果[J].中华烧伤与创面修复杂志,2023,39(8):753-757. DOI: 10.3760/cma.j.cn501225-20221115-00488.
|
| [11] |
孙佳琳, 郭鹏飞, 崔正军, 等. 臀上动脉穿支接力皮瓣修复骶尾部压疮的临床效果[J].中华烧伤杂志,2020,36(8):726-729. DOI: 10.3760/cma.j.cn501120-20190607-00265.
|
| [12] |
龙照忠, 张莉莉, 王彤华, 等. VSD序贯结合PRP及臀上动脉穿支皮瓣修复骶尾部压疮[J].中国美容医学,2022,31(11):9-11,125.
|
| [13] |
陈凯, 张玉玲, 许喜生, 等. 臀上动脉穿支螺旋桨皮瓣结合PU-VSD在骶尾部压疮修复中的应用[J]. 湘南学院学报(医学版), 2022,24(4):32-35.
|
| [14] |
隆腾飞, 张轩轩, 赵辉, 等. 基于三维CT的臀上动脉解剖学研究[J]. 中国临床解剖学杂志, 2013,31(4):402-406. DOI: 10.7666/d.Y2405990.
|
| [15] |
沈佳祚, 官世水, 郑毅全, 等. 臀上动脉穿支肌皮瓣修复腰骶部深度缺损难愈合创面[J]. 临床骨科杂志, 2023,26(6):809-812. DOI: 10.3969/j.issn.1008-0287.2023.06.016.
|
| [16] |
金文虎, 李海, 常树森, 等. 臀上动脉穿支蒂V-Y推进皮瓣治疗骶尾部压疮的效果评价[J].中华创伤杂志,2019,35(12):1138-1141. DOI: 10.3760/cma.j.issn.1001-8050.2019.12.014.
|
| [17] |
王君, 井刚, 潘云川, 等. 臀上动脉穿支皮瓣修复骶尾部Ⅳ期压疮12例[J].中华显微外科杂志,2019,42(6):602-604. DOI: 10.3760/cma.j.issn.1001-2036.2019.06.024.
|
| [18] |
李承龙, 仲海燕, 陈勇, 等. 胸背动脉穿支皮瓣在肩胸背部创面修复中的临床应用[J].组织工程与重建外科杂志,2024,20(1):64-68. DOI: 10.3969/j.issn.1673-0364.2024.01.004.
|
| [19] |
何晓清, 范新宇, 徐永清. 腓动脉和胫后动脉穿支螺旋桨皮瓣的应用[J].中华显微外科杂志,2022,45(6):705-709. DOI: 10.3760/cma.j.cn441206-20220913-00190.
|
| [20] |
HyakusokuH, YamamotoT, FumiiriM. The propeller flap method[J]. Br J Plast Surg, 1991,44(1):53-54. DOI: 10.1016/0007-1226(91)90179-n.
|
| [21] |
邱致深, 宋坤, 伍逸婷, 等. 螺旋桨皮瓣在足踝部修复中应用的研究进展[J].解剖学杂志,2023,46(4):335-338. DOI: 10.3969/j.issn.1001-1633.2023.04.012.
|
| [22] |
陶友伦, 张世民. 穿支血管蒂螺旋桨皮瓣[J].中国临床解剖学杂志,2011,29(6):606-608,618.
|
| [23] |
HifnyMA, TohamyA, RabieO, et al. Propeller perforator flaps for coverage of soft tissue defects in the middle and distal lower extremities[J]. Ann Chir Plast Esthet, 2020,65(1):54-60. DOI: 10.1016/j.anplas.2019.04.002.
|
| [24] |
朱婷婷, 方小魁, 李光早, 等. 臀上动脉穿支皮瓣在修复骶尾部压疮的应用[J].蚌埠医学院学报,2019,44(3):332-334. DOI: 10.13898/j.cnki.issn.1000-2200.2019.03.014.
|
| [25] |
韦铭, 杨诚勇, 蓝芳令, 等. 太极皮瓣联合庆大霉素骨水泥治疗骶尾部巨大压疮效果观察[J].山东医药,2020,60(26):83-85. DOI: 10.3969/j.issn.1002-266X.2020.26.023.
|
| [26] |
王君, 潘云川, 徐家钦, 等. 双侧臀部旋转皮瓣修复骶尾部巨大压疮52例[J].中华烧伤杂志,2017,33(12):775-777. DOI: 10.3760/cma.j.issn.1009-2587.2017.12.011.
|
| [27] |
徐永清, 柴益民, 张世民, 等. 穿支螺旋桨皮瓣专家共识[J].中华显微外科杂志,2019,42(5):417-422. DOI: 10.3760/cma.j.issn.1001-2036.2019.05.001.
|
| [28] |
杨若梦, 刘元波, 朱珊, 等. 膝上外侧动脉穿支螺旋桨皮瓣修复膝关节周围软组织缺损[J].中国修复重建外科杂志,2021,35(12):1603-1608. DOI: 10.7507/1002-1892.202106024.
|
| [29] |
王扬剑, 李学渊, 王胜伟, 等. 术前多普勒定位的自由式穿支螺旋桨皮瓣设计[J].同济大学学报(医学版),2016,37(4):109-114. DOI: 10.16118/j.1008-0392.2016.04.022.
|
| [30] |
DingX, TangQ, XuZ, et al. Challenges and innovations in treating chronic and acute wound infections: from basic science to clinical practice[J/OL]. Burns Trauma, 2022,10:tkac014[2023-10-31]. https://pubmed.ncbi.nlm.nih.gov/35611318/.DOI: 10.1093/burnst/tkac014.
|

Figures(2)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: