- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
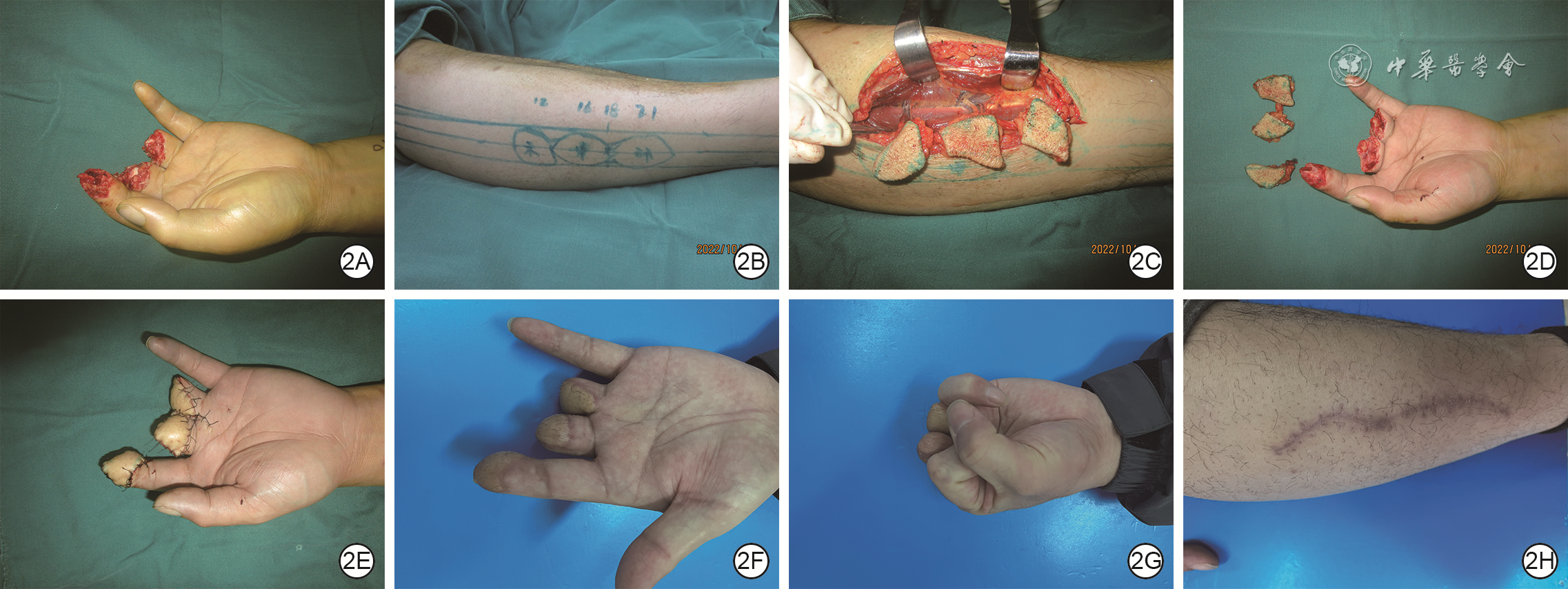
| Citation: | Cheng HY,Ju JH,Zhao Q,et al.Efficacy of free multiple lateral crural perforator flaps from one lower limb under CDU precise localization for repairing multiple wounds at different sites of the finger[J].Chin J Burns Wounds,2026,42(2):182-188.DOI: 10.3760/cma.j.cn501225-20241210-00484.

|

| [1] |
张韬,程俊楠,杨林,等.腓浅动脉穿支双叶皮瓣修复手指相邻2处创面的效果[J].中华烧伤与创面修复杂志,2023,39(7):655-661.DOI: 10.3760/cma.j.cn501225-20220930-00428.
|
| [2] |
JiaoX,CuiC,NgSK,et al.The modified bilobed flap for reconstructing sacral decubitus ulcers[J/OL].Burns Trauma,2020,8:tkaa012[2024-12-10].https://pubmed.ncbi.nlm.nih.gov/33335930/.DOI: 10.1093/burnst/tkaa012.
|
| [3] |
程贺云,巨积辉,赵强,等.游离同侧双蒂双腓浅动脉穿支皮瓣修复同指或邻指2处创面[J].中华显微外科杂志,2022,45(6):608-612.DOI: 10.3760/cma.j.cn441206-20220623-00129.
|
| [4] |
储国平,唐晓钰,蒋朝龙,等.腹部多个宽蒂超薄皮瓣修复多手指创面[J].中华手外科杂志,2022,38(4):277-280.DOI: 10.3760/cma.j.cn311653-20210904-00272.
|
| [5] |
肖媚媚,谢松林,肖湘君.游离骨间后动脉四叶皮瓣联合𧿹甲瓣修复单手5指指背软组织缺损一例[J].中华显微外科杂志,2022,45(5):588-590.DOI: 10.3760/cma.j.cn441206-20220729-00160.
|
| [6] |
王兵,马炬雷,张斌,等.小腿腓动脉穿支皮瓣在𧿹趾缺损修复中的临床应用[J].中华手外科杂志,2024,40(1):26-28.DOI: 10.3760/cma.j.cn311653-20231102-00067.
|
| [7] |
王凯,滕志成,董帅,等.3D打印技术辅助设计游离皮瓣修复虎口挛缩松解术后软组织缺损[J].中华显微外科杂志,2024,47(2):143-147.DOI: 10.3760/cma.j.cn441206-20231129-00090.
|
| [8] |
张韬,杨林,程俊楠,等.游离腓浅动脉穿支皮瓣修复手部热压伤创面的疗效分析研究[J].中华手外科杂志,2023,39(2):132-135.DOI: 10.3760/cma.j.cn311653-20220902-00229.
|
| [9] |
NikiH,AokiH,InokuchiS,et al.Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders I: development of standard rating system[J]. J Orthop Sci,2005,10(5):457-465.DOI: 10.1007/s00776-005-0936-2.
|
| [10] |
肖飞鹏,柳志锦,刘胜哲,等.综合评价量表在股前外侧皮瓣修复术后疗效评价中的应用[J].中国美容整形外科杂志,2021,32(6):348-351.DOI: 10.3969/j.issn.1673-7040.2021.06.010.
|
| [11] |
李海,常树森,魏在荣,等.联合指端动脉弓的指固有血管神经束V-Y推进皮瓣修复儿童指端小面积皮肤软组织缺损[J].中华手外科杂志,2020,36(4):250-252.DOI: 10.3760/cma.j.cn311653-20200224-00063.
|
| [12] |
孙旭,殷宗琦,郑捷新,等.基于指动脉背侧支供血的蝶形皮瓣与螺旋桨皮瓣修复手指掌侧创面疗效的对比研究[J].中华烧伤与创面修复杂志,2023,39(6):552-557.DOI: 10.3760/cma.j.cn501225-20220714-00294.
|
| [13] |
杨焕友,王斌,李瑞国,等.吻合血管的第二掌背动脉皮瓣修复手指掌侧皮肤伴双侧指固有神经、动脉缺损[J].中华手外科杂志,2021,37(1):10-12.DOI: 10.3760/cma.j.cn311653-20200303-00094.
|
| [14] |
王凯,金光哲,滕志成,等.游离血流与神经桥接型第2趾胫侧皮瓣治疗近指间关节重度屈曲挛缩的效果[J].中华烧伤与创面修复杂志,2023,39(8):765-770.DOI: 10.3760/cma.j.cn501225-20220707-00286.
|
| [15] |
李海建,李甲,闫成士,等. 应用双足𧿹趾腓侧游离皮瓣同期修复双手指远节指腹缺损[J]. 中华手外科杂志,2023,39(2):129-131. DOI: 10.3760/cma.j.cn311653-20221007-00262.
|
| [16] |
武海波,金光哲,李锦,等.第1跖背动脉终末支皮瓣修复手指皮肤软组织缺损的效果[J].中华烧伤与创面修复杂志,2024,40(10):963-970.DOI: 10.3760/cma.j.cn501225-20231226-00271.
|
| [17] |
张伟,程芳斌,刘刚义,等.游离𧿹趾腓侧皮瓣移植修复指腹缺失的临床体会[J].中华手外科杂志,2022,38(3):241-242.DOI: 10.3760/cma.j.cn311653-20211108-00326.
|
| [18] |
周健辉,石惠文,冷树立,等.𧿹趾腓侧折叠皮瓣修复拇指全指腹缺损[J].中华手外科杂志,2023,39(2):176-178.DOI: 10.3760/cma.j.cn311653-20220905-00230.
|
| [19] |
李甲,裴广楠,朱辉,等.游离𧿹趾腓侧皮瓣与足底内侧皮瓣在修复指腹创面中的疗效比较[J].中华手外科杂志,2023,39(1):33-37.DOI: 10.3760/cma.j.cn311653-20211210-00363.
|
| [20] |
ChanJK, SongM, ShirleyR, et al. Free dorsal toe flap for reconstruction of the hallux[J]. Plast Reconstr Surg Glob Open,2020,8(9):e3117.DOI: 10.1097/GOX.0000000000003117.
|
| [21] |
程贺云,巨积辉,赵强,等.游离腓浅动脉穿支皮瓣修复手部中小面积热压伤创面的效果[J].中华烧伤与创面修复杂志,2023,39(6):546-551.DOI: 10.3760/cma.j.cn501225-20220623-00256.
|
| [22] |
李友,唐林峰,熊胜,等.游离多块小腿前外侧穿支皮瓣一期修复单手多指创面[J].中华显微外科杂志,2024,47(3):307-311.DOI: 10.3760/cma.j.cn441206-20230909-00031.
|
| [23] |
郭全伟,赵强,程贺云,等.游离小腿同一供区多块腓浅动脉穿支皮瓣修复手部多处热压伤狭长创面的效果观察[J].中华手外科杂志,2024,40(4):356-359.DOI: 10.3760/cma.j.cn311653-20231207-00095.
|
| [24] |
StoccoC, MurphyDC, GargiuloM, et al. Superficial peroneal nerve accessory artery (SPNAA) flap for head and neck reconstruction: a cadaveric anatomical study and retrospective case series review[J]. J Plast Reconstr Aesthet Surg,2020,74(7):1524-1533.DOI: 10.1016/j.bjps.2020.11.012.
|
| [25] |
张韬,程俊楠,杨林,等.多穿支腓浅动脉穿支皮瓣修复手足创面的疗效[J].中华烧伤与创面修复杂志,2023,39(3):234-240.DOI: 10.3760/cma.j.cn501225-20220723-00305.
|
| [26] |
程贺云,巨积辉,赵强,等.腓浅动脉穿支皮瓣在拇指和手指瓦合再造术中的临床应用[J].中华显微外科杂志,2023,46(6):631-636.DOI: 10.3760/cma.j.cn441206-20230714-00120.
|
| [27] |
张韬,杨林,程俊楠,等.“ABC”三线定位穿支方法在游离小腿前外侧穿支皮瓣的应用[J].中华显微外科杂志,2023,46(1):70-75.DOI: 10.3760/cma.j.cn441206-20220530-00107.
|
| [28] |
周飞亚,张弦,蔡乐益,等.精准定位的微型股前外侧穿支皮瓣修复手指中等面积皮肤软组织缺损的效果[J].中华烧伤与创面修复杂志,2024,40(2):165-171.DOI: 10.3760/cma.j.cn501225-20231030-00150.
|
| [29] |
林伟栋,黄海,施海峰,等.股前外侧区红外热点复温速度与浅筋膜内分支解剖情况的相关性研究[J].中华手外科杂志,2025,41(1):63-66.DOI: 10.3760/cma.j.cn311653-20240704-00185.
|
| [30] |
肖栋超,潘佳栋,周贤挺,等.止血带控制再灌注增强红外热成像术辅助设计腓肠内侧动脉穿支皮瓣的临床应用[J].中华整形外科杂志,2023,39(12):1324-1330.DOI: 10.3760/cma.j.cn114453-20230704-00145.
|
| [31] |
孙艺然,陈勇,王倩,等.DSA联合多普勒超声辅助下胫后动脉穿支皮瓣修复小腿下段软组织缺损[J].组织工程与重建外科,2023,19(5):446-449.DOI: 10.3969/j.issn.1673-0364.2023.05.003.
|
| [32] |
张海钰,仲海燕,陈勇,等.腓肠内、外侧动脉的DSA观察及其在皮瓣移植中的应用[J].组织工程与重建外科,2025,21(2):119-124.DOI: 10.3969/j.issn.1673-0364.2025.02.002.
|
| [33] |
蓝波,傅尚俊,刘涛,等.CTA三维重建技术在游离双叶股前外侧穿支皮瓣移植修复四肢创面中的效果[J].中华医学美学美容杂志,2025,31(2):148-154.DOI: 10.3760/cma.j.cn114657-20241206-00207.
|
| [34] |
董帅,王石,滕志成,等.吲哚菁绿血管造影在皮瓣穿支定位中的应用[J].中华手外科杂志,2025,41(1):46-51.DOI: 10.3760/cma.j.cn311653-20240629-00181.
|
| [35] |
李昌松,李雷,周正虎,等.3D数字减影血管造影联合彩色多普勒超声穿支血管定位技术在股前外侧穿支皮瓣修复小腿创面中的临床应用[J/OL].中华损伤与修复杂志(电子版),2025,20(1):7-12[2025-08-02]. https://rs.yiigle.com/cmaid/1571441.DOI: 10.3877/cma.j.issn.1673-9450.2025.01.002.
|
| [36] |
李贤海,周建东,郑杰,等.红外热成像结合高频彩色多普勒超声定位浅筋膜穿支在超薄股前外侧皮瓣切取中的应用[J].中华显微外科杂志,2024,47(6):635-640.DOI: 10.3760/cma.j.cn441206-20240205-00041.
|
| [37] |
李建杭,赵军,陈裕祥,等.高频彩色多普勒超声辅助定位在修薄穿支皮瓣移植术中的临床疗效[J].中华显微外科杂志,2024,47(6):679-685.DOI: 10.3760/cma.j.cn441206-20240402-00091.
|
| [38] |
张宇轩,许亚军,周建东,等.宽频线阵容积探头引导下三维超声技术在股前外侧穿支皮瓣术前穿支定位中的应用[J].中华显微外科杂志,2024,47(1):17-21.DOI: 10.3760/cma.j.cn441206-20230815-00015.
|
 程贺云 2月2日.mp4
程贺云 2月2日.mp4
|

|

Figures(3)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: