- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
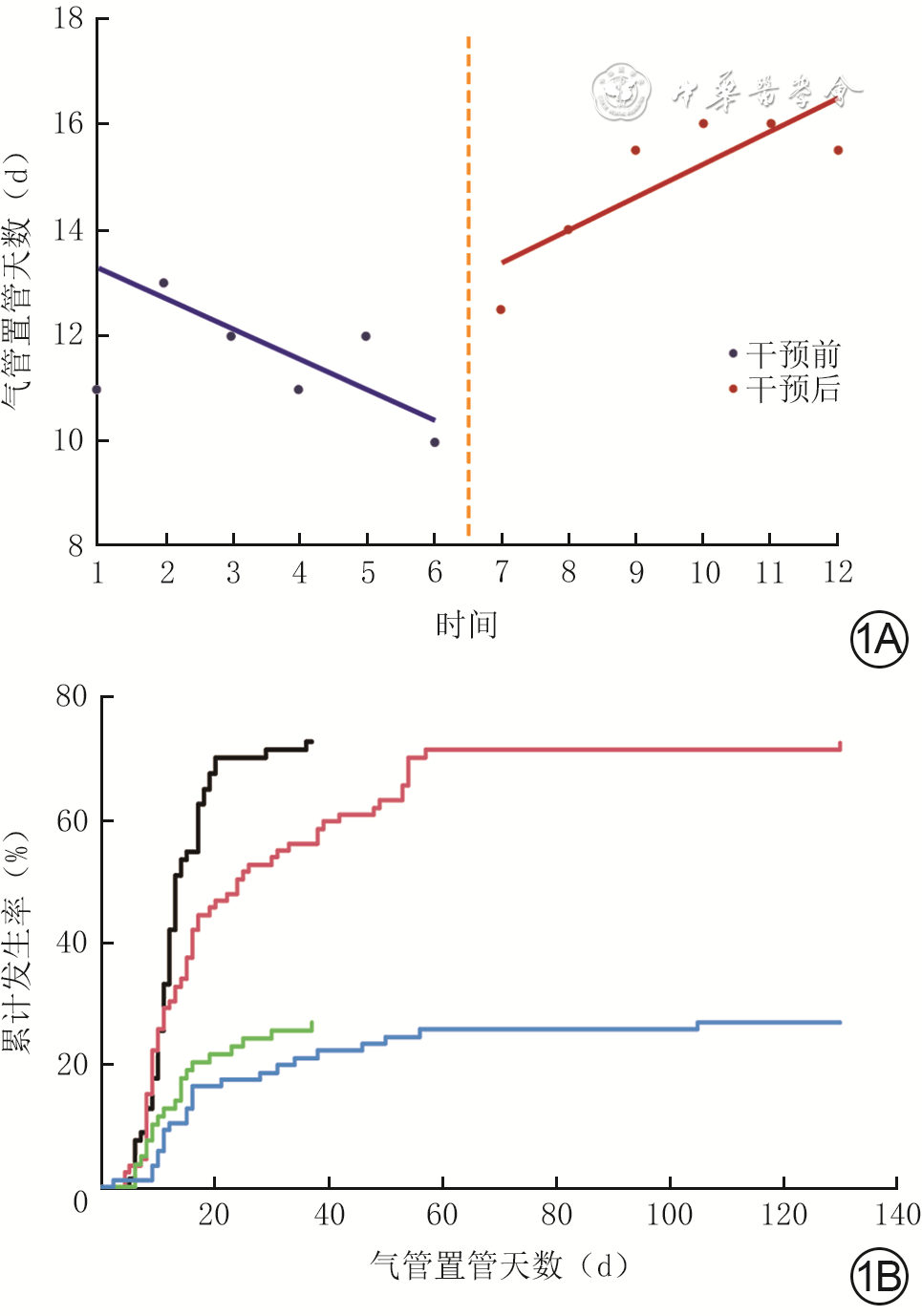
| Citation: | Pan YY,Fan YF.Effects of analgesic and sedation management in critical care medicine on patients with severe burns combined with inhalation injuries and the factors affecting tracheal intubation time[J].Chin J Burns Wounds,2024,40(12):1123-1131.DOI: 10.3760/cma.j.cn501225-20240625-00248.

|

| [1] |
YangJ,TianG,LiuJ,et al.Epidemiology and clinical characteristics of burns in mainland China from 2009 to 2018[J/OL].Burns Trauma,2022,10:tkac039[2024-06-25]. https://pubmed.ncbi.nlm.nih.gov/36196302/. DOI: 10.1093/burnst/tkac039.
|
| [2] |
OpriessnigE,LuzeH,SmolleC,et al.Epidemiology of burn injury and the ideal dressing in global burn care - regional differences explored[J].Burns,2023,49(1):1-14.DOI: 10.1016/j.burns.2022.06.018.
|
| [3] |
ChimaAM, MahmoudMA, NarayanasamyS. What is the role of dexmedetomidine in modern anesthesia and critical care? [J]. Adv Anesth, 2022,40(1):111-130. DOI: 10.1016/j.aan.2022.06.003.
|
| [4] |
ChanquesG,ConstantinJM,DevlinJW,et al.Analgesia and sedation in patients with ARDS[J].Intensive Care Med,2020,46(12):2342-2356.DOI: 10.1007/s00134-020-06307-9.
|
| [5] |
EgbutaC,MasonKP.Current state of analgesia and sedation in the pediatric intensive care unit[J].J Clin Med,2021,10(9):1847.DOI: 10.3390/jcm10091847.
|
| [6] |
BarrJ,FraserGL,PuntilloK,et al.Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit[J].Crit Care Med,2013,41(1):263-306.DOI: 10.1097/CCM.0b013e3182783b72.
|
| [7] |
DevlinJW,SkrobikY,GélinasC,et al.Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU[J].Crit Care Med,2018,46(9):e825-e873.DOI: 10.1097/CCM.0000000000003299.
|
| [8] |
HinkelbeinJ, LampertiM, AkesonJ, et al. European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults[J]. Eur J Anaesthesiol, 2018, 35(1):6-24. DOI: 10.1097/EJA.0000000000000683.
|
| [9] |
中华医学会重症医学分会.中国成人ICU镇痛和镇静治疗指南[J].中华危重病急救医学,2018,30(6):497-514.DOI: 10.3760/cma.j.issn.2095-4352.2018.06.001.
|
| [10] |
CinottiR,BesnardN,DesmedtL,et al.Feasibility and impact of the implementation of a clinical scale-based sedation-analgesia protocol in severe burn patients undergoing mechanical ventilation. A before-after bi-center study[J].Burns,2020,46(6):1310-1317.DOI: 10.1016/j.burns.2020.02.009.
|
| [11] |
朱峰,夏照帆.成人重症烧伤镇痛镇静管理[J].中华烧伤杂志,2018,34(6):407-411.DOI: 10.3760/cma.j.issn.1009-2587.2018.06.022.
|
| [12] |
杨宗城.烧伤治疗学[M].北京:人民卫生出版社, 2006.
|
| [13] |
吴军,唐丹,李曾慧平.烧伤康复治疗学[M].北京:人民卫生出版社, 2015.
|
| [14] |
路卫,夏照帆,陈旭林.吸入性损伤后预防性气管切开与紧急气管切开的临床研究[J].中华烧伤杂志,2003,19(4):233-235.DOI: 10.3760/cma.j.issn.1009-2587.2003.04.013.
|
| [15] |
GigengackRK,CleffkenBI,LoerSA.Advances in airway management and mechanical ventilation in inhalation injury[J].Curr Opin Anaesthesiol,2020,33(6):774-780.DOI: 10.1097/ACO.0000000000000929.
|
| [16] |
李世杰, 申传安. 烧伤合并吸入性损伤患者呼吸机相关肺炎的研究现状[J/CD]. 中华损伤与修复杂志(电子版), 2024, 9(4):351-355. DOI: 10.3877/cma.j.issn.1673-9450.2024.04.014
|
| [17] |
中国老年医学学会烧创伤分会. 吸入性损伤临床诊疗全国专家共识(2018版)[J]. 中华烧伤杂志,2018,34(11):770-775. DOI: 10.3760/cma.j.issn.1009-2587.2018.11.010.
|
| [18] |
UsmaniA,PipalDK,BaglaH,et al.Prediction of mortality in acute thermal burn patients using the abbreviated burn severity index score: a single-center experience[J].Cureus,2022,14(6):e26161.DOI: 10.7759/cureus.26161.
|
| [19] |
ZhangM,YangP,YuT,et al.Lytic cocktail: an effective method to alleviate severe burn induced hyper-metabolism through regulating white adipose tissue browning[J].Heliyon,2022,8(3):e09128.DOI: 10.1016/j.heliyon.2022.e09128.
|
| [20] |
曾宪锋,刘伟,李景春.冬眠Ⅰ号与地西泮治疗颅脑外伤伴躁动患者的疗效对比研究[J].临床合理用药杂志,2014,7(12C):59-60.DOI: 10.3969/j.issn.1674-3296.2014.36.040.
|
| [21] |
邵华,王琦琦,胡跃华,等.中断时间序列分析及其在公共卫生领域中的应用[J].中华流行病学杂志,2015,36(9):1015-1017.DOI: 10.3760/cma.j.issn.0254-6450.2015.09.023.
|
| [22] |
MagransR,FerreiraF,SarlabousL,et al.The effect of clusters of double triggering and ineffective efforts in critically ill patients[J].Crit Care Med,2022,50(7):e619-e629.DOI: 10.1097/CCM.0000000000005471.
|
| [23] |
AustinPC, PutterH, LeeDS,et al.Estimation of the absolute risk of cardiovascular disease and other events: issues with the use of multiple Fine-Gray subdistribution hazard models[J].Circ Cardiovasc Qual Outcomes,2022,15(2):e008368. DOI: 10.1161/CIRCOUTCOMES.121.008368.
|
| [24] |
JakobSM,RuokonenE,GroundsRM,et al.Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials[J].JAMA,2012,307(11):1151-1160.DOI: 10.1001/jama.2012.304.
|
| [25] |
HughesCG,MaillouxPT,DevlinJW,et al.Dexmedetomidine or propofol for sedation in mechanically ventilated adults with sepsis[J].N Engl J Med,2021,384(15):1424-1436.DOI: 10.1056/NEJMoa2024922.
|
| [26] |
中华医学会急诊医学分会危重症学组,中国急诊成人镇痛、镇静与谵妄管理专家共识组.中国急诊成人镇痛、镇静与谵妄管理专家共识[J].中华急诊医学杂志,2023,32(12):1594-1609.DOI: 10.3760/cma.j.issn.1671-0282.2023.12.004.
|
| [27] |
中华医学会儿科学分会急救学组,中华医学会急诊医学分会儿科学组,中华儿科杂志编辑委员会.中国儿童重症监护病房镇痛和镇静治疗专家共识(2024)[J].中华儿科杂志,2024,62(3):196-203.DOI: 10.3760/cma.j.cn112140-20231130-00400.
|
| [28] |
中华医学会呼吸病学分会,中国医师协会呼吸医师分会危重症医学专家组.成人呼吸危重症患者镇痛镇静管理及相关问题专家共识[J].中华结核和呼吸杂志,2023,46(12):1162-1175.DOI: 10.3760/cma.j.cn112147-20230901-00123.
|
| [29] |
张晗希,韩孟杰,周郁,等.应用中断时间序列分析我国“四免一关怀”政策实施前后对艾滋病相关病死率的影响[J].中华流行病学杂志,2020,41(3):406-411.DOI: 10.3760/cma.j.issn.0254-6450.2020.03.024.
|
| [30] |
肖桂真,杨蕾,吴优优,等.中断时间序列分析在基本医疗保险支付方式改革效果评估中的应用研究[J].中国卫生统计,2024,41(3):360-364.DOI: 10.11783/j.issn.1002-3674.2024.03.007.
|
| [31] |
文静,张鹏,曹英南,等.基于中断时间序列分析的髋和膝关节置换术患者住院费用变化趋势研究[J].中国医院管理, 2023, 43(10):42-47.
|
| [32] |
FaginA,PalmieriTL.Considerations for pediatric burn sedation and analgesia[J/OL].Burns Trauma,2017,5:28[2024-06-25]. https://pubmed.ncbi.nlm.nih.gov/29051890/. DOI: 10.1186/s41038-017-0094-8.
|
| [33] |
ReadeMC,FinferS.Sedation and delirium in the intensive care unit[J].N Engl J Med,2014,370(5):444-454.DOI: 10.1056/NEJMra1208705.
|
| [34] |
BaldoBA. Toxicities of opioid analgesics: respiratory depression, histamine release, hemodynamic changes, hypersensitivity, serotonin toxicity[J].Arch Toxicol,2021,95(8):2627-2642. DOI: 10.1007/s00204-021-03068-2.
|
| [35] |
RyanNM,IsbisterGK.Tramadol overdose causes seizures and respiratory depression but serotonin toxicity appears unlikely[J].Clin Toxicol (Phila),2015,53(6):545-550.DOI: 10.3109/15563650.2015.1036279.
|
| [36] |
ParkS, LeeGH, KimS, et al.Risk factors for respiratory depression associated with tramadol based on the Global Pharmacovigilance Database (VigiBase)[J].Pharmaceuticals (Basel),2024,17(2):205. DOI: 10.3390/ph17020205.
|
| [37] |
郭光华,江政英.小儿吸入性损伤[J].中华烧伤杂志,2020,36(4):247-251.DOI: 10.3760/cma.j.cn501120-20191002-00393.
|
| [38] |
HolleyAD, ReadeMC, LipmanJ, et al.There is no fire without smoke! Pathophysiology and treatment of inhalational injury in burns: a narrative review[J].Anaesth Intensive Care,2020,48(2):114-122. DOI: 10.1177/0310057X20913282.
|
| [39] |
郭光华.重度吸入性损伤的呼吸支持与治疗[J].中华烧伤杂志, 2013, 29(2):134-138. DOI: 10.3760/cma.j.issn.1009-2587.2013.02.011.
|
| [40] |
RikerRR,ShehabiY,BokeschPM,et al.Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial[J].JAMA,2009,301(5):489-499.DOI: 10.1001/jama.2009.56.
|
| [41] |
XiaoK,ChenWX,LiXJ.Analysis of risk factors of prolonged mechanical ventilation in patients with severe burn injury[J].Clin Respir J,2023,17(8):791-798.DOI: 10.1111/crj.13673.
|
| [42] |
SchreiberAF, CerianaP, AmbrosinoN, et al.Physiotherapy and weaning from prolonged mechanical ventilation[J].Respir Care,2019,64(1):17-25. DOI: 10.4187/respcare.06280.
|
| [43] |
TrudzinskiFC,NeetzB,BornitzF,et al.Risk factors for prolonged mechanical ventilation and weaning failure: a systematic review[J].Respiration,2022,101(10):959-969.DOI: 10.1159/000525604.
|
| [44] |
RossettiAO, ClaassenJ, GaspardN. Status epilepticus in the ICU[J].Intensive Care Med,2024,50(1):1-16. DOI: 10.1007/s00134-023-07263-w.
|
| [45] |
娄林娟.咪达唑仑用于重症监护患者镇静的效果评价[J].中国药业,2013,22(5):9-10.DOI: 10.3969/j.issn.1006-4931.2013.05.005.
|
| [46] |
GarciaR, SalluhJIF, AndradeTR, et al.A systematic review and meta-analysis of propofol versus midazolam sedation in adult intensive care (ICU) patients[J].J Crit Care,2021,64:91-99. DOI: 10.1016/j.jcrc.2021.04.001.
|
| [47] |
BaarslagMA,AllegaertK,KnibbeCA,et al.Pharmacological sedation management in the paediatric intensive care unit[J].J Pharm Pharmacol,2017,69(5):498-513.DOI: 10.1111/jphp.12630.
|
| [48] |
FaginA,PalmieriT,GreenhalghD,et al.A comparison of dexmedetomidine and midazolam for sedation in severe pediatric burn injury[J].J Burn Care Res,2012,33(6):759-763.DOI: 10.1097/BCR.0b013e318254d48e.
|
| [49] |
LewisK, AlshamsiF, CarayannopoulosKL, et al.Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials[J].Intensive Care Med,2022,48(7):811-840. DOI: 10.1007/s00134-022-06712-2.
|
| [50] |
杨毅,邱海波.镇痛和镇静治疗的进步:从改善患者舒适度到器官功能保护[J].中华内科杂志,2011,50(10):809-811.DOI: 10.3760/cma.j.issn.0578-1426.2011.10.001.
|
| [51] |
VincentJL,ShehabiY,WalshTS,et al.Comfort and patient-centred care without excessive sedation: the eCASH concept[J].Intensive Care Med,2016,42(6):962-971.DOI: 10.1007/s00134-016-4297-4.
|
| [52] |
王桥生,罗琼,蒋志华,等.以eCASH理念为基础的镇静策略对ICU患者的效果[J].中华急诊医学杂志,2021,30(2):226-230.DOI: 10.3760/cma.j.issn.1671-0282.2021.02.017.
|
| [53] |
StollingsJL,BalasMC,ChanquesG.Evolution of sedation management in the intensive care unit (ICU)[J].Intensive Care Med,2022,48(11):1625-1628.DOI: 10.1007/s00134-022-06806-x.
|
| [54] |
ShehabiY,BellomoR,ReadeMC,et al.Early goal-directed sedation versus standard sedation in mechanically ventilated critically ill patients: a pilot study*[J].Crit Care Med,2013,41(8):1983-1991.DOI: 10.1097/CCM.0b013e31828a437d.
|
| [55] |
舒开丽,燕朋波,曹文理,等.早期目标导向型镇静策略对术后机械通气患者的临床效果观察[J].中国中西医结合外科杂志,2023,29(1):34-37.DOI: 10.3969/j.issn.1007-6948.2023.01.007.
|

Figures(2) / Tables(6)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: