- Medline/PubMed数据库
- Scopus数据库
- PMC数据库
- CSCD
- 北大核心收录期刊
- 统计源期刊
- 我国高质量科技期刊T1级
- 第6届中国精品科技期刊
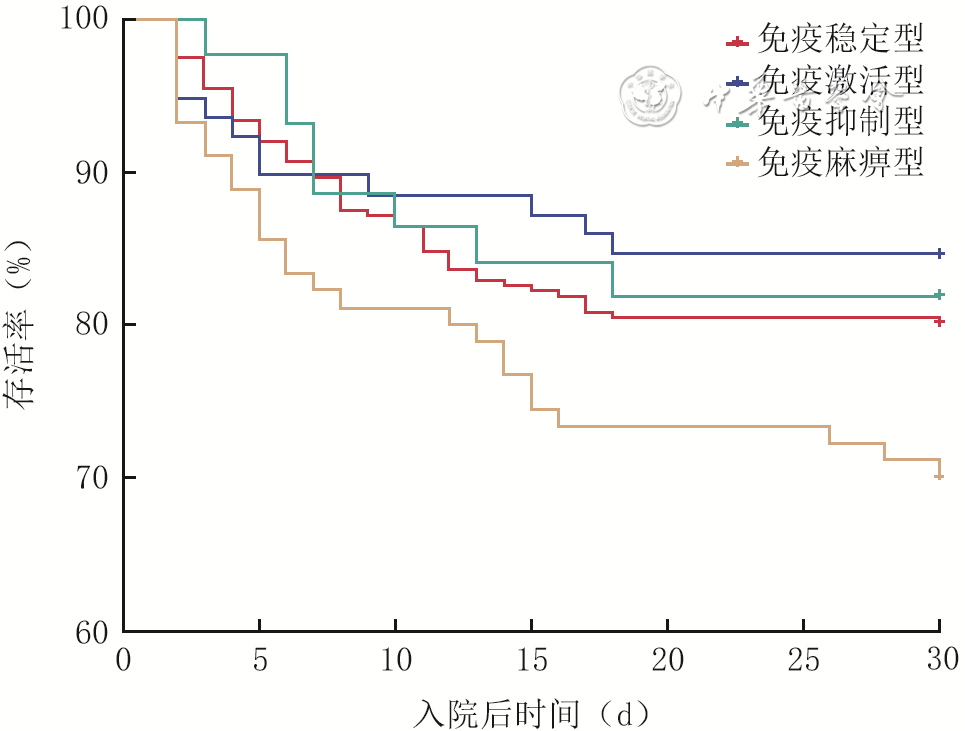
| Citation: | Hong DJ,Zeng WT,Wang W,et al.Latent profile analysis of the relationship between immune subtypes in sepsis patients and response to glucocorticoid treatment and prognosis[J].Chin J Burns Wounds,2026,42(2):153-162.DOI: 10.3760/cma.j.cn501225-20251030-00451.

|

| [1] |
SingerM,DeutschmanCS,SeymourCW,et al.The third international consensus definitions for sepsis and septic shock (Sepsis-3)[J].JAMA,2016,315(8):801-810.DOI: 10.1001/jama.2016.0287.
|
| [2] |
LiY,ZhangH,ChenC,et al.Biomimetic immunosuppressive exosomes that inhibit cytokine storms contribute to the alleviation of sepsis[J].Adv Mater,2022,34(19):e2108476.DOI: 10.1002/adma.202108476.
|
| [3] |
姚咏明,张卉.改善脓毒症患者长期预后的康复治疗对策[J].中华烧伤与创面修复杂志,2022,38(3):201-206.DOI: 10.3760/cma.j.cn501120-20211004-00344.
|
| [4] |
Fleischmann-StruzekC,RuddK.Challenges of assessing the burden of sepsis[J].Med Klin Intensivmed Notfmed,2023,118(Suppl 2):S68-S74.DOI: 10.1007/s00063-023-01088-7.
|
| [5] |
SeymourCW,GomezH,ChangCH,et al.Precision medicine for all? Challenges and opportunities for a precision medicine approach to critical illness[J].Crit Care,2017,21(1):257.DOI: 10.1186/s13054-017-1836-5.
|
| [6] |
WangW,LiuCF.Sepsis heterogeneity[J].World J Pediatr,2023,19(10):919-927.DOI: 10.1007/s12519-023-00689-8.
|
| [7] |
WiersingaWJ,van der PollT.Immunopathophysiology of human sepsis[J].EBioMedicine,2022,86:104363.DOI: 10.1016/j.ebiom.2022.104363.
|
| [8] |
ZhangZ,AbardaA,ContractorAA,et al.Exploring heterogeneity in clinical trials with latent class analysis[J].Ann Transl Med,2018,6(7):119.DOI: 10.21037/atm.2018.01.24.
|
| [9] |
KempkerJA,MartinGS.The changing epidemiology and definitions of sepsis[J].Clin Chest Med,2016,37(2):165-179.DOI: 10.1016/j.ccm.2016.01.002.
|
| [10] |
马帅,郭树彬.脓毒症免疫麻痹与细胞免疫调理治疗研究进展[J].中华急诊医学杂志,2016,25(7):969-973.DOI: 10.3760/cma.j.issn.1671-0282.2016.07.027.
|
| [11] |
裴飞,吴健锋.脓毒症免疫调理治疗研究进展[J].中华医学信息导报,2021,36(21):19.DOI: 10.3760/cma.j.issn.1000-8039.2021.21.127.
|
| [12] |
姚咏明,栾樱译.严重烧创伤感染及其并发症的免疫新认识[J].中华烧伤杂志,2021,37(6):519-523.DOI: 10.3760/cma.j.cn501120-20210118-00025.
|
| [13] |
WuY,WangL,LiY,et al.Immunotherapy in the context of sepsis-induced immunological dysregulation[J].Front Immunol,2024,15:1391395.DOI: 10.3389/fimmu.2024.1391395.
|
| [14] |
胡荣华,郑颜磊,程飞,等.脓毒症精准免疫治疗的新进展[J].中国中西医结合急救杂志,2019,26(4):504-506.DOI: 10.3969/j.issn.1008-9691.2019.04.036.
|
| [15] |
权震,温良鹤,郑俊波,等.脓毒症免疫抑制机制及治疗策略[J].中国急救医学,2024,44(1):25-29.DOI: 10.3969/j.issn.1002-1949.2024.01.005.
|
| [16] |
彭海伦,赵月丽,徐崇孝,等. 成人脓毒症分型研究进展[J]. 解放军医学杂志,2023,48(9):1107-1112. DOI: 10.11855/j.issn.0577-7402.1426.2022.0915.
|
| [17] |
姚咏明,张卉,董宁.脓毒症分型:精准治疗之基石[J].中华烧伤与创面修复杂志,2024,40(10):915-919.DOI: 10.3760/cma.j.cn501225-20240529-00203.
|
| [18] |
CaoM,WangG,XieJ.Immune dysregulation in sepsis: experiences, lessons and perspectives[J].Cell Death Discov,2023,9(1):465.DOI: 10.1038/s41420-023-01766-7.
|
| [19] |
LiuZ,TingY,LiM,et al.From immune dysregulation to organ dysfunction: understanding the enigma of Sepsis[J].Front Microbiol,2024,15:1415274.DOI: 10.3389/fmicb.2024.1415274.
|
| [20] |
魏启美,修光辉.人工智能在脓毒症早期诊断及预测中应用的研究进展[J].中华危重病急救医学,2022,34(11):1218-1221.DOI: 10.3760/cma.j.cn121430-20220628-00611.
|
| [21] |
SpurkD,HirschiA,WangM,et al.Latent profile analysis: a review and “how to” guide of its application within vocational behavior research[J].J Vocat Behav,2020,120:103445. DOI: 10.1016/j.jvb.2020.103445.
|
| [22] |
RhodesA,EvansLE,AlhazzaniW,et al.Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016[J].Intensive Care Med,2017,43(3):304-377.DOI: 10.1007/s00134-017-4683-6.
|
| [23] |
FraleyC,RafteryAE.How many clusters? Which clustering method? Answers via model-based cluster analysis[J].Comput J,1998,41(8):578-588.DOI: 10.1093/comjnl/41.8.578.
|
| [24] |
TsukamotoH,FujiedaK,SenjuS,et al.Immune-suppressive effects of interleukin-6 on T-cell-mediated anti-tumor immunity[J].Cancer Sci,2018,109(3):523-530.DOI: 10.1111/cas.13433.
|
| [25] |
SeymourCW,KennedyJN,WangS,et al.Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis[J].JAMA,2019,321(20):2003-2017.DOI: 10.1001/jama.2019.5791.
|
| [26] |
SongJ,ParkDW,MoonS,et al.Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: a prospective controlled study according to the Sepsis-3 definitions[J].BMC Infect Dis,2019,19(1):968.DOI: 10.1186/s12879-019-4618-7.
|
| [27] |
马跃,傅斌清,魏海明.脓毒症的过度炎症反应与免疫抑制[J].中华微生物学和免疫学杂志,2025,45(3):190-197.DOI: 10.3760/cma.j.cn112309-20250122-00025.
|
| [28] |
ZhangX,ZhangY,YuanS,et al.The potential immunological mechanisms of sepsis[J].Front Immunol,2024,15:1434688.DOI: 10.3389/fimmu.2024.1434688.
|
| [29] |
BarriosEL,MazerMB,McGonagillPW,et al.Adverse outcomes and an immunosuppressed endotype in septic patients with reduced IFN-γ ELISpot[J].JCI Insight,2024,9(2):e175785.DOI: 10.1172/jci.insight.175785.
|
| [30] |
PitreT,DroverK,ChaudhuriD,et al.Corticosteroids in sepsis and septic shock: a systematic review, pairwise, and dose-response meta-analysis[J].Crit Care Explor,2024,6(1):e1000.DOI: 10.1097/CCE.0000000000001000.
|
| [31] |
孙玉景,吴建华,任建国,等.糖皮质激素在脓毒症治疗中研究进展[J].中国老年学杂志,2022,42(17):4365-4369.DOI: 10.3969/j.issn.1005-9202.2022.17.058.
|
| [32] |
HemingN,SivanandamoorthyS,MengP,et al.Immune effects of corticosteroids in sepsis[J].Front Immunol,2018,9:1736.DOI: 10.3389/fimmu.2018.01736.
|
| [33] |
KobbeP,BläsiusFM,LichteP,et al.Neuroendocrine modulation of the immune response after trauma and sepsis: does it influence outcome?[J].J Clin Med,2020,9(7):2287.DOI: 10.3390/jcm9072287.
|
| [34] |
YangZ,GaoY,ZhaoL,et al.Molecular mechanisms of Sepsis attacking the immune system and solid organs[J].Front Med (Lausanne),2024,11:1429370.DOI: 10.3389/fmed.2024.1429370.
|
| [35] |
KudoD,GotoT,UchimidoR,et al.Coagulation phenotypes in sepsis and effects of recombinant human thrombomodulin: an analysis of three multicentre observational studies[J].Crit Care,2021,25(1):114.DOI: 10.1186/s13054-021-03541-5.
|
| [36] |
宋景春,丁仁彧,吕奔,等. 脓毒症性凝血病诊疗中国专家共识(2024版)[J]. 解放军医学杂志,2024,49(11):1221-1236. DOI: 10.11855/j.issn.0577-7402.1189.2024.0918.
|
| [37] |
PeiF,YaoRQ,RenC,et al.Expert consensus on the monitoring and treatment of sepsis-induced immunosuppression[J].Mil Med Res,2022,9(1):74.DOI: 10.1186/s40779-022-00430-y.
|
 洪德江.mp4
洪德江.mp4
|

|

Figures(2) / Tables(7)
Copyright © Chinese Journal of Burns京ICP备07035254号-14
E-mail:shaoshangzazhi@163.com
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: